
Abstract
Purpose:
The systemic and ocular pharmacokinetics (PK), and ocular toxicity of benzalkonium chloride (BAK)-free TearClear latanoprost ophthalmic solution, 0.005% formulation (TC-002) were evaluated. TC-002 is designed to selectively capture BAK at the time of drug administration; therefore, the dose delivered to the eye contains no quantifiable level of preservative.
Methods:
The systemic and ocular PK of TC-002 were compared to a BAK containing reference listed drug (RLD, Xalatan™) over a 24-h period, after a single topical ocular dose to 1 eye of male Dutch Belted (DB) rabbits (n = 3/timepoint). Latanoprost acid concentrations were measured in plasma and ocular tissues. The ocular toxicity was evaluated in a separate study and included toxicokinetic evaluation of TC-002 after once daily topical ocular dosing into each eye of DB rabbits (n = 8/group) for at least 28 days. Toxicity endpoints included ophthalmic and clinical evaluations, necropsy, and microscopic evaluation of ocular tissues.
Results:
Average ratios of Cmax values for TC-002/RLD ranged from 0.6 to 1.6, and Cmax and area under the concentration-time curve of last observed concentration (AUClast) exposures to latanoprost acid were similar (<2-fold) between the 2 treatments. In the 28-day study, the Tmax was achieved in both groups in <0.5 h. There were no abnormal ocular findings.
Conclusions:
TC-002 with no quantifiable preservative or BAK-containing RLD exhibited similar ocular and systemic PK profiles. TC-002 was well tolerated and comparable to RLD. TC-002 retains the safety and PK characteristics of RLD without the added concern of long-term exposure of the eye to preservatives.
Introduction
Most topical intraocular pressure (IOP)-lowering medications contain preservatives with benzalkonium chloride (BAK) being the most common.1–5 BAK is a quaternary ammonium compound with detergent-like properties. 6 It is an effective agent for preventing microbial growth in multiuse medication bottles and has been approved as part of the formulation by most regulatory bodies for this purpose for several decades.7,8 However, due to the nature of glaucoma, topical medications are dosed long term, chronically exposing the ocular surface to BAK, which can lead to adverse effects. 7 The agent disrupts metabolic process in microbial cells and causes cell lysis leading to death. 9 BAK concentrations in topical glaucoma medications typically range in concentrations from 0.004% to 0.1%. 10 Lower concentrations of BAK in topical glaucoma formulations are associated with less damage to the cornea and conjunctiva. 11 It follows that topical glaucoma formulations with low or no BAK when they are administered could be expected contribution to the preservation of ocular surface health. 11
Ocular surface disease is common among glaucoma patients chiefly due to the preservatives, such as BAK, contained in their topical medication formulations.1,3,12 A higher prevalence of dry eye symptoms has been observed in studies of patients taking ocular hypotensive drops compared with healthy controls.13–15 Positive correlations have been shown between the number of topical ocular hypotensive medications and the severity of the signs and symptoms of ocular surface disease.1,16–19
Adverse effects on conjunctival staining, 13 corneal and conjunctival sensitivity,20,21 corneal clarity, 22 Schirmer test scores,13,23–26 tear film break-up time,13,23–25 Ocular Surface Disease Index scores,17,18,24,25,27 ocular redness,28,29 lipid layer thickness, 30 and tear osmolarity,26,27 have been demonstrated in patients on topical glaucoma medications. 1 While the dose–response for preservative effectiveness is known (generally 0.005% to 0.03% is used in marketed ophthalmic products), the dose–response for untoward effects is not. For example, in a chronic ocular toxicology study in rabbits and monkeys, there was no toxicity (clinical or histopathological) observed with 0.005% to 0.01% benzalkonium eyedrops given from twice- to eight-times daily. 31 Nonetheless, based upon studies noted, reduction of BAK is desirable.
A new multidose product has been designed to reduce BAK from the topical formulation immediately before drop instillation, thus preserving the medication in the bottle while virtually eliminating BAK from the eyedrop that is delivered to the ocular surface. 32 The TearClear design consists of a conventional opthalmic multidose bottle with a proprietary tip filled with a polymer hydrogel that has high affinity for BAK. During drop administration, the formulation passes through the tip and is bound by the hydrogel to ensure that the concentration of BAK in the dispensed drop is below the limit of quantitation (0.9 ng/mL).
The current studies compared 0.005% latanoprost [either TearClear (TC-002) or Xalatan® (reference listed drug (RLD)-latanoprost, RLD-LAT, Lot number AW332, expiration date February 2022)] and were conducted in 2 parts: A single dose 24-h pharmacokinetics (PK) study was conducted that examined latanoprost acid levels in plasma, aqueous humor, cornea, iris/ciliary body (ICB), conjunctiva, lens, vitreous, neurosensory retina, choroid/retinal pigment epithelium (RPE) complex, optic nerve, and sclera. A 28-day study was conducted to evaluate the ocular tolerability and PK of once-daily administration. The Dutch Belted (DB) rabbit was chosen as the animal model for these studies because it is considered to be an accepted pigmented species for nonclinical testing through the ocular route by regulatory agencies. In addition, the DB rabbit was used previously in preclinical studies with the innovator latanoprost product.33,34
The current studies were designed to support the further clinical development of TC-002 and a Phase 3 prospective, double masked, randomized, multicenter, active-controlled, parallel group 3-month CLEAR trial, which evaluated the efficacy and safety of TC-002 in patients with elevated IOP. Demonstrating comparable PK data with TC-002 to the marketed product, Xalatan supports the large existing amount of safety data with the active pharmaceutical ingredient. Therefore, Phase 1 and 2 human studies were not required.
Methods
Drug product/test agents
The TearClear drug product consists of a conventional ophthalmic bottle with a proprietary tip filled with a polymer hydrogel that has a high affinity for the BAK preservative. When the bottle is squeezed to dispense an eye drop, the liquid formulation passes through the tip and BAK is bound by the hydrogel contained within the tip. This reduces the concentration of BAK in the dispensed drop to a negligible level (eg, below the limit of quantitation, 0.9 mg/mL). The analytical method for determination of BAK is provided in Table 1. The test articles were TearClear Latanoprost Ophthalmic Solution, 0.005% [TC-002; containing 0.0157% BAK (Single Dose PK Study) or 0.0175% BAK (28-day Repeat Dose Tolerability Study)] and the comparator RLD (0.005% RLD-latanoprost; RLD-LAT; containing 0.02% BAK).
Summary of Analytical Method Parameters for Benzalkonium Chloride Assay in TC-002
BAK, benzalkonium chloride.
The concentration of both latanoprost and BAK for TC-002 was stable over a 28-day simulated use study. The drop size for TC-002 was 40 μL. Each drop of Xalatan contains 1.5 μg, which converts to a drop size of 30 μL (Xalatan Package Insert, 2011).
Animal welfare (both studies)
The procedures used were reviewed and approved by the iuvo BioScience Institutional Animal Care and Use Committee. The study designs complied with all applicable sections of the Final Rules of the Animal Welfare Act regulations (Code of Federal Regulations, Title 9), the Guide for the Care and Use of Laboratory Animals from the National Research Council, and the Association for Research in Vision and Ophthalmology statement for use of animals in ophthalmic and vision research.
Single dose PK study
Animals were assigned to groups by an allocation scheme based on body weight to a single dose (1 drop) of either 0.005% TC-002 or RLD-LAT. Three animals per PK timepoint—0.25, 0.5, 1, 2, 4, 8, and 24 h (42 total animals) were used. Latanoprost free acid concentrations were measured in plasma and the aqueous humor, cornea, ICB, conjunctiva, lens, vitreous, neurosensory retina, choroid/RPE complex, optic nerve (including optic nerve head), and sclera of the eye.
Housing and food (both studies)
Rabbits were individually housed at 16°C–22°C, 30%–70% humidity, under 12-h light/12-h dark cycle. The animals were provided 100–125 g daily of 5325 Certified High Fiber Rabbit Diet (Purina, Neenah, WI) and ad libitum water through an automatic watering system.
In-life observations
Body weights were obtained before dosing on day 1. All animals were given a general health check at least once daily. Ophthalmic examinations, including slit-lamp examinations with fluorescein staining (McDonald-Shadduck scoring), were performed the day before dosing. 35
Blood collection
Blood (1.0 mL) was collected once per animal at 0.25, 0.5, 1, 2, 4, 8, and 24 h postdose using the central ear artery or marginal ear vein. Sodium fluoride and potassium oxalate were used for anticoagulation, and the samples were maintained on wet ice before and after centrifugation. Samples were centrifuged within 30 min of collection at 5,000 rpm for 10 min under refrigerated conditions. The resulting plasma was harvested, placed in standard cryotubes, and stored in a freezer, set to maintain −70°C ± 10°C until ready for shipment.
Ocular tissue collection
Immediately after the blood collection (at 0.25, 0.5, 1, 2, 4, 8, and 24 h), animals were euthanized by an overdose of sodium pentobarbital and the ocular tissues harvested. Aqueous humor was aspirated immediately postmortem. The frozen technique (liquid nitrogen) was used for remaining tissues of the globe 36 : Cornea, ICB, conjunctiva, lens, vitreous, neurosensory retina, choroid/RPE complex, optic nerve (including optic nerve head), and sclera. Tissue samples were stored in cryotubes in a −70°C ± 10°C freezer until ready for shipment. The plasma and ocular tissue samples from the right eye of each animal were shipped overnight on dry ice to the bioanalytical laboratory. The systemic and ocular bioanalysis was conducted at Inotiv Labs (Maryland Heights, MO).
PK analysis
Latanoprost free acid was measured in tissues following developed and qualified LC-MS/MS methods (Data on File, Inotiv Internal Report 1656–221920NJ, 2022). Pharmacokinetic parameters for each dose group (sparse sampling) were estimated using Phoenix WinNonlin (Version 8.1 or later) PK software. A noncompartmental approach consistent with the ocular route of administration was used for parameter estimation. The following PK parameters were generated from latanoprost acid concentrations in plasma, aqueous humor, cornea, and ICB, whenever practical: the time of observed maximum concentration (Tmax), maximum observed concentration (Cmax), area under the concentration-time curve of last observed concentration (AUClast), area under the concentration-time curve from zero to infinity (AUCinf), and terminal elimination half-life (T1/2). Typically changes 2-fold or greater would represent a true reliable difference, and changes <2-fold suggest that the compounds are similar.
Twenty-eight-day repeat dose tolerability study
Healthy naive male and female DB rabbits were assigned to the 2 treatment groups (n-8/group). They received once-daily treatment in both eyes.
In-life observations
Body weights were obtained before dosing on day 1 and just before euthanasia. Food consumption was qualitatively assessed daily. The study animals were observed once daily predose and then weekly for changes in the skin, fur, eyes and mucous membranes, respiratory system, circulatory system, autonomic central nervous system, somatomotor activity, locomotor activity, and behavioral patterns.
Ophthalmic examinations, including slit-lamp examinations with fluorescein staining (McDonald-Shadduck scoring) and indirect ophthalmoscopy (with dilation), were performed by a board-certified veterinary ophthalmologist predose and on days 1 and 7, ∼2 h ± 30 min postdosing. 35
IOP measurements were taken using Tono-vet predose, day 1 of dosing, and then weekly. These measurements were taken approximately the same time each day (9:30 to 10:40 AM) at 1 h ± 15 min after dosing. At least 3 readings were taken per eye, and the mean was recorded. Draize testing was performed 15–30 min after dosing. Behavioral observations suggestive of ocular irritation, such as squinting or pawing, were noted. Slit-lamp examinations with fluorescein staining (McDonald-Shadduck scoring) were conducted by study personnel on days 9, 16, and 21 to monitor general ocular health. One milliliter of blood was collected once per animal predose and on days 1 and 27 at 0.25, 0.5, 1, 2, 6, and 24 h postdose using the central ear artery. The PK analysis was performed as previously described.
Euthanasia and necropsy
At the end of the study (and at least 28 days of dosing), the study animals were euthanized by an overdose of sodium pentobarbital. All study animals underwent a limited necropsy examination, which included an evaluation of all external surfaces, including the eye and eyelids. Ocular tissues were collected at necropsy.
Pathology
Microscopic evaluation of slides from all animals was evaluated by a board-certified veterinary pathologist. The microscopic evaluation provided a thorough histopathological evaluation of 5 sections of the eye, as well as the eyelid, Harderian gland, lacrimal gland, and optic nerve, according to the methodology described by Booler et al. 37
Statistics
Statistical analysis was conducted using Minitab® (Minitab, LLC, State College, PA) statistical software (Version 19.2). For inferential analyses, normally distributed data were analyzed by appropriate parametric methods (eg, unpaired t-test or analysis of variance with appropriate post hoc test, if necessary). Non-normally distributed data were analyzed by appropriate nonparametric methods (eg, Mann–Whitney or Kruskal–Wallis with appropriate post hoc test, if necessary). Differences were considered statistically significant if P ≤ 0.05. Body weights, body weight changes, and mean IOP values were analyzed using inferential analyses. As this was primarily a safety study, no correction for multiplicity was made. Gross ocular observation scores and toxicokinetic parameters were analyzed using descriptive statistics. Other clinical observations and indirect ophthalmoscopy were evaluated using an observed count. The study was designed following ICH M3 principles for nonclinical studies in terms of animal numbers and other parameters. In keeping with animal welfare principles to meet the objectives, the study was not powered per se to claim noninferiority.
Results
Single-dose PK study
In-life observations
All animals used in this study were healthy at predose and over the course of the study. Mean body weights were similar for the 2 groups (1.77 and 1.78 kg for the TC-002 and for the RLD-LAT groups, respectively). Ophthalmic examinations showed that all eyes were normal at predose, with McDonald-Shadduck scores of 0 for all parameters.
Pharmacokinetics
Latanoprost acid was quantifiable in the aqueous and vitreous humor and tissues but not in any of the plasma samples. Latanoprost acid was quantifiable from 0.25 h through 0.5 h (optic nerves), 4 h (choroid and sclera), 8 h (aqueous humor, conjunctiva, and ICB), and 24 h (cornea) and in the lens at 0.5 and 1 h postdose. Time to peak concentrations (Tmax) occurred at 0.25 h (choroid, conjunctiva, cornea, optic nerve, retina, and sclera), 0.5 h (lens), and 1 h (aqueous and vitreous humors and ICB) postdose (Figs. 1 and 2). Where PK parameters could be calculated, peak (Cmax) and total (AUClast) exposures to latanoprost free acid in the eyes were highest in the cornea and the lowest in the vitreous humor (Table 2). Following a single topical dose of the 2 formulation, Cmax and AUClast exposures to latanoprost free acid were similar between the 2. The differences in Cmax and AUClast between the 2 formulations ranged from 0.6- to 1.6-fold (Table 3).
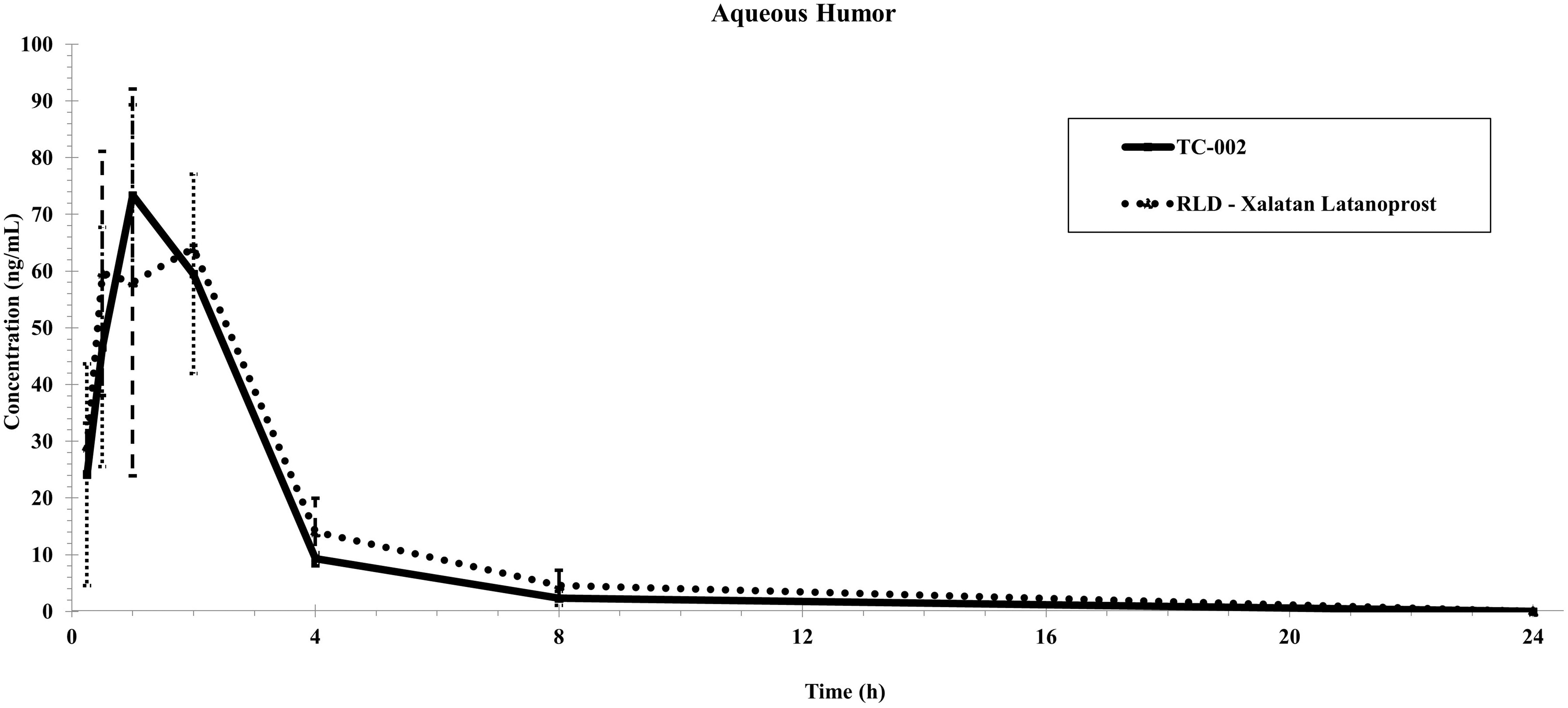
Latanoprost concentration over time: aqueous humor (mean ± s.e.m., ng/mL). RLD, reference listed drug; s.e.m., standard error of the mean.

Latanoprost concentration over time: iris-ciliary body (mean ± s.e.m., ng/mL).
Pharmacokinetic Parameters Following a Single Topical Ocular Administration of 0.005% TC-002 or RLD-Xalatan Latanoprost to Male Dutch Belt Rabbits Analyte Latanoprost Free Acid
AUClast, area under the concentration-time curve of last observed concentration; Cmax, maximum observed concentration; RLD, reference listed drug; SE, standard error; T1/2, terminal elimination half-life; Tmax, the time of observed maximum concentration.
Fold Differences in Latanoprost Free Acid Cmax and AUClast Values
Ratios were calculated as TC-002/RLD.
NA, not applicable.
Twenty-eight-day repeat dose tolerability study
In-life observations
No drug-related abnormal clinical observations were reported. There were no statistically significant differences between the treatment groups in weight gain. All animals gained weight over the course of the study. There were no abnormal food consumption findings. Ophthalmic examinations, including slit lamp evaluation with fluorescein staining and indirect ophthalmoscopy, showed that all eyes in both groups were normal at predose and on day 1 and 27. IOP measurements were not significantly different between the 2 groups at any time point (predose, day 1, week 1, week 2, week 3, and week 4, Table 4).
Mean Intraocular Pressure Values
N = 4 for all timepoints.
IOP, intraocular pressure; OD, right eye; OS, left eye; SD, standard deviation.
Ocular health as assessed using the Draize scoring system showed no scores above zero in either group.
Bioanalysis
Latanoprost acid was detectable (≥0.05 ng/mL) in the plasma of TC-002-treated males up to 4 h postdose administration on day 1 (n = 2 of 4 at 4 h), whereas in the TC-002-treated females, latanoprost acid was detectable up to 0.5 h postdose administration (n = 4 of 4 at 0.5 h). On day 27, latanoprost acid was detectable in the plasma of both male and female TC-002-treated animals up to 1 h postdose administration (n = 3 of 4 males; n = 4 of 4 females). Plasma concentrations of latanoprost acid were below the lower limit of quantitation (LLOQ) of the method for all remaining time points for male and female TC-002 treated groups, respectively, on day 1 and 27.
Latanoprost acid was detectable in the plasma of RLD-treated males and females up to 0.25 h postdose administration on day 1 (n = 4 of 4 males; n = 4 of 4 females at 0.25 h). Only 1 RLD-treated female had a detectable plasma concentration of latanoprost acid at the 0.5 h time point on day 1. On day 27, latanoprost acid was detectable in the plasma of both male and female RLD-LAT-treated animals up to 0.5 h postdose administration (n = 2 of 4 males; n = 2 of 4 females). Only 1 RLD-treated male had a detectable plasma concentration of latanoprost acid at the 1 h time point on day 27. Concentrations of latanoprost acid were below the LLOQ for all remaining time points for both male and female RLD-LAT-treated groups on day 1 and 27.
Toxicokinetics
No sex-based differences were observed in the latanoprost acid Tmax, Cmax,or AUClast for either of the 2 formulations evaluated on day 1 or Day. 27 A Tmax of 0.25 h, the first collection timepoint, was noted for both formulations on day 1 and 27 regardless of sex. There were differences in systemic exposure between the 2 latanoprost formulations. Cmax and AUClast for latanoprost acid following TC-002 administration were greater than for RLD-LAT on day 1 and 27 in both males and females. The Cmax for TC-002 was ∼1.4- to 2-fold greater than that for RLD-LAT. In general, AUClast was ∼1.6- to 2.6-fold greater for animals receiving TC-002 than those on RLD-LAT on days 1 and 27. Sufficient data points were available for the calculation of AUCinf and terminal t1/2 in 4 groups, 1 on day 1 and 3 on day 27. AUCinf and terminal t1/2 were 2.4- to 3.3-fold and 1.4- to 1.9-fold higher, respectively, in the TC-002 groups compared to the RLD-LAT male group (Table 5).
Summary of Latanoprost Acid Toxicokinetic Parameters—Day 27
AUCinf, area under the concentration-time curve from zero to infinity; NC, not calculatable; SD, standard deviation; T1/2, terminal elimination half-life.
Histopathology No test article-related microscopic or macroscopic findings were noted in the eyes or ocular adnexa of either group. All nonrelated microscopic findings occurred at a similar incidence between the 2 groups.
Discussion
The single-dose PK study showed that with both formulations, latanoprost free acid was rapidly taken up within 0.25 h in the ocular tissues and humors. Systemic exposure to the drug was minimal with concentrations below the limit of detection. Peak (Cmax) and total (AUClast) exposures to latanoprost free acid were highest in the cornea and lowest in the vitreous humor (and optic nerve AUClast for RLD-LAT only) and similar overall between the 2 formulations. The PK data are consistent between studies suggesting that contamination is low or more variability would be observed. 36
There is a perception in the medical community that BAK is necessary for the penetration of prostaglandin analogs and other drugs through the cornea. It is known that BAK disrupts tight junctions in the corneal epithelium. 38 However, PK studies with latanoprost have shown comparable aqueous humor concentrations of latanoprost using formulations with or without BAK. 39 A recent study compared the PK profiles at 0.5, 1, 2, 3, 4, 8, and 24 h postdose in aqueous humor and ICB of DB rabbits after dosing with either preservative-free/surfactant-free latanoprost or a formulation containing 0.02% BAK. The Tmax occurred at 1 h postdose in the aqueous humor and ICB in the current study and at 2 h for the aqueous humor between 0.5 and 1 h in the ICB in this study under similar, but not identical, conditions. Similar to the current study, latanoprost free acid concentrations were not statistically different between the 2 formulations in nearly all the samples. 40
Over the course of the 28-day Repeat Dose Tolerability Study, there were no abnormal ocular findings, including effects on IOP. No macroscopic findings were noted in the eyes or ocular adnexa of either the TC-002 or RLD-LAT groups. No test article-related macroscopic or microscopic findings were reported in the eyes or ocular adnexa.
The plasma concentrations of latanoprost acid detected in all samples were nominal (<6-fold the LLOQ of 0.05 ng/mL). There was no evidence for systemic accumulation of latanoprost acid for either formulation as evidenced by all day 27 plasma samples below the level of quantitation 4 h postadministration. This is supported by a terminal t1/2 of <0.5 h, when it could be calculated. While the latanoprost systemic exposure following topical ocular administration of 0.005% TC-LAT was greater compared with RLD-Xalatan, the systemic exposure and difference between the 2 formulations were negligible. A study in New Zealand white rabbits also reported comparable PK for latanoprost formulations with or without BAK. 39
While this article focuses on the preclinical PK and ocular safety of this new formulation, from a pharmaceutics perspective, in a simulated 28-day use study, the concentration of latanoprost and BAK did not change. Furthermore, while the drop size of TC-002 is nominally larger than marketed Xalatan, this did not result in any difference of note in this study. Furthermore, drop size changes within 20–50 μL have little effect on clinical measures in humans.41,42
BAK is an effective preservative for multiuse bottles; however, it is generally considered to be the most toxic preservative to the ocular surface. 10 The antimicrobial efficacy of this agent is generally thought to be inversely proportional to its ocular surface compatibility. 43 BAK has deleterious effects on many ocular cells and tissues, including the conjunctiva, corneal epithelium, trabecular meshwork, and lens epithelium.10,44,45 These effects may be due, in part, to the induction of inflammatory mediators such as tumor necrosis factor (TNF) and interleukin (IL) 1. 6 Pro-apototic effects of BAK exposure have been observed in conjunctival epithelium, corneal epithelium, as well as trabecular meshwork cells.46–48 Conversely, lower concentrations of BAK in topical glaucoma formulations are associated with less damage to the cornea and conjunctiva. 11 Thus topical glaucoma formulations with low concentrations of BAK could be expected to be more beneficial to the ocular surface health. 11
A prospective 16- to 30-week clinical audit of 375 glaucoma patients with ocular surface disease was undertaken to test the hypothesis that BAK-free ocular hypotensives may provide clinical advantages over those containing the preservative. 49 Patients switched to BAK-free formulations experienced: a significant reduction in the use of lubricating drops (P ≤ 0.001); a significant improvement in McMonnies Dry Eye Questionnaire scores (P ≤ 0.0001); a decrease in the percentage of patients with low tear-film breakup time (P ≤ 0.0001); stable IOP levels (P = 0.105) compared to prestudy levels. These results suggest that a switch to BAK-free IOP-lowering medications may provide improvements in some symptoms of ocular surface disease for glaucoma patients on chronic topical medications.
One of the greatest challenges in glaucoma treatment is low patient adherence to their topical medication regimens. 50 Since glaucoma medications can be associated with ocular surface toxicity, most often due to the preservative used to decrease or prevent microbial contamination in the bottle of medication; 1 way to reduce the incidence of this adverse effect is by the use of preservative free medications or those with decreased preservative concentrations. 51 Addressing the health of the ocular surface may improve glaucoma treatment adherence and ultimately lead to better treatment outcomes. 51
Because of the numerous adverse effects of chronic exposure of BAK to the ocular surface, there is still a significant unmet need for the development of easily administering BAK-free topical drops, especially for diseases such as glaucoma. 7 The design of an innovative bottle to reduce BAK upon delivery is one way to address this need. 52 In fact, the DEWS II report recommends nonpreserved ocular lubricant for Stage 2 management of dry eye disease to minimize preservative-induced toxicity. 53 Providing latanoprost in a BAK-preserved bottle that is designed to reduce the preservative to below the limit of quantitation level as it is administered to the ocular surface should provide dual benefits—a well-preserved bottle of medication and an eye drop delivered to the eye that is essentially free of BAK.
Limitations
The current studies are limited by their small size and relatively short duration. The time frames of these studies may have been too short to show deleterious effects of BAK. However, these studies do provide important PK evidence for latanoprost delivered through the new TearClear bottle.
Conclusions
In conclusion, topical ocular administration of TearClear Latanoprost Ophthalmic Solution, 0.005% (TC-002), administered to the eyes of Dutch-belt rabbits once a day for 28 days was well-tolerated and comparable to the RLD Xalatan in terms of IOP lowering efficacy. No local ocular or systemic adverse effects were noted for either the TC-002 or RLD-LAT groups. Overall, the single dose and multiple-dose studies demonstrated that the toxicokinetic and PK profiles of TC-002 are similar to that of the RLD-LAT.
Footnotes
Acknowledgment
The authors acknowledge Julie Crider, PhD, for medical writing contributions.
Authors' Contributions
S.V.: Conceptualization, Methodology, Formal analysis, Writing—Original Draft, Writing—Review and Editing, Visualization, Supervision, Project administration, Funding acquisition. M.R.: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing—Original Draft, Writing—Review and Editing, Visualization, Supervision, Project administration.
Author Disclosure Statement
S.V. is an employee of TearClear. M.R. has no commercial interest in this report.
Funding Information
The study was funded by TearClear Corp.