
Abstract
Purpose:
To investigate the clinical efficacy of omidenepag isopropyl (OMDI) among glaucoma patients in terms of increased intraocular pressure (IOP) changes through a meta-analysis.
Methods:
Studies investigating the clinical efficacy of OMDI toward glaucoma patients were systemically searched. Inclusion criteria include recruiting studies that consisted of glaucoma or normal tension glaucoma patients who received OMDI treatment at least 4 weeks in duration. The primary outcome was to compare changes in IOP levels at baseline before OMDI treatment and after OMDI treatment.
Results:
Six studies were included with a total of 358 eyes. Our results showed OMDI monotherapy resulted in significant decreased IOP among patients with ocular hypertension, with weighted mean difference post-OMDI treatment being −4.684 (95% confidence interval: −6.010 to −3.358) and I2 of 91.092%. Separate subgroup analyses also showed initial IOP greater than 21 mmHg and those within the age group greater than 65 years old to be correlated with significant reduction in IOP post-OMDI. Randomized control trial (RCTs) design was also found to be superior compared with non-RCT in terms of investigating IOP changes after OMDI. The country of origin of the recruited studies and OMDI dosage frequencies were also found to have no effect on overall IOP changes after OMDI treatment.
Conclusions:
The current meta-analysis indicates OMDI to be a clinically effective treatment for glaucoma patients in terms of lowering IOP levels.
Introduction
Glaucoma is a group of optic neuropathy syndromes characterized by the progressive degeneration of retinal ganglion cells. It is a leading cause of blindness that affects more than 70 million people globally. 1 Because the pathophysiology underlining glaucoma is associated with increased intraocular pressure (IOP) level, the primary goal of treating glaucoma essentially involves the lowering of IOP.2,3
Various interventions for reducing IOP therapy currently exist. This includes medical treatment, laser therapy, and surgery. Medical treatment is widely accepted to be the first-line treatment for glaucoma. There are several categories for medical treatment of glaucoma depending on their mechanism of action. One such category is the prostaglandin (PG) F2α analogs, which targets the F-prostanoid (FP) receptors. 4 F2α analog agents reduce IOP by enhancing the drainage of the aqueous humor through the uveoscleral outflow pathway as well as facilitating trabecular outflow. 5 There are four commonly used PG derivatives targeting the FP receptor, namely: Latanoprost, Bimatoprost, Travoprost, and Tafluprost. Due to their ease of use with once-a-day dosing as well as good efficacy in terms of lowering IOP, these drugs are widely used for glaucoma medical therapy. 6
Draw backs with regard to FP receptor agonists includes conjunctival hyperemia and prostaglandin-associated peri orbitopathy (PAP). PAP is a complication characterized by the appearance of color changing of the iris color, pigment deposition around the eyelids, increase in the length and number of eye lashes, dermatochalasis involution, deepening of the upper eyelid sulcus, loss of lower lid steatoblepharon, upper lid ptosis, lower lid retraction, and enophthalmos.6–8
Complications, such as PAP, are important as they can affect a patient's quality of life and impact treatment adherence.4–6 Therefore, there is an unmet need to provide glaucoma patients with an alternative monotherapy that is both as clinically effective as well as having a low side-effect profile. 9 With regard to this, recent studies have shown EP receptor for PGE2 to equally have an effect on the ciliary body and trabecular meshwork as well as significantly affect the IOP levels. 10 Omidenepag isopropyl (OMDI) is one such type of EP2 prostanoid receptor agonist. It is through the novel and specific targeting of EP2 prostanoid receptors that OMDI would theoretically have a lower side effect profile compared with the current standard FP receptor agonists. 11
OMDI is a relatively new drug that was first launched in Japan back in November 2018 and has only entered the wider global market in February 2021. It has also recently received approval from the United States FDA in September 2022 for the treatment of primary open-angle glaucoma or ocular hypertension. 9 However, in spite of all this, there is still a paucity of studies on OMDI. Much is still unclear about IOP outcomes after ODMI treatment.
Unknown factors include how patients' age, frequency of drug administration, the country of usage, initial IOP, and other myriad of variables would affect clinical outcomes after OMDI usage among glaucoma patients. It is perhaps due to the sparse information that there is still an absence of wider international approval for the clinical use of OMDI with clinical trials still ongoing in various countries. 9
We, therefore, seek to investigate and provide evidence toward the clinical efficacy of OMDI by undertaking meta-analysis of all published studies on glaucoma patients.
Methods
Our study protocol was performed in accordance with the statements from the Preferred Report Items for Systemic Reviews and Meta-analyses (PRISMA). 12 Our protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42022377641).
Literature search strategy
We searched Scopus, Google scholar, and PubMed using the following search terms of: “OMDI,” “glaucoma,” “ocular hypertension,” and “omidenepag isopropyl.” Additionally, a manual search of original studies was performed to identify articles that were potentially missed by the database searches. We also searched for relevant citations in identified literature. Only original, English research articles published in peer-reviewed journals from the earliest record to August 2022 were included in our current meta-analysis. Studies not published in English or not available in the full-length article were excluded (Fig. 1).
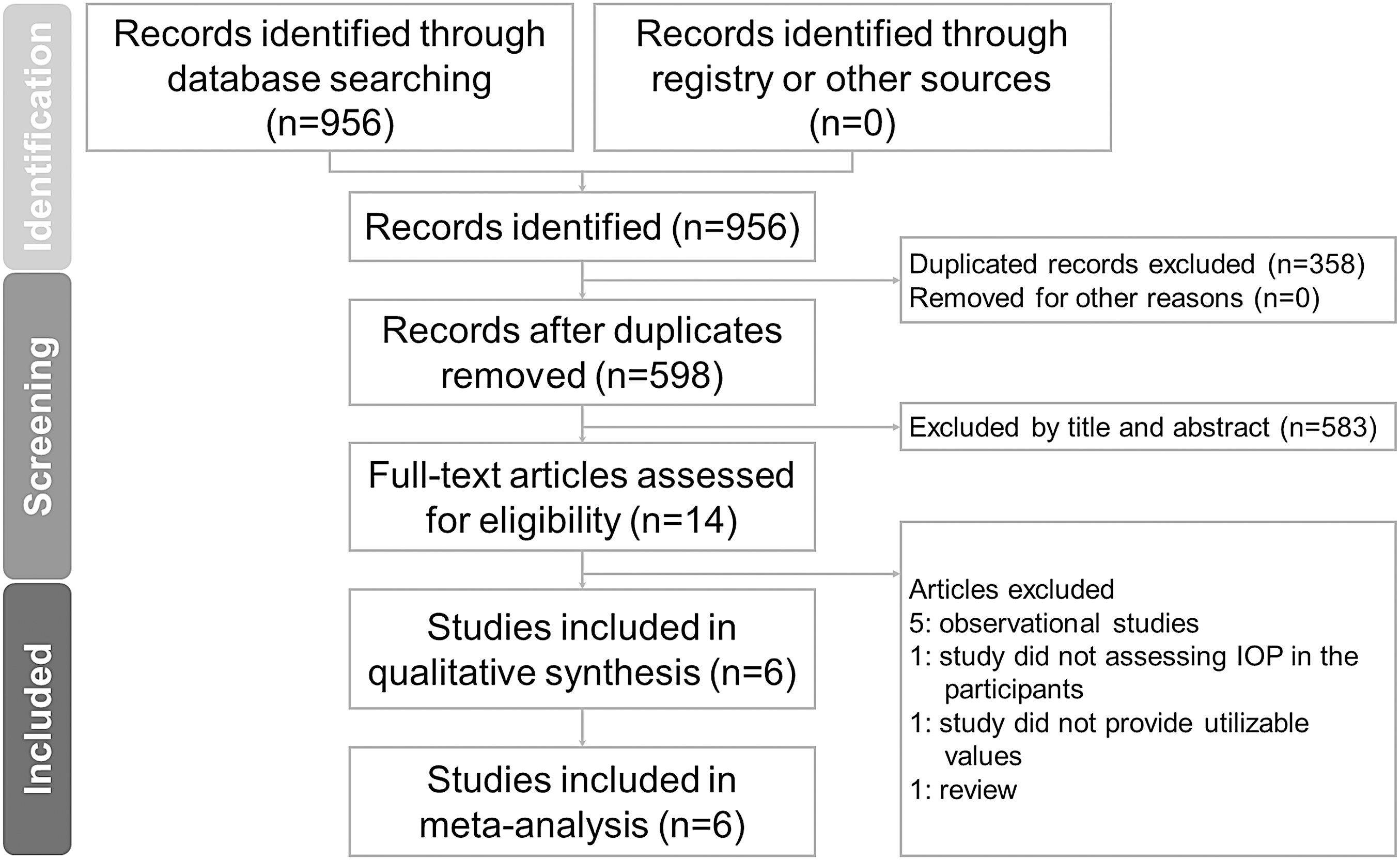
PRISMA Flow Diagram Literature search and study selection. This is a PRISMA diagram showing the different steps of our meta-analysis, starting from literature search to study screening and selection. For each step, the reasons for exclusions are indicated. PRISMA, Preferred Report Items for Systemic Reviews and Meta-analyses.
Eligibility criteria
The following inclusion criteria were applied to determine if the included studies were suitable for our meta-analysis: (1) studies with enrollment of adult patients with glaucoma or normal tension glaucoma who previously received FP receptor agonist agent at least once and their treatment regime was switched to OMDI; (2) studies that include OMDI treatment course of at least 4 weeks in duration; and (3) studies enrolled should include quantitative measurement of IOP pre- and post-OMDI intervention.
The following noncompliant studies were excluded: (1) Observational studies; (2) Animal studies (3) studies of which full text could not be obtained or no data available; (3) studies with patients who did not receive either OMDI or any FP receptor agonist agents; (4) studies with patients who did not receive OMDI for at least 4 weeks in duration; (5) studies of whom IOP was not an outcome measure of interest.
Our primary outcome was to compare IOP changes before and after ODMI intervention. Pooled weight mean difference (WMD) was used to estimate the efficacy of OMDI.
Study selection
Title and abstracts of all identified studies were independently reviewed by two researchers (H.T.K. and Y.C.Y.). Full-text evaluation of all potential studies was performed to assess for compatibility with the inclusion/exclusion criteria.
Data collection and risk of bias assessment
Once studies have been selected and included, data were extracted by two independent researchers (H.T.K. and Y.C.Y.). The extracted data were as follows: study design, first author, publication year and journal, location of study, patient demographics (gender, age), duration of follow-up of any usage of OMDI, concentration and dosage frequency of OMDI used, and mean IOP measurements during each follow-up. The risk of bias for each included studies were assessed by two researchers (H.T.K and Y.C.Y) according to Cochrane risk of bias and classified as “low,” “unclear,” or “high.” 13 We considered a study to be at high risk of bias if at least one domain was at high risk.
A first selection of studies was gathered by two reviewers based on their pertinence and relevance to our inclusion criteria (H.T.K and Y.C.Y). Discrepancies were resolved if one of the reviewers deems a study eligible. Data extraction and qualitive assessment of included studies were carried out by the two reviewers (H.T.K. and Y.C.Y.).
Data synthesis and analysis
This study followed the PRISMA criteria in reporting our results. 12 For articles containing data stratified into different treatment groups, these data were treated as separate treatment arms for analysis. All analysis were conducted by using the Comprehensive Meta-analysis software. We used the pooled weighted mean difference (WMD) to estimate the efficacy of OMDI. The data were calculated by taking the difference between the mean ocular pressure of OMDI and the mean baseline ocular pressure. A negative value for the effect size indicates a favorable result of OMDI compared with baseline. Pooled estimates and 95% confidence interval (CI) were calculated. Statistical significance was deemed to be achieved when P value was <0.05. Significant heterogeneity was defined as I2 > 50.0%. Random-effects model approach was used before proceeding to quantitative analysis. Heterogeneity was quantified using I2 and Cochran's Q tests.
We expected that heterogenicity might originate from either the different initial presenting IOP, by follow-up duration, by the type of study design recruited, by age of participants and by country of origin of the study. Thus, predefined subgroup analysis for patients were performed based on these factors. Funnel plot and Egger's tests were also used to assess the potential role of publication bias.
Results
Study search and characteristics of included patients
Figure 1 illustrates the study selection process. Overall, 956 studies were identified from the electronic search of all databases. Of the remaining 598 articles after duplicates were excluded, 14 received full-text assessment. Among these, five observational studies, one study without IOP data from the participants, one study with incomplete data sets, and one review article were excluded. Other studies that were excluded include: one study lacked assessment for IOP difference among their participants, one study lacked complete data sets and one was only a review article. A total of six articles (consisting of 358 eyes) screened based on aforementioned inclusion and exclusion criteria were included in this meta-analysis. Table 1 showed all the characteristics of the included studies.
Characteristics of Included Studies
Age is presented as means ± standard deviations.
OHT, ocular hypertension; OMDI, omidenepag isopropyl; POAG, primary open-angle glaucoma; RCT, randomized control trial.
Quality assessment and risk of bias
Risk of bias assessment is displayed in Table 2. The overall risk of bias of the included studies were mixed, with half of our included studies achieving low overall risk of bias, while the other half achieving high overall risk of bias. Three of our included studies were rated at low risk and three were rated at high risk for random sequence generation, respectively; half of the included studies were rated at low risk and high risk for allocation concealment, respectively; one of the studies was rated low risk and five of the included studies were rated high risk, respectively, for masking of outcome assessment. PRISMA checklist table was submitted as Supplementary Table S1.
Risk of Bias Summary for Each Study Based on the Cochrane Bias Assessment Tool
†Correction added on September 08, 2023 after first online publication of August 9, 2023: the word Blinding has been updated to
Intraocular pressure outcomes
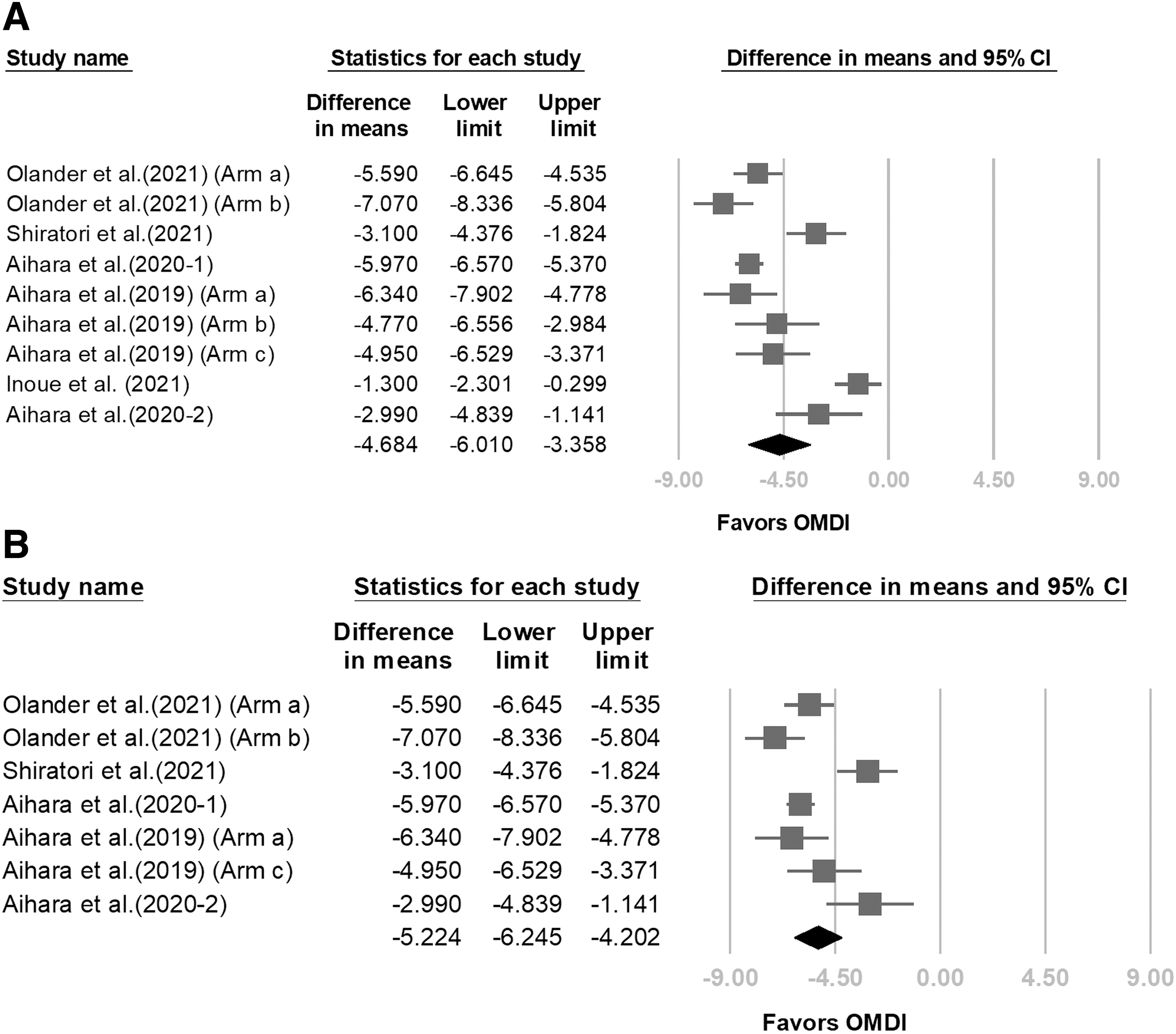
Pooled analysis from all six studies were performed to examine overall IOP changes before and after OMDI treatment. The WMD post-treatment from OMDI in terms of IOP changes was −4.684 (95% CI: −6.010 to −3.358). Regarding heterogeneity of the included study, the I2 was 91.092% (Table 3 and Fig. 2A).
Subgroup Analysis of Weight Mean Differences Based on Study Designs, Follow-Up Duration, and Initial Increased Intraocular Pressure
WMD (used for continuous variables with the same unit of measurement among meta-analysis).
IOP, increased intraocular pressure; WMD, weighted mean differences.
To determine whether dosing frequency of OMDI would be a source of confounding, a separate pooled analysis was done where IOP changes after OMDI treatment with once-daily dosage (QD) was examined exclusively and data containing twice daily dosing (BID) was excluded. The WMD obtained from this subgroup analysis on dosage frequency was −4.564 (95% CI: −6.089 to −3.040).
In the subgroup analysis that assessed for IOP changes after OMDI treatment when follow-up was restricted to 1 month (4–6 weeks) duration, the WMD obtained was −5.224 (95% CI: −6.245 to −4.202). Regarding WMD heterogeneity, the I2 was 80.317% (Fig. 2B).
In the subgroup analysis that assessed for IOP changes after OMDI treatment between the groups with high initial IOP (>21 mmHg) and low initial IOP (≤21 mmHg), the WMD of OMDI regarding post-treatment IOP in the high and low IOP groups were −5.551 (95% CI: −6.333 to −4.768) and −2.155 (95% CI: −3.916 to −0.393), respectively. Regarding heterogeneity, the I2 was 62.553% and 78.858%, respectively for the high and low initial IOP groups (Fig. 3A).
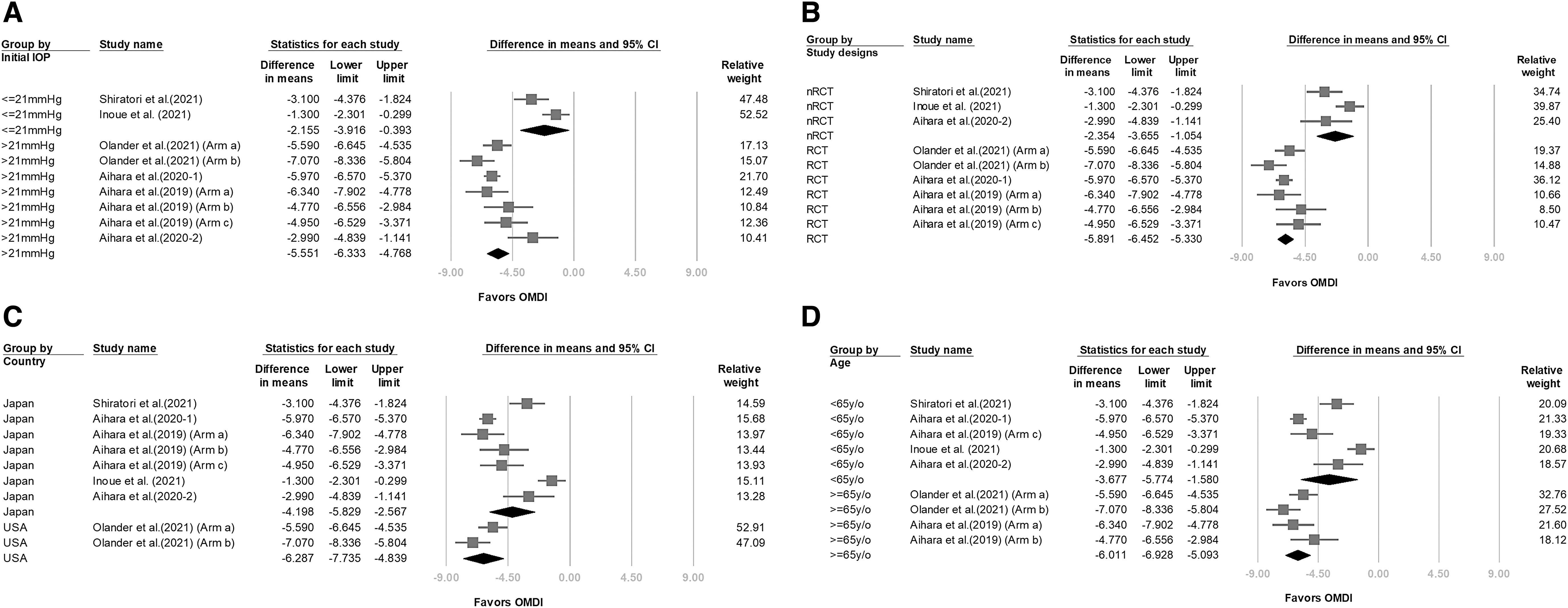
In the subgroup analyses that assessed IOP changes after OMDI treatment between the groups with recruited randomized control trials (RCTs) only and those without RCTs, our results showed that treatment effect of OMDI in terms of IOP changes seem to be more apparent among the subgroup with RCTs only. Furthermore, lower heterogeneity was found among the subgroup with RCTs only compared with the subgroup with no RCTs. The WMD of OMDI with regard to post-treatment IOP in the RCTs and non-RCTs (nRCTs) were −5.891 (95% CI: −6.452 to −5.330) and −2.354 (95% CI: −3.655 to −1.054), respectively. Regarding heterogeneity, the I2 was 27.469 and 64.841% for RCT subgroup and nRCT subgroup, respectively (Fig. 3B).
In the subgroup analysis based on the country of origin of the recruited studies, the WMD was −4.198 (95% CI: −5.829 to −2.567) and −6.287 (95% CI: −7.735 to −4.839) for studies originating from the Japan region and the United States region, respectively (Fig. 3C). I2 was 91.998% and 67.737%, respectively, for those from Japan and from the United States.
In the subgroup analysis based on age, the WMD was −6.011 (95% CI: −6.928 to −5.093) and −3.677 (95% CI: −5.774 to −1.580) for those above 65 years of age and those below 65 years of age (Fig. 3D). I2 was 43.661% and 94.267%, respectively, for those age groups above and below 65 years of age.
The included studies demonstrated no significant publication bias in terms of overall WMD, with P-value on the Egger's test being 0.266. The funnel plots for WMD of post-OMDI ocular pressure is shown in Fig. 4.
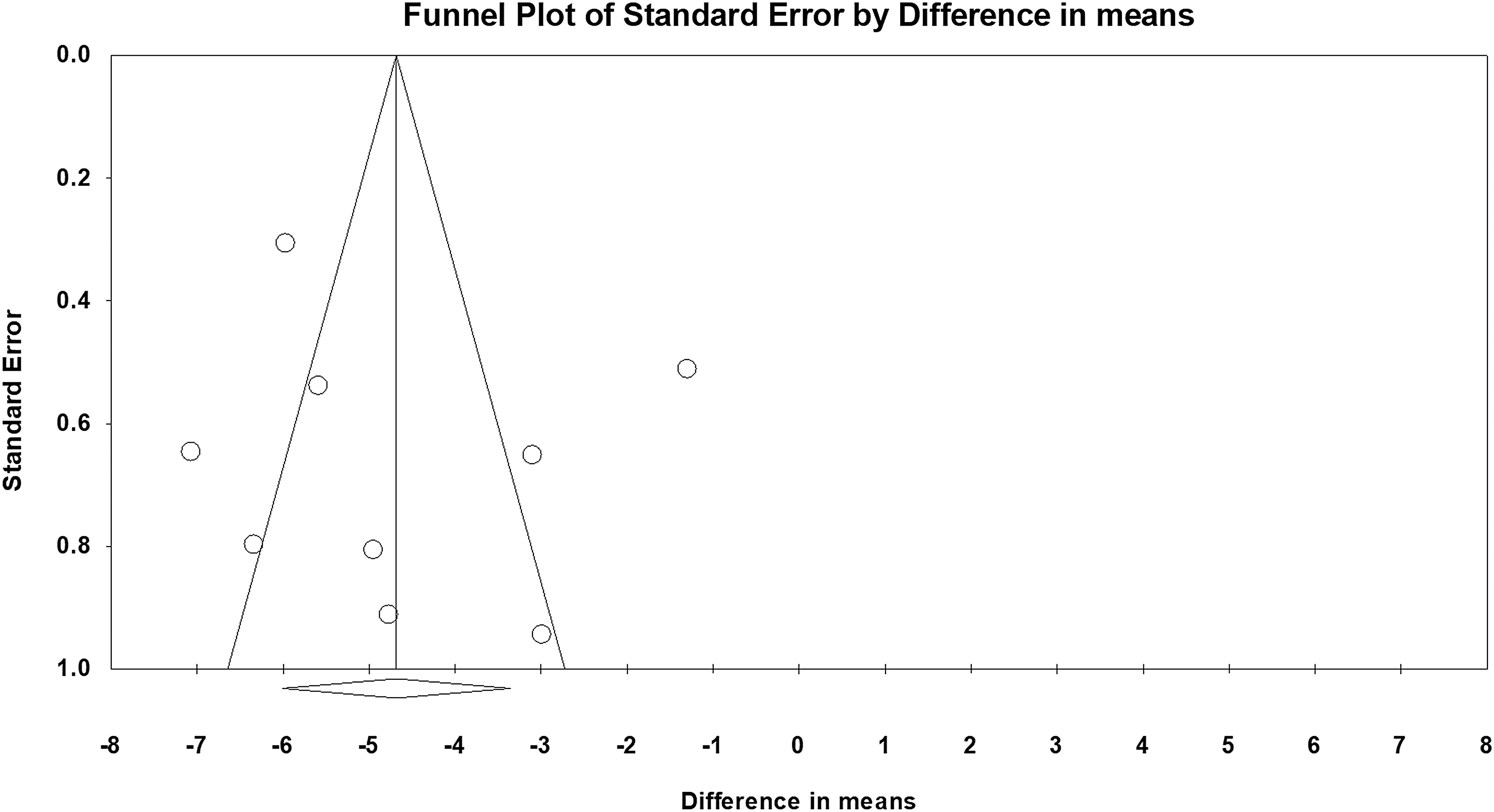
Funnel plots of 6 included studies based on WMD before and after OMDI treatment.
Discussion
To the best of our knowledge, this is the first study to investigate the clinical efficacy of OMDI in terms of lowering IOP among glaucoma patients.
Novel findings
The results of our meta-analysis demonstrated IOP changes in terms of WMD after OMDI treatment was −4.684 overall with no restriction on follow-up. Through pooled analysis, OMDI monotherapy was found to significantly decrease IOP among patients with ocular hypertension, especially among patients with initial IOP greater than 21 mmHg and those within the age groups greater than 65 years of age. RCT was also found to be superior compared with nRCT study design in terms of investigating therapeutic effects after OMDI as lower heterogeneity was achieved for the RCT group comparatively. We also found that the country of origin and once-daily dosage frequencies have no effect in terms of overall IOP changes after OMDI treatment.
Clinical implications
There is currently an unmet need for alternative options for glaucoma with equal clinical efficacy to the current standard treatment and simultaneously possessing a lower side-effect profile. The current first line and most commonly used medical management for glaucoma patients is widely considered to be PG analogs. 14 However, drawbacks with the standard PG analog include complications such as PAP. 21 OMDI has already been demonstrated in some nonclinical studies to have reduced risk for complications owing to its intrinsic drug structure. 22 Therefore, being able to demonstrate IOP-lowering efficacy in a meta-analysis would make contributions toward the wider adoption of OMDI as an alternative first-line agent for glaucoma patients.
Our results were able to demonstrate this by showing IOP standard mean difference of −4.684 mmHg after OMDI treatment among glaucoma patients. Our results were also almost entirely based on once-daily dosing of OMDI and this is important as multiple daily dosing may be negatively associated with patient adherence. 23 Overall, our results have clinical implications as it could influence clinical decision making with regard to the choice of medical treatment for glaucoma patients. Furthermore, our contribution of valuable data would further guide the methodology for future research into this novel glaucoma agent.
Comparisons to other studies
The present meta-analysis included 3 RCTs and 3 prospective experimental studies, with a total of 358 eyes. From our results, we have demonstrated that IOP standard mean difference decreased to −4.684 mmHg after treatment with ODMI. This is interesting as we can make comparisons between our results and with other studies on similar patient groups such as Li et al. 24 Li et al. was a meta-analysis conducted in 2016 of which they recruited 114 RCTs with data from 20,275 glaucoma participants. Li et al. recruited patients that received topical medical interventions from one of the four drug classes: beta blockers, carbonic anhydrase inhibitors, alpha-2 adrenergic agonist, and PG analogs. Their result showed reductions in IOP when patients received standard topical glaucoma drugs compared with the placebo group. They also showed that drugs in the PG class were more clinically effective compared with drugs from other classes.
In terms of the PG subgroup, Li et al. demonstrated mean reductions in IOP at 3 months, with examples of IOP mean reductions (95% credible intervals) from their study showing 5.61 (4.94; 6.29) for bimatoprost and 4.85 (4.24; 5.46) for latanoprost. Our study in comparison only looked at OMDI, a topical agent, which also belongs to the PG agonist class. Our pooled analysis showed OMDI to significantly reduce IOP among glaucoma patients, with WMD being −4.684 in terms of overall IOP changes irrespective of the follow-up duration. Although direct comparisons between our study and Li et al. cannot be made as OMDI was not included in Li et al., their results complement our own as it validates the usage of the specific class of PG agonist (from which OMDI belongs to) on glaucoma patients.
In another study by Aihara et al., this was a Phase 3 study where they recruited 190 patients and randomized them in a 1:1 ratio to either ODMI or latanoprost and compared the effects of these two different PG agonists on IOP measurements over a 4 weeks' period. 7 Aihara et al. showed that OMDI was noninferior in terms of lowering IOP levels compared with latanoprost. This is encouraging results as latanoprost is a class of PG drugs that is considered among the first-line medical treatment toward glaucoma. Additionally, demonstrating noninferiority of this drug with OMDI further highlights the potential novel role of OMDI in glaucoma patients.
Strength and limitations
The current meta-analysis has strengths, which include being the first to present a pooled analysis on the clinical effect of OMDI on glaucoma in terms of IOP changes. There is currently a paucity of research in terms of clinical efficacy of OMDI for glaucoma and, therefore, our results serve as a milestone for future studies to follow-up on as well as provide guidance for doctors caring for glaucoma patients.
However, there were some limitations. One limitation is with regard to our small power and limited number of RCT studies included in our meta-analysis. It is possible that our observed outcome may be affected if larger number of RCTs were recruited. However, it should be highlighted that our lack of recruited studies stems from the fact that OMDI is a relatively new drug. Due to the limited studies that were included, our results can only provide valuable insights—and not definite conclusions, in terms of the clinical effects of this new novel ODMI agent on glaucoma patients.
Another limitation pertains to the considerable heterogeneity that exists in our study. We propose some explanations for this. As part of our several subgroup analyses, we aimed to analyze IOP changes at the 1-month interval. We chose the 1-month (4–6 weeks) interval because we theorize that this time point is just long enough for the OMDI therapeutic effect to stabilize, as well as to further prove that follow-up intervals is a source of heterogeneity.
It should be noted that if the recruited studies did not have available data at the predetermined 1-month point, then data after the 1-month point, which were closest to it was then chosen. In terms of our recruited studies, we had two studies of which there was an absence of follow-up intervals close to 1 month: one of which had follow-up interval post-OMDI treatment that was greater than 6 months 19 and one with only follow-up duration post-OMDI treatment at the 3-month point. 18 Therefore, these two studies were excluded from this subgroup analysis. We found reduced heterogeneity from this subgroup analysis on 1-month follow-up (I 2 of 80.317%) in comparison to the overall I2 value of 91.092% obtained from the pooled analysis with no restriction on follow-up duration.
Hence, the variability in follow-up intervals after OMDI usage among our recruited study could possibly be a source of observed heterogeneity. It should be further noted that we also found WMD decreased to −5.224 (CI: 4.202 to 6.245) among the subgroup of 1-month follow-up duration compared with the overall WMD of −4.684. It can be surmised from this subgroup analysis on 1-month follow-up duration that the arbitrarily set point of 1-month duration for our meta-analysis may have been too short in duration to assess for any meaningful treatment effect from OMDI. This is hinted from our included studies, where one study even reported some IOP increase even after 1 month of post-OMDI. 25
The second possible source of heterogeneity is from the presenting IOP from our recruited studies. This is hinted from our recruited studies, where some reported mean initial IOP being higher than 21, while the initial mean IOP was found to be lower or equal than 21 mmHg in others.16,19 The reason for this difference in initial IOP was possibly due to the fact that some studies recruited newly diagnosed glaucoma patients that have not received glaucoma medications yet, while others may have.
Furthermore, the application of a washout period after any preceding glaucoma medications was not uniformly applied across our different included studies and may have again contributed to this variability. This variation in initial IOP has implications, as it can affect the outcomes obtained from IOP-lowering medications like OMDI. It is also standard practice among clinical studies studying glaucoma patients to stratify patients based on baseline IOP level. Therefore, in our second subgroup analysis performed that examined the effect of high initial IOP (≥21 mm Hg) versus low initial IOP (<21 mm Hg) groups, we found that within the subgroup of high-presenting IOP (≥21 mmHg), the heterogeneity I2 value reduced to 62% compared with the overall I2 of 91.092%.
In terms of the WMD of the subgroup of high-presenting IOP, we found the value reduced to −5.551 (CI: 4.768 to 6.333) from overall WMD of −4.684. Comparatively, within the subgroup of low initial IOP, the heterogeneity I2 dropped to 78% and WMD decreased to 2.155 (CI: 0.393 to 3.916). From this subgroup analysis, we can surmise that the initial IOP has some effect on the subsequent change in IOP post-OMDI treatment. This indicates that initial IOP could be confounding factor and has implications for our study's results. Future studies should take note of these issues.
Our third subgroup analysis was with regard to RCT versus nRCT groups. The RCT subgroup's I2 value was 27% and nRCTs I2 was 64%. Reduction in heterogeneity is therefore clearly seen in the RCT group in comparison to the nRCTs. Furthermore, we can see that IOP-lowering effect is seemingly better within the RCT group compared with the nRCT groups (WMD of 5.891 and 2.354, respectively). Overall, this subgroup analysis on RCTs versus non-RCTs highlights the potential heterogeneity that underlines our study results may also possibly stem from the study designs (RCT or nRCT) recruited. It should be noted that among the three nRCT studies, two of the studies recruited patients with initial IOP that are less than 21 mmHg. This implies that the initial IOP levels is a possible confounding factor. Overall, the demonstration of these sources of heterogeneity from our recruited studies indicates inherent limitations from our study. However, it can also be a sign of strength, as being able to identify these sources of heterogeneities can better inform methodologies for future studies on this topic.
In spite of our use of subgroup analysis, one important problem with regard to this type of analysis is that subgroup analysis generally lacks the statistical power to find any significant differences between subgroups. This is especially the case in smaller scale meta-analysis such as ours and so any conclusions drawn must be followed up in future with either larger scale meta-analysis or prospective studies.
Our next subgroup analysis was based on the mean age of participants. From this subgroup analysis, we noticed that among the age group greater than 65 years of age from our recruited studies had greater mean baseline ocular pressure compared with those whose mean age were less than 65 years of age. As demonstrated earlier in our previous subgroup analysis and as of which cannot be explained yet, a higher initial IOP could result in greater response toward OMDI. However, there are several other general considerations that should be made with regard to glaucoma in geriatrics. Renal and hepatic functions that are responsible for drug metabolism are likely impaired among the elderly, which can result in delayed inactivation or elimination of said drugs. Implications of this is that it can lead to delayed elimination of previously used glaucoma drugs as well as exaggerated effects of regular doses of drugs taken such as OMDI. 26 Future studies should explore this phenomenon and shed further light.
Our final subgroup analysis was based on the country of origin of our recruited study in question. Studies from Japan and the United States showed some variation in WMD, with −4.198 for Japanese studies and −6.287 for those from the United States. Interestingly, ethnic group differences have been demonstrated in terms of treatment efficacy for glaucoma treatments. For example, in a study on Caucasian and African ethnicities with glaucoma, African ethnicities seemed to experience better visual outcomes when receiving argon laser trabeculoplasty (ALT) before trabeculotomy procedure. This is in contrast to Caucasians, who experience better IOP outcome when ALT was performed in between trabeculotomy procedures. Furthermore, in a clinical trial study by Aihara et al., they showed significant pharmacokinetic differences between their recruited Japanese and Caucasian subjects. Specifically, they found ethnic differences within the amount and concentration of the glaucoma drug given at various follow-up intervals within their study.
They hypothesized that it could be a consequence of the ethnical differences in mean body weight, as the mean average body weight for young Japanese males is estimated to be around 68.3 kg, while the mean average body weight for young Caucasian has been estimated in other studies to be around 87.9 kg. Therefore, these racial differences in mean average body weight have implications in terms of dose per weight for any given drugs, including OMDI. Biological differences based on ethnicity such as this could potentially affect OMDI treatment outcomes and therefore make our results not entirely generalizable to other population of different ethnical profiles. This again deserves some exploration in future studies.27,28
An additional limitation with regard to our study is in terms of gender. Due to the lack of gender information among our recruited studies, we were unable to provide any conclusions on how gender might have affected our results. Multiple observations have hinted women being at higher risk for glaucoma.
It is unknown why this is the case but levels of female hormones have been pointed out to be a factor. Estrogen has been known to enhance ocular blood flow from previous animal physiology studies and so any reduction in said female hormones could consequently lead to reduction in ocular blood flow. This can lead to increased vulnerability by the optic nerve and result in glaucomatous changes. 29 This is further supported in one large-scale study, where females who experienced early menopause were found to have heighted risk of glaucoma, compared with those who entered menopause after age 50. 30 In another study, they also found significant risk reduction in terms of glaucoma development among ocular hypertensive females who received a combination of estrogen and progestin. 31 Future studies should further delineate how gender would affect OMDI treatment outcomes.
Another limitation from our study was that our meta-analysis focused on the effect of OMDI solely, instead of comparing outcomes with other first-line glaucoma topical treatments. This limits any ability for direct comparisons. However, this is mostly due to the scarcity of research covering OMDI, with only two previous RCT published so far directly comparing OMDI with other glaucoma drugs.7,18
One final limitation is with regard to the outcome measure of interest. We chose IOP because it is one of the most commonly used measure to follow-up glaucoma patients among studies. However, this excludes some other potentially useful measures that are equally important, such as quality of life and other forms of visual outcomes.32,33 Furthermore, there were variability in terms of IOP measurement among our included studies, where some followed mean diurnal IOP while others took morning or evening IOP values. This could have implications again for our results and would be another source of heterogeneity.
Furthermore, there were some other unaccounted for confounding factors among the recruited studies that may have influenced the IOP obtained. Among our recruited studies, it was noted that some did not exclude other forms of corneal abnormality that may interfere with tonometry measurements, such as recent history of intraocular surgery or severe eye injury. Additionally, there was variability in terms of washout period from previous glaucoma topical agents, which may again interfere with our results. All these deserve some considerations in future studies.
Conclusion
Our meta-analysis analyzed the clinical effect of OMDI among glaucoma patients in terms of IOP changes. Our results have shown that OMDI demonstrated statistical significance in terms of lowering IOP levels among glaucoma patients. The clinical effect on IOP observed seem to be correlated with initial IOP levels as well as treatment duration. Based on our results, OMDI could potentially be a viable treatment option for the clinical cohort of glaucoma and OHT. However, future studies, including RCT, are still warranted.
Footnotes
Authors' Contributions
Conceptualization: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; methodology: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; software: H.T.K. and C.Y.Y.; validation: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., and C.J.L.; formal analysis: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; investigation: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; resources: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; data curation: H.T.K., C.Y.Y., J.H.C.H., and C.J.L.; writing—original draft preparation: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; writing—review and editing: H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.; visualization: H.T.K., C.Y.Y., J.H.C.H., and C.J.L.,; supervision: J.H.C.H., C.J.L., and Y.Y.T.; project administration: H.T.K., C.Y.Y., A.Y.H., ![]() ., C.J.L., and Y.Y.T. All authors (H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.) listed have made a substantial, direct, and intellectual contribution to the work, and gave final approval of the version to be published.
., C.J.L., and Y.Y.T. All authors (H.T.K., C.Y.Y., A.Y.H., J.H.C.H., C.J.L., and Y.Y.T.) listed have made a substantial, direct, and intellectual contribution to the work, and gave final approval of the version to be published.
Data Availability Statement
The data generated during and analyzed in this article are available from the corresponding author, without undue reservation.
Ethics Statement
This study is based on published documents, unrelated to personal data, so ethics approval is not needed. Our protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42022377641).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.