
Abstract
Purpose:
Previous literature has investigated opioid prescription trends in ophthalmology at large, however, little has been done looking at differences between subspecialties. We evaluate if significant trends exist among subspecialties in opioid prescribing patterns. This study aims to illuminate potential over-usage of opioids in ophthalmology that could compromise patient quality of life.
Methods:
Medicare data and “National Plan and Provider Enumeration System (NPPES) Downloadable File” were queried for cases of ophthalmologists with nonsuppressed opioid prescription data from 2014 to 2019. Ophthalmologists with no subspecialty code or missing regional, gender, degree, or graduation information were excluded. Chi-squared analysis, analysis of variance, t-tests, and multivariate logistic regression were utilized.
Results:
Five thousand one hundred forty-three physician records were included in analysis, 450 of which were by cornea subspecialists. Most cornea cases were male, graduated before 2005, and practiced in the South. All subspecialties had a significantly increased likelihood of making opioid claims and higher prescription rates compared with cornea (P < 0.050) besides glaucoma (P = 0.357). Only oculoplastics had significantly increased likelihood of greater total supply of opioids compared with cornea (odds ratio [OR] = 22.195, 95% confidence interval [CI] = 12.209–40.350, P < 0.001), while pediatrics (OR = 4.036, 95% CI = 1.377–11.831, P = 0.011) and neuro-ophthalmology (OR = 4.158, 95% CI = 1.237–13.975, P = 0.021) in addition to oculoplastics (OR = 64.380, 95% CI = 26.306–157.560, P < 0.001) were predicted to have significantly greater opioid beneficiaries. Males, the South/Midwest, and graduating before 2005, all were generally associated with increased likelihood of greater total opioid claims, supply, beneficiaries, and prescription rate (P < 0.050).
Conclusion:
Subspecialty, demographic, chronological, and regional trends exist for opioid prescribing patterns in ophthalmology.
Introduction
In recent years, opioid prescribing patterns in many medical specialties have been under increasing scrutiny. This may partially be attributable to President Trump declaring the opioid crisis a “public health emergency” on October 26, 2017. 1 Before the declaration, despite over 33,000 opioid overdose deaths in 2015, the number of opioid-related deaths had been steadily increasing for over a decade. 2 Opioid-related deaths have comprised a staggering three-quarters of all drug overdose deaths. 2 Furthermore, opioid abuse imposes heavy social and economic burdens on affected individuals and their families.3,4 On a larger scale, a report by the Council of Economic Advisers estimated the economic burden of the opioid crisis in 2015 to exceed 500 billion dollars. 5
A major contributor to the opioid epidemic is the abuse of prescription opioids. Since 1999, during the start of the first wave of opioid overdose deaths, deaths attributed to prescription opioids have increased fivefold. 6 In a viewpoint published in JAMA, the authors note that while about a third of adults in the United States deal with chronic pain and that its management is critical to achieving effective patient care, a 156% increase in opioid overdose deaths within just 5 years from 2010 to 2015, alongside an associated tripling in incidence of hepatitis C and increased overall financial burden, is alarming and calls for reevaluating opioid prescribing patterns. 7 One of the strategies of the Overdose Data to Action (OD2A) program implemented by the Centers for Disease Control (CDC) is to utilize prescription drug monitoring programs (PDMPs) to inform and improve opioid prescribing practices. 8
In ophthalmology specifically, various studies have been published investigating opioid prescribing patterns. Results of one study found nearly 90% of ophthalmologists prescribed 10 opioid prescriptions or fewer from 2013 to 2015, suggesting that the vast majority of ophthalmologists prescribe opioids responsibly. 9 Certain subspecialty-specific investigations, however, suggest that variation in opioid prescribing patterns exists between subspecialists. Among a cohort of oculoplastic specialists for example, the authors state that opioid prescribing was over four times higher than the rate of opioid prescribing among general ophthalmologists. 10
Another study reported the highest rates of filled opioid prescriptions postincisional surgery in strabismus, trauma, and retina surgery. 11 However, there is little large-scale literature to our knowledge specifically investigating differences in opioid prescribing patterns across all ophthalmology subspecialties. We perform this study using Medicare data to further investigate large-scale opioid prescribing patterns in ophthalmology, as well as evaluate potential influence of various provider characteristics, such as subspecialty, in prescribing behaviors. Finally, we explore if the declaration of the opioid crisis as a public health emergency influenced opioid prescribing patterns.
Methods
The “Medicare Part D Prescribers–by Provider” registry was queried for cases of ophthalmologists that had nonsuppressed opioid prescription data from the years 2014 to 2019. Through national provider identifiers, these data were merged with the Medicare “Doctors and Clinicians National Downloadable File” and “National Plan and Provider Enumeration System (NPPES) Downloadable File” to collect physician medical school graduation year and subspecialty taxonomy codes, respectively. Ophthalmologists with no subspecialty code or who were missing regional information, gender, or graduation year were excluded.
Pearson's chi-squared analysis was performed to discern significant deviation of observed frequencies from expected frequencies of cohort demographic characteristics for each subspecialty (gender, region, graduation year before and after 2005). Analysis was done for all years, 2014 and 2019 specifically, and then 2014 to 2016 versus 2018 to 2019. The last comparison was performed to evaluate if there was a significant difference before and after President Trump declared the opioid crisis to be a “public health emergency” in 2017. Analysis of variance and t-tests were also conducted for all three chronological conditions to evaluate significant differences between five measures of opioid prescribing patterns: mean total opioid claims, aggregate opioid cost, days of opioid supply, number of Medicare beneficiaries, and opioid prescription rate. Multivariable binary logistic regression adjusting for region, gender, graduation year (before or after 2005), subspecialty, and year (before or after 2017) for each of the five metrics of opioid prescribing patterns were finally performed excluding cases from 2017 once again. IRB approval was not required for this investigation as all data is publicly accessible online and no human subjects or identifying information were analyzed.
Results
The number of ophthalmologists making opioids claims that satisfied inclusion criteria increased from 603 in 2014 to 1,415 in 2019. The majority of ophthalmologists across all subspecialties and years were male (75.5%), from the South (37.9%), and graduated before 2005 (64.7%). However, there was only significant difference in graduation year (P < 0.001) but not region (P = 0.442) nor gender (P = 0.534). Similar trends were observed between 2014 and 2019 specifically as well as before and after 2017, where there was significant difference in the graduation year of ophthalmologists (P < 0.001) but not region or gender. See Table 1.
Demographics of Ophthalmologists Stratified by Subspecialty
SD, standard deviation.
Subspecialty-specific demographic characteristics may also be observed in Table 1. Frequencies of characteristics among cornea specialists paralleled those observed overall, where the majority of cornea specialists were male (70.9%), from the South (35.6%), and graduated before 2005 (56.2%). Likewise, across all years, 2014 and 2019 specifically, and before and after 2017, there was only significant difference in graduation year (P < 0.050) but not region or gender. Identical trends were observed in ophthalmologists specializing in oculoplastics and retina/uveitis. Similar trends were also observed for glaucoma specialists, except the majority of specialists were from the Northeast (31.5%) rather than the South (29.9%), although there was still no significant difference (P > 0.050). Neuro-ophthalmologists were similar to glaucoma specialists in that their most common region was the Northeast (33.6%), but there was no significant difference in the number of neuro-ophthalmologists who graduated before 2005 versus after 2005 across all years, 2014 and 2019, or pre/post-2017 (P > 0.050).
Pediatric/strabismus ophthalmologists, on the other hand, still were most commonly from the South (45%), but like neuro-ophthalmologists, there was no significant difference across all three chronological conditions in graduation year, alongside gender and region.
Across all years, the mean total opioid claim, including all subspecialties was 23.00 ± 50.68, the mean aggregate opioid cost was 126.21 ± 322.10, the mean days of opioid supply was 75.49 ± 176.75, the mean number of Medicare beneficiaries was 21.08 ± 46.52, and the mean opioid prescription rate was 4.29 ± 8.40. There were significant differences between the means of all five opioid metrics across all years, the years 2014 and 2019, and before and after 2017 (P < 0.001). Results varied by subspecialty, however. For cornea specialists, while there was significant difference in total opioid claims across all three chronological conditions, the aggregate cost of opioids was significantly different across all years (P = 0.047) and before and after 2017 (P = 0.031), but not between 2014 and 2019 (P = 0.147). The same was observed for days of opioid supply, but the number of Medicare beneficiaries was only significantly different when comparing before and after 2017 (P = 0.008). There was no significance across any chronological condition in the opioid prescription rate for cornea specialists.
For neuro-ophthalmologists, there was no significant difference in any of the five metrics of opioid prescribing patterns in any of the three chronological conditions, while for glaucoma specialists there was only significant difference in opioid prescription rate across all years (P = 0.048). Among oculoplastic specialists, there was no significant difference in total opioid claims or the number of Medicare beneficiaries under any chronological condition; however, there were significant differences observed across all years in mean aggregate opioid cost (P < 0.001), days of opioid supply (P = 0.002), and opioid prescription rate (P = 0.021). For pediatric/strabismus specialists, there was significant difference between 2014 and 2019 and pre- and post-2017 in aggregate opioid cost, days of opioid supply, and opioid prescription rate (P < 0.050). There were no significant results across all years for pediatric/strabismus ophthalmologists. Finally, for retina/uveitis specialists, there was significant difference in all five opioid metrics under all three chronological conditions (P < 0.001). See Table 2.
Opioid Prescription Practices Stratified by Subspecialty
Multivariable binary logistic regression evaluating significant predictors of high opioid prescription practices (≥1 standard deviation above the mean) can be observed in Table 3. Pre-2017, male gender, Northeast region, graduating before 2005, and the cornea subspecialty were the reference variables. Post-2017 (odds ratio [OR]: 0.67, 95% confidence interval [CI]: 0.52–0.85, P = 0.001), female gender (OR: 0.52, 95% CI: 0.38–0.70, P < 0.001), and graduating in 2005 or after (OR: 0.51, 95% CI: 0.39–0.68, P < 0.001) were associated with a significantly decreased likelihood of ≥1 standard deviation above the mean number of total opioid claims. Conversely, the South (OR: 2.46, 95% CI: 1.75–3.48, P < 0.001), neuro-ophthalmology (OR: 4.04, 95% CI: 1.05–15.44, P = 0.042), pediatric/strabismus (OR: 4.16, 95% CI: 1.26–13.79, P = 0.020), and oculoplastics especially (OR: 62.26, 95% CI: 1.26–13.79, P < 0.001) were associated with a significantly increased likelihood of high opioid total claims.
Binary Logistic Regression for Factors Associated with Opioid Prescription Practices ≥1 Standard Deviation Above the Mean
CI, confidence interval; OR, odds ratio.
Post-2017, female gender, and graduating in 2005 or after were additionally generally associated with significantly decreased likelihood of high aggregate opioid cost, days of opioid supply, number of Medicare beneficiaries, and opioid prescription rate. Ophthalmologists with decreased experience, graduating in 2005 or after, show significantly decreased opioid prescribing patterns across several metrics compared with their more experienced counterparts. The only exception was that graduating in 2005 or after was not a significant predictor of high opioid prescription rate (OR: 1.27, 95% CI: 1.00–1.61, P = 0.054). The South and oculoplastics, on the other hand, were consistently associated with increased risk of high aggregate opioid cost, days of opioid supply, number of Medicare beneficiaries, and high opioid prescription rate (P < 0.050). Additionally, the Midwest was associated with increased likelihood of high aggregate opioid cost (OR: 1.79, 95% CI: 1.16–2.76, P = 0.009) and high opioid prescription rate (OR: 2.77, 95% CI: 1.93–3.99, P < 0.001), while the West was only associated with increased probability of high opioid prescription rate (OR: 1.98, 95% CI: 1.34–2.92, P < 0.001).
In terms of subspecialties, aside from oculoplastics, neuro-ophthalmology (OR: 4.04, 95% CI: 1.06–15.44, P = 0.042) and pediatric/strabismus (OR: 4.180, 95% CI: 1.26–13.85, P = 0.019) were associated with greater risk of a high number of Medicare beneficiaries.
Discussion
Trends over time
From 1999 to 2019, opioid overdose has caused 500,000 deaths, and many of these deaths are attributed to overprescription of opioids. 6 In response to efforts to combat the opioid burden, overall U.S. opioid prescription rates have gone down since 2011. 12 Our study shows a similar downward trend in opioid prescription in ophthalmology from 2014 to 2019, where a downward trend is evident across all five metrics we used to model opioid prescription: total opioid claims, aggregate opioid cost, days of opioid supply, number of Medicare beneficiaries, and opioid prescription rate. This takes place in the setting of increased attention to opioid prescription due to the opioid crisis. Implementation and discussion of opioid prescription guidelines in various medical specialties have led to changes in opioid prescribing patterns, and recent studies implementing opioid guidelines in ophthalmology also show success in reducing opioid prescriptions.13,14 Considering documentation of numerous ocular effects, such as blurred vision, ptosis, and nystagmus that oral opioid users experience, in addition to the onset of retinal microembolisms and endophthalmitis common in intravenous abuse, an ophthalmology-specific analysis of opioid prescribing patterns is necessary.
Given the significant differences in opioid metrics in years before and after 2017, our study suggests that President Trump's declaration of a national public health emergency in 2017 influenced opioid prescription by ophthalmologists. The declaration was followed by a 2018 announcement of 1.8$ billion in grants to states to support efforts combating opioid abuse, 15 such as PDMPs. State-level and national opioid prescribing policies have been shown to have substantial beneficial effects, reducing opioid-related adverse effects 16 and increasing health care provider awareness of prescription opioid abuse. 17 It is also possible that the announcement itself, associated with publicity and coverage by news media, influenced public perceptions of opioid usage. 18 See Figure 1 for total opioid claims by subspecialty.
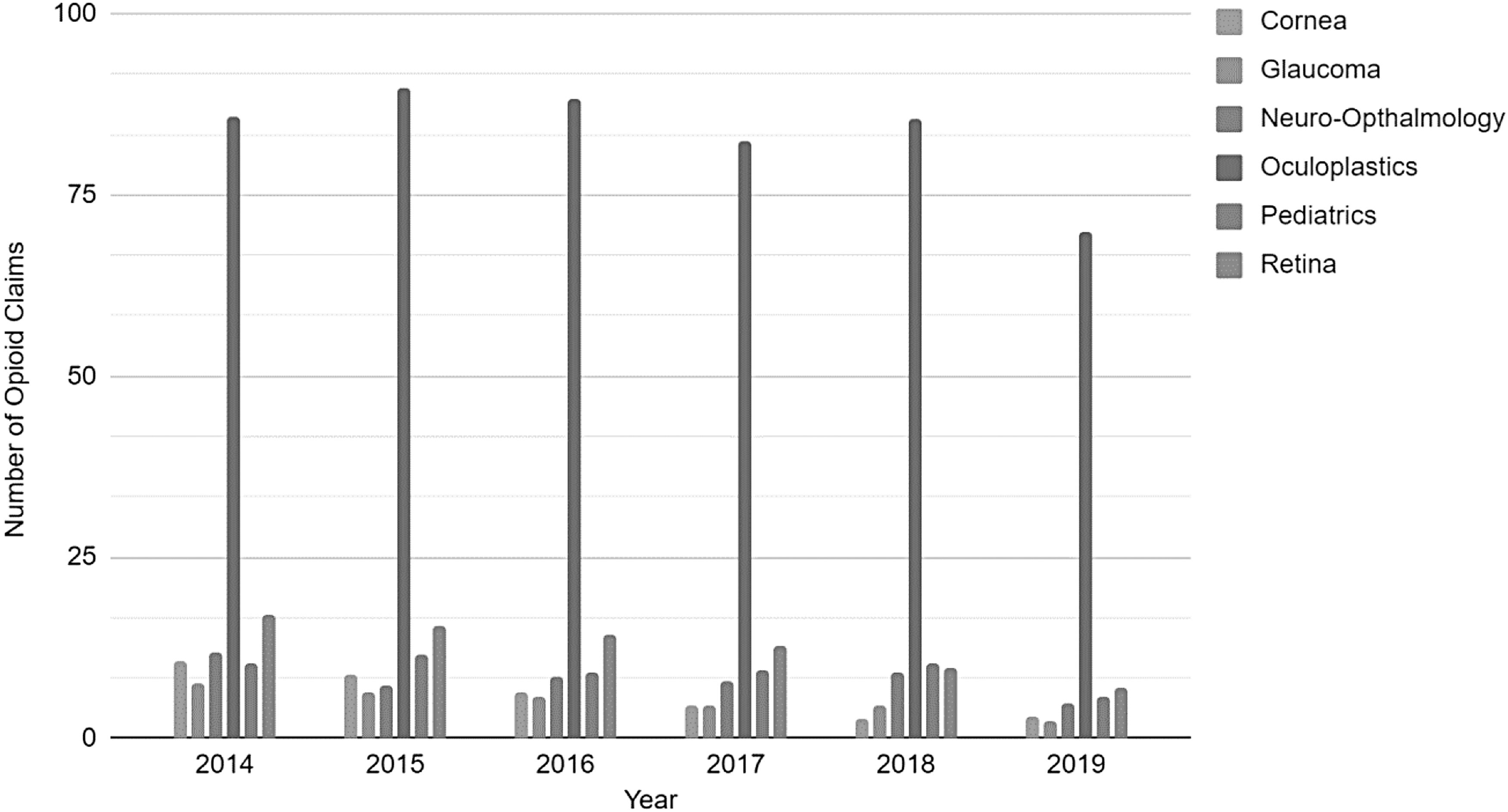
Total Opioid Claim Per Subspeciality from the years 2014–2019.
Interspecialty differences
Among all medical fields, surgical specialties are generally considered to be associated with increased opioid prescribing behavior.19–21 Within ophthalmology, subspecialties with a higher surgical volume, such as oculoplastics, tend to have higher prescription rates. 10 Our study expands on previous studies and is one of the first to our knowledge investigating differences in opioid prescription patterns between ophthalmic subspecialties. Our findings are consistent: oculoplastics was associated with high aggregate opioid cost, days of opioid supply, number of Medicare beneficiaries, and high opioid prescription rate. In addition, when looking at chronological trends, our data show that oculoplastics did not show significant changes in opioid prescription metrics. Furthermore, it is important to consider the high rates of opioid prescribing by other surgical specialties compared with ophthalmologists in oculoplastic surgeries. 22 As oculoplastic patients can also be seen by plastic surgeons and otorhinolaryngologists, regulation of their opioid prescribing behaviors is important as well.
Along with oculoplastics, glaucoma and neuro-ophthalmology also did not show a significant difference in opioid prescription metrics before and after 2017. The resistance of these subspecialties to change should be further investigated as current explanations are unclear. For example, microinvasive glaucoma surgery has gained traction; with less incisional surgery, one would expect less need for opioid pain management. 23 The lack of significant change in opioid prescription metrics may be due to a persistent perceived need for pain control in patients; Kolomeyer et al. has proposed other potential reasons, including desire to improve patient satisfaction. 11 In addition, it is important to consider the impact that mentorship has on practice patterns of newly trained ophthalmologists. By nature of training with certain people, young ophthalmologists pick up on clinical practices and routines of those mentoring them. Much of the success of residents is often measured by how well they imitate their attending physicians during their postgraduate training. 5
While younger generations are now taught the risk of opioids, the experience throughout training and what they observe from more senior ophthalmologists may not emphasize minimizing opioid prescribing as much.
Our study revealed retina, pediatrics, and cornea showing significant decreases in opioid prescription metrics over time. The study by Kolomeyer et al. showed that retina surgery was associated with the highest rates of filled opioid prescriptions per surgery from 2000 to 2016, before President Trump's declaration of the public health emergency. However, a 2020 corneal surgery study suggested patient opioid usage rates were far less than prescription fill rates, and as providers decreased the number of opioids, patients simultaneously lowered their utilization of these medications. It is possible that previous research, coupled with public attention prompting more informed patient decision making and implementation of guidelines in response to the declaration, has significantly influenced retinal and corneal subspecialist prescription behavior since 2016. More likely, however, much of the surgical procedures performed by corneal and retinal surgeons may produce less pain in patients compared with other subspecialties, including oculoplastics. Change in surgical practices and perioperative pain management may also decrease need for opioids postoperatively.
Similar to glaucoma surgeries, retina surgery has become increasingly minimally invasive with the development of small gauge vitrectomy and the decreasing use of scleral buckling. Through the increased use of intravitreal anti-vascular endothelial growth factor medications, more and more diabetes-related surgical problems can be better treated and managed nonsurgically. 24
The growing concerns of children being especially vulnerable to adverse opioid effects and the dangers of early exposure are in line with the observed susceptibility of pediatric ophthalmology to decreased opioid prescriptions. Younger patients are more likely to underestimate the risks of opioid misuse and have higher risk of accidental prescription opioid overdose, as well as carry developmental effects and increased risk of opioid misuse to adulthood.25,26 Even children exposed to opioid misuse in the household experience adverse consequences, including risk of drug use and accidental opioid poisoning. 27 Newer research in pediatrics has also advocated for perioperative and postoperative anesthetic techniques, such as eye drops, to minimize need for postoperative opioid use.28,29 Extensive research and guidelines should be performed and implemented addressing postoperative pain management in the pediatric population, as inappropriate pain management can also lead to opioid misuse. 26
A study in cornea surgery showed that physician awareness of opioid use decreased prescription dosages; furthermore, patients who were prescribed less opioids still achieved adequate pain control. 30 Another study in cataract surgery showed that perioperative opioid use with topical anesthesia increased adverse side effects such as nausea, vomiting, and hyperalgesia. 31 Furthermore, while opioid use did decrease reported pain, it did not affect satisfaction with pain management. Systemic opioid use for pain management is not as essential after cornea surgery compared with other subspecialty surgeries at baseline. As cornea involves the ocular surface, frequently opioids are used topically rather than systemically to control pain, reduce inflammation, and reduce dry eye. 32 In addition, other medications are first-line for neuropathic corneal pain, as there is no consensus about opioid efficacy.33,34 These studies may suggest that cornea subspecialists may have been prone to overprescribing opioids for refractive surgery and dry eye disease in the past, thus being more susceptible to newly implemented guidelines and education. 35
Although pain management in postoperative patients is of importance, postoperative patients are often overprescribed opioids. 36 Moreover, advances in ophthalmic surgery techniques have aimed to increase patient satisfaction by reducing postoperative recovery times and invasive techniques. 11 Thus, ophthalmologists should be cognizant of the risk of overprescribing and carefully consider the best pain management plan for their patients.30,31
Other characteristics
Our data also showed the influence of region and gender on opioid prescription behaviors. Practicing in the South was significantly and consistently associated with higher opioid prescription metrics. This aligns with other studies showing higher opioid prescription rates in the South, by ophthalmologists as well as providers in other surgical and nonsurgical specialties.9,20,37 States in the South have reported a disproportionate number of opioid prescriptions and opioid-related deaths. 38 Given this high burden, states in the South have created action plans to address opioid use. 38 These action plans include expansion of medication-assisted treatment programs for patients, as well as PDMPs and guidelines to promote nonpharmacological therapy and nonopioid pharmacological therapy for health care systems. These regional differences can be explained by several factors. A study reporting regional differences in opioid-related news reporting showed that higher news volume was associated with areas that were more educated, urbanized, and located in the Northeast. 39
The same study found that opioid-related deaths are more common in areas that have a greater population of Caucasian people and are more rural, which according to the Census Bureau are concentrated in the South and Midwest. 40 Other hypotheses include differing policies and marketing by pharmaceutical manufacturers across different regions. 41
Our study showed female ophthalmologists were less likely to prescribe opioids; however, other studies that characterize gender differences have mixed results. Some studies report that female physicians are more likely to be conservative in prescribing medications and adhere more closely to guidelines, reflecting lower risk-taking tendencies.42,43 Other studies report no gender difference.44,45 Another study has reported female gender is associated with greater intent to prescribe an opioid. 46 The same study, along with others, 47 also reports female gender is associated with greater likelihood to address psychosocial aspects of pain and perhaps be more cognizant of the patient perspective of pain. 46
Interestingly, another study reports that female physicians with higher competence and communication scores were less likely to prescribe opioids, while more competent male physicians tended to prescribe higher doses. 48 Additionally, while the percentage of women in surgical specialties is increasing, one must wonder if women are choosing to practice nonsurgically for similar reasons that deterred females from choosing surgical specialties in the past. Further study of gender differences is warranted. 49
The significant difference in opioid prescription between providers with a graduation year before and after 2005 can also be attributed to increased efforts to raise awareness over time. Our results suggest that providers graduating in 2005 or after were associated with a significantly decreased likelihood of high total opioid claims, aggregate opioid cost, days of opioid supply, and number of Medicare beneficiaries. Previous studies have investigated the role of physician education on opioid prescribing behaviors.50,51 Notably, the Association of American Medical Colleges released a statement with 74 medical schools expressing their commitment to opioid education. 52 Efforts, such as the CDC Guidelines for Prescribing Opioids for Chronic Pain, were created to improve physician awareness and promote thoughtfulness on the risks and benefits of opioid use for chronic pain. 53 State committees have encouraged sponsorship of research and training programs, and academic institutions have encouraged education and discussion through programs such as conferences. 38
As a result of more recent medical school graduates receiving more education on the opioid epidemic compared with more experienced physicians, 52 less opioids appeared to be prescribed by physicians in recent years. In particular, a 2014 study of primary care providers' perceptions of clinical opioid usage shows that younger physicians report significantly more concern about potential opioid dependance than older counterparts. Whether formally 54 or through clinical experience, 55 educational efforts during physician training can make an impact on opioid prescribing.
Although prescription rates have decreased, opioid-related deaths have not. 56 One of the opioid metrics we considered was days of opioid supply prescribed. This metric is important to include, as previous studies have noted the importance of not only prescription rates but also quantity and patient use of the prescription. 14 Thiels et al. quantified ∼92% of patients who do not use their opioid prescriptions keep the medication, which can be diverted to others or even utilized by the same patient at a later time. 57 The same study found that 71% of opioid abusers receive their opioids through diversion rather than their own medical prescriptions. Multiple studies have observed high rates of improper disposal of unused opioids by patients, creating opportunities for diversion. 30 This warrants a continued need for consideration of opioid prescription guidelines to address not only prescription rates but also prescription usage.
Our study possesses certain limitations. Physicians subspecialized, but not registered under a specific subspecialty taxonomy code, were not included in our analysis. Additionally, the 2017 data are excluded from the regressions, as we were unable to split data within the year of 2017 before and after the exact date of the public declaration on October 26th. However, given the ongoing discussion surrounding opioids in 2017 all year long, and the potential for a few months following the public declaration for ophthalmologists to adapt their clinical practice patterns, excluding 2017 as a “transitional year” and looking at the opioid prescribing patterns in years prior and years subsequent, was a reasonable decision.
Conclusion
Although ophthalmologists have a low prescription rate compared with other specialties, with 4% of all prescriptions being opioid prescriptions, opioid awareness is still critical. 9 Our study is consistent with other studies that show gender and regional influences on providers' opioid prescription practices. In addition, our data further elucidates discrepancies in opioid prescription between different subspecialties in ophthalmology, specifically surgical subspecialties such as oculoplastics. We propose that the presidential declaration of the opioid epidemic as a “public health emergency” succeeded in drawing attention to opioid prescriptions and enacting changes in prescription patterns. Although our study shows that in ophthalmology, opioid prescription patterns have improved from 2014 to 2019, the opioid crisis is still ongoing. Opioid prescription guidelines and thoughtful opioid stewardship by health care professionals can lessen the burden of the opioid crisis. 58 Efforts should continue to reduce health care sector contributions to the opioid epidemic.
Footnotes
Authors' Contributions
H.S.C. contributed to project conceptualization (lead), methodology (lead), data collection, data analysis (lead), article writing (equal), and article editing (lead). A.M.P. contributed to methodology, data analysis, and article editing. A.Z. contributed to methodology, article writing (equal), and article editing. S.G. contributed to methodology, data collection (lead), and article editing. A.S. contributed to methodology, data collection, and article editing. H.S.S., C.W.S., and M.H.D. all equally contributed to project conceptualization, project supervision, and article editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.