
Abstract
Purpose:
To assess antibiotic prescribing patterns among ophthalmologists and optometrists from 2018 to 2021.
Methods:
This is an observational, retrospective cohort study of the Medicare Part D prescriber public use files from 2018 to 2020. Prescription trends were analyzed with analysis of variance and negative binomial regression tests based on specialty, region, and types of antibiotics.
Results:
From 2018 to 2021, the number of ophthalmologists in the Medicare Part D database decreased from 18,452 to 18,285, and the number of optometrists increased from 23,071 to 24,734. Throughout the study period, the total number and proportion of antibiotic prescriptions by ophthalmologists and optometrists stayed almost constant with a dip in 2020, likely reflecting the effects of the COVID-19 pandemic. Both ophthalmologists and optometrists demonstrated geographic regional differences in prescribing patterns. The South consistently had the highest average number of claims per provider. Of the antibiotics prescribed by ophthalmologists in 2021, 48.6% are from the fluoroquinolone class, 20.5% are from the aminoglycoside class, and 18.2% are from the macrolide class. Optometrists were found to be more likely to prescribe antibiotics in a formulation combined with a corticosteroid throughout the study period.
Conclusions:
Our results have shown that prescribing patterns among ophthalmologists and optometrists have demonstrated significant changes in prescriptions of microbial resistance-promoting antibiotics. These patterns persist despite nation-wide attempts to control antimicrobial resistance.
Introduction
The World Health Organization's Global Antimicrobial Resistance and Use Surveillance System reported 1.27 million deaths attributed to bacterial antimicrobial resistance in the year 2019 alone. 1 Antimicrobial resistance is a global issue that spans all fields of medicine including Ophthalmology. Ocular infections can have a variety of presentations and causative microorganisms that are often treated empirically with broad-spectrum antibiotics that come in the form of ophthalmic drops, ointments, and intraocular formulations. Because of widespread injudicious use of conventional antibiotics, improper treatment therapy, polypharmacy, lack of standardized treatment guidelines, and the inclination of ocular microbiomes to form biofilms that prevents their clearance, widespread antimicrobial resistance has emerged. This has led to difficulty treating patients and increased morbidity. Surveillance programs such as Ocular Tracking Resistance in the United States Today (TRUST) and Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) have been established to monitor ocular pathogens in the United States.
These groups report significant resistance in many common bacteria. 2 Studies have found that the use of prophylactic antibiotics with intravitreal injections has resulted in an increase in resistant strains of bacteria that colonize the ocular surface.3,4 In addition, it has been shown that shorter periods of postoperative topical antibiotics are less frequently associated with persistent antimicrobial-resistant bacteria in the ocular flora. 5 This is particularly important in the elderly population, where intervention for conditions such as cataracts and glaucoma may be followed by ophthalmic antibiotic use. 6 Elderly patients have also been shown to have increased susceptibility to ocular bacterial infection, which can increase the population's prescriptions. 7 Systemic antimicrobial resistance is a well-researched topic, and ocular-specific antimicrobial resistance research is growing. However, there have been no studies looking at actual prescription trends of ophthalmologists and optometrists in the United States. This study aims to examine trends in antibiotic prescription patterns of U.S. ophthalmologist and optometrists using the Medicare Part D data from 2018 to 2021.
Methods
This study is an observational retrospective review of antibiotics prescribed by ophthalmologists and optometrists using public use files of Medicare Part D prescribers from 2018 to 2021. No IRB review was necessary since we used public use files. After analysis of all antibiotics prescribed, filters were applied for the most common antibiotics prescribed to include both variation in formulation and combination formulations: neomycin/polymyxin B/dexamethasone, erythromycin, tobramycin/dexamethasone, ofloxacin, moxifloxacin, doxycycline, ciprofloxacin, cephalexin, tobramycin, polymyxin B sulfamethoxazole/trimethoprim, azithromycin, besifloxacin, amoxicillin/potassium clavulanate, gatifloxacin, minocycline, bacitracin/polymyxin B sulfate, bacitracin, tobramycin/loteprednol, gentamicin, amoxicillin, neomycin/bacitracin/polymyxin/hydrocortisone, neomycin/bacitracin/polymyxin B, levofloxacin, and these data were exported to Microsoft® Excel®, SAS®, and RStudio® for analysis.
Regions were assigned based on those defined by the U.S. Census Bureau. 8 Analysis of variance tests were used to analyze differences in antibiotic claims across regions, and negative binomial regression tests were used to evaluate trends in total claims from 2018 to 2021 with P values <0.5 deemed statistically significant.
Results
From 2018 to 2021, the total number of ophthalmologists in the Medicare Part D database decreased from 18,452 to 18,285, a 1% decrease (Table 1). In addition, the number of optometrists increased from 23,071 to 24,734, a 7.0% increase (Table 1). The total number of antibiotic prescriptions by ophthalmologists decreased from 3.39 million to 3.26 million during the study period; however, the proportion of all antibiotic claims stayed about the same, from 13.0% in 2018 to 13.17% in 2021. This number was lowest in the year 2020 at 2.86 million, a 14.9% decrease compared with the previous year. Optometrists demonstrated a rise in the number of antibiotic prescriptions and a similar trend in proportion with 430,000 claims (8.0%) in 2018 and 484,000 claims (8.17%) in 2021.
Characteristics of Ophthalmologists and Optometrists and Antibiotic Prescriptions Dispensed
SD, standard deviation.
They also reached a low in 2020 with 397,000 claims, a 10.9% decrease compared with the previous year. In addition, there were slight changes in the average number of antibiotic prescriptions and median prescriber rates among both groups. In 2021, ophthalmologists had a mean prescriber rate of 133 claims per prescriber, and optometrists had a median prescriber rate of 26 per prescriber. The total cost of ophthalmologist-prescribed antibiotic claims in Medicare Part D decreased, and the number of optometry antibiotic claims during the study period increased (Table 1).
Both ophthalmologists and optometrists demonstrated different prescription patterns when regional geographic locations were analyzed (Table 2). “Other” was defined as Puerto Rico, Armed Forces, Guam, and Virgin Islands. However, the patterns were similar between groups. The South consistently had the highest average number of claims per provider. For ophthalmologists, this number decreased from 2018 to 2021, whereas optometrist numbers increased. Both groups had significant differences across the years. The average number of claims per provider for optometrists was lowest in the Midwest within the continental United States for both groups as well (Table 2). All regions demonstrated significant differences between the years of 2018 and 2021 except for the “other” group. There were also significant differences between all regions.
Regional Breakdown of Antibiotic Claims Per Provider, 2018–2021
Analysis of variance for differences in antibiotic claims across regions.
P < 0.05 deemed statistically significant.
This study also reviewed the most frequently prescribed antibiotics (Supplementary Table S1). Of the antibiotics prescribed by ophthalmologists in 2021, 48.6% were from the fluoroquinolone class, 20.5% were from the aminoglycoside class, and 18.2% were from macrolides (Fig. 1). Optometrists prescribed aminoglycosides 49.5% of the time, macrolides 23.5% of the time, and fluoroquinolones 15.13% of the time (Fig. 1). Optometrists were found to be more likely to prescribe antibiotics in a formulation combined with a corticosteroid throughout the study period (Fig. 1).
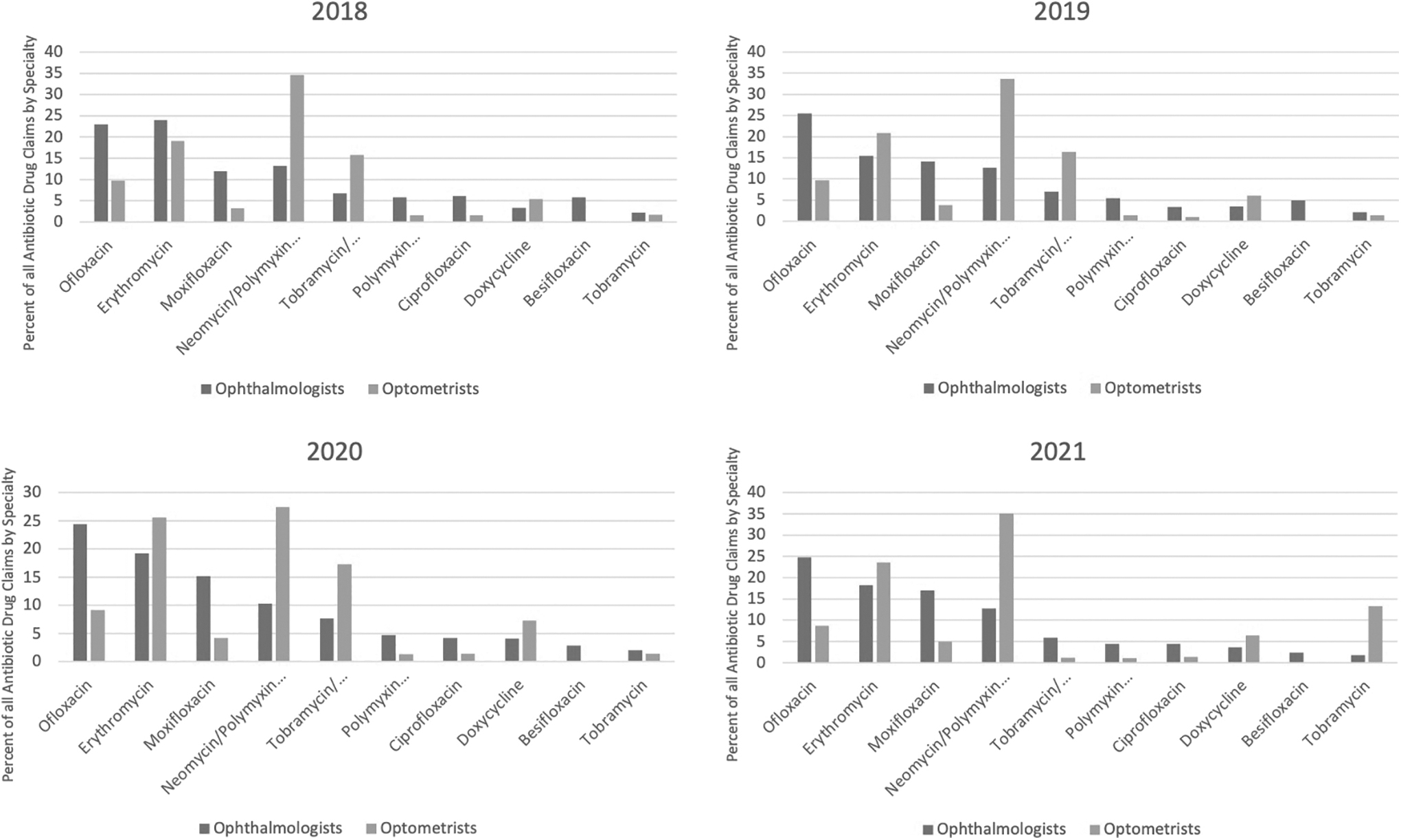
Antibiotic prescription trends of ophthalmologists and optometrists.
In 2021, 18.7% (611,628) of antibiotics prescribed by ophthalmologists were in a formulation combined with a corticosteroid, whereas 48.3% (233,400) of antibiotics prescribed by optometrists were combined with corticosteroids. Prescription rates of the top 10 most prescribed antibiotics did show meaningfully change over the study period for ophthalmologist and optometrists (Tables 3 and 4). For ophthalmologists, all medications except for doxycycline and tobramycin demonstrated that year was a predictor of total claims. Optometrists were somewhat more consistent with their prescription trends with no significant difference in prescription rates over the years for moxifloxacin, tobramycin/dexamethasone, doxycycline, and besifloxacin.
Ophthalmologist Prescription Rate Trends for the 10 Most Common Antibiotics, 2018 to 2021
P < 0.05 deemed statistically significant.
Optometrist Prescription Rate Trends for the 10 Most Common Antibiotics, 2018 to 2021
P < 0.05 deemed statistically significant.
Discussion
There has been large amount of research conducted regarding the over prescription of antibiotics in medicine and the resulting surge of antimicrobial resistance. However, there are limited data within the field of ophthalmology in terms of ophthalmologic and optometric prescription trends. Our study shows that over the study period, there was a slight decline in the amount of antibiotics that ophthalmologists are prescribing from year to year, and optometrist prescription rates have increased slightly. It is unclear why mean prescriptions per ophthalmologist decreased while those from optometrists increased. Both groups demonstrated slight drops in antibiotic prescriptions in the year 2020 (14.9% and 10.9%, respectively) that may be attributed to COVID-19. This decrease, however, was not caused by a decrease in cataract surgeries, as the number of surgeries were not shown to significantly decrease in that time. 9
While no specific research has been conducted regarding decreases in ophthalmologic and optometric prescriptions during the pandemic specifically, many articles have demonstrated decreases in national antibiotic prescriptions during this period determining that antibiotic prescribing rates in the United States fell 26.8% in 2020 compared with 2019.10–12 Many factors could contribute to this decline including decreased numbers of bacterial infections due to limited contact with other people and increased failure to seek medical attention. These reasons could also contribute to the decline in ophthalmologic and optometric prescriptions. There were 29,909 and 20,726 cases of diagnosed endophthalmitis in 2018 and 2019, respectively, and 957,088 and 977,057 cases of diagnosed keratitis in 2018 and 2019, respectively. Data are not yet available for 2020, so future studies will include analysis of change in infection rate during our entire study period to observe if these changes correlate with the changes in prescription patterns.
Our study demonstrates that ophthalmologists and optometrists have different prescription trends, which is likely related to the difference in clinical practice patterns. One main limitation of our study is the lack of clinical indication in the data to support the intent of antibiotic prescription. However, one clear discrepancy was the increased tendency for optometrists to prescribe combination antibiotic with steroid formulations. The effect of antibiotic steroid combination on the development of antimicrobial resistance remains unclear. To the best of our knowledge, there was no change in provider reimbursement during this time. Interestingly, while the number of optometry prescriptions rose slightly, the total cost of antibiotic claims decreased over the 4 years. The total cost of antibiotic claims also decreased for ophthalmology claims, although not significant. This could be attributed to the fact that the combined weighted average Part D premium across Prescription Drug Plans and Medicare Advantage Prescription Drugs reduced roughly 20% from 2018 to 2021. 13
Fluoroquinolones remain the most prescribed antibiotic by ophthalmologists, accounting for 48.6% of all antibiotic prescriptions in 2021 (Fig. 2a). They accounted for only 15.13% of antibiotics prescribed by optometrists in 2021 (Fig. 2b). Topical fluoroquinolones are often used as first-line treatment for ocular infections; however, up to 85% of methicillin-resistant isolates of Staphylococcus aureus have been found to be resistant to ophthalmic fluoroquinolones including moxifloxacin, which our study shows as the third most common antibiotic prescribed from 2018 to 2021. 14 In addition, fluoroquinolones are commonly used prophylactically. 15 This prophylactic use has been shown to significantly increase the percentage of bacteria such as Staphylococcus epidermidis on the conjunctival surface, thus indicating antibiotic resistance. 4

Similarly, aminoglycosides and macrolides, the second and third most commonly prescribed antibiotic class among ophthalmologists (20.5% and 18.2%, respectively) and the first and second most commonly prescribed among optometrists (49.5% and 23.5%, respectively), have been shown to demonstrate similar resistance patterns.4,16 Trends of drug prescriptions show that the most common drug prescribed by ophthalmologist was the fluoroquinolone, ofloxacin, increases in claims per 1,000 beneficiaries throughout the 4 years of this study, and that the year is shown to be a significant predictor of claim rate. This drug decreases for optometrists with year as a significant predictor.
The other frequently prescribed quinolone, moxifloxacin, also showed a significant increase in claims per 1,000 beneficiaries over the years among ophthalmologists and optometrists, with year once again being a significant predictor of claims per 1,000 beneficiaries. The most commonly prescribed macrolide, erythromycin, also showed a similar trend among both groups as did the steroid combination neomycin/polymyxin B/dexamethasone. These increases in prescription drugs such as fluoroquinolones and macrolides could continue to promote antimicrobial resistance and should be further investigated.
When looking at regional breakdowns of antibiotic prescriptions in the United States, the South consistently has both the highest number of claims and the highest average number of claims per provider for both optometrists and ophthalmologists. These findings are consistent with those of the U.S. Centers for Disease Control and Prevention that show that the South has more prescriptions of overall outpatient antibiotics than other regions of the United States. 17 The South also consistently has the highest number of claims per 1,000 population for optometrist prescriptions with 1.7 in 2021. Among ophthalmologists, the Northeast had the highest number of claims per 1,000 population with 12.5 in the Northeast and the West had the lowest with 9.0 in 2021 (Fig. 3).
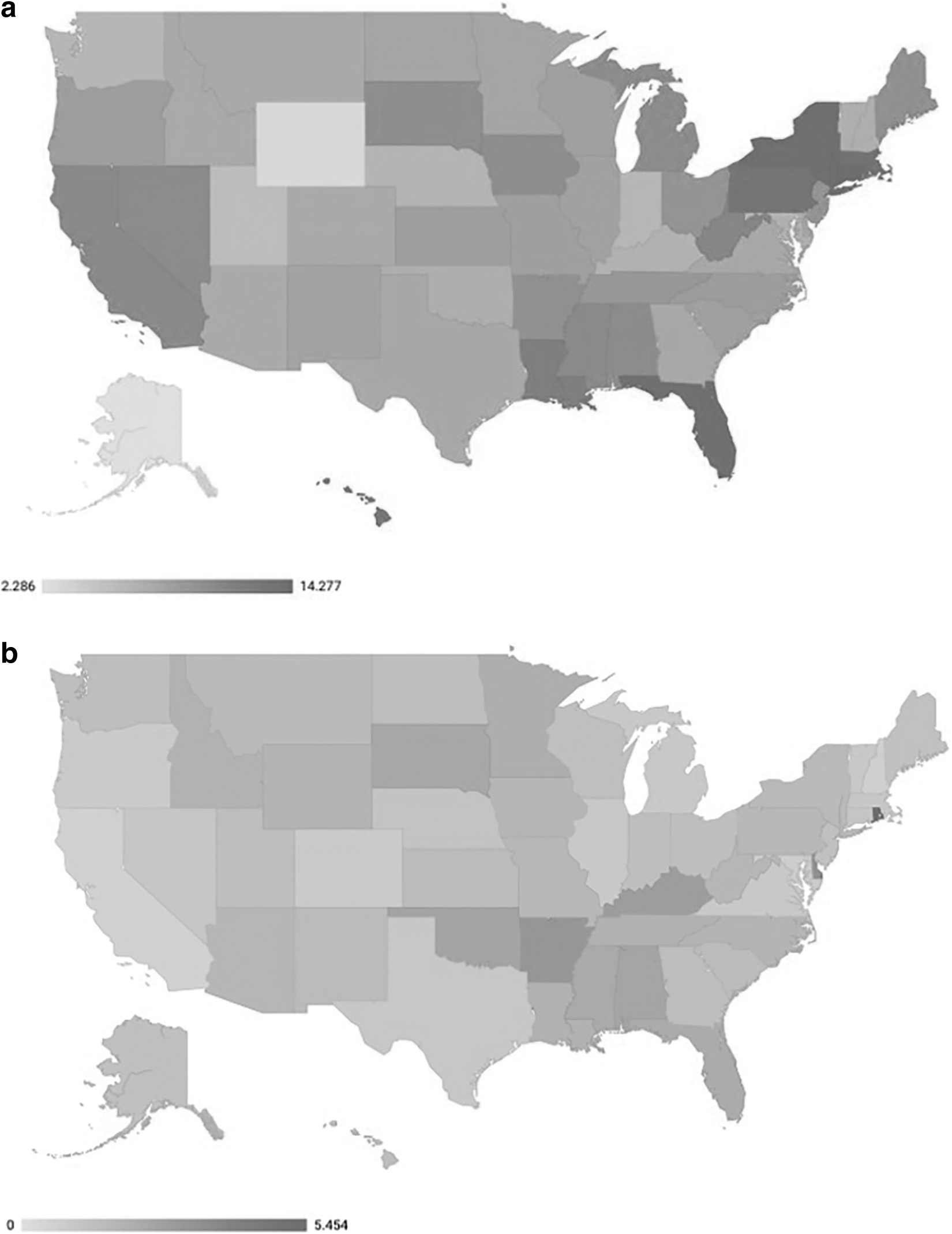
Heat maps of
In a regional breakdown of the average number of claims per provider, both ophthalmologists and optometrists demonstrated significant differences in the average number of claims per provider over the years (Fig. 2a, b). There was also a significant difference in the average number of claims per provider between all regions (Tables 3 and 4). More research is needed to determine the cause. Different possibilities for discrepancies between regions include varying levels of antimicrobial resistance awareness and stewardship or simply more patients per prescriber. Regions may also have varying levels socioeconomic factors that can lead to barriers to access of Medicare and health care in general. It has been shown that, despite the goal of Medicare Part D to make care more accessible, people from lower socioeconomic status tend to have a more difficult time receiving Medicare Part D coverage. 18 Further research needs to be conducted to determine the exact causes of these discrepancies.
Our study is limited by the scope of public use files of Medicare Part D, which includes eligible patients aged 65 years and older, those who have received social security disability insurance for more than 24 months, and those with end-stage renal disease. This limits the applicability of our results to other patient populations. As previously described, the database is also limited in the ability to delineate the clinical indication of the diagnosis for which each antibiotic was prescribed, and thus, we are unable to correlate our findings with an underlying disease etiology. The database does not disclose any specific drug dosing regimen, which may have been instructed by the provider. Our results have shown that prescribing patterns among ophthalmologists and optometrists have demonstrated significant changes in prescriptions of microbial resistance-promoting antibiotics. These patterns persist despite nation-wide attempts to control antimicrobial resistance. Further research into long-term ophthalmic antibiotic prescription trends and its impact on antimicrobial resistance is needed to maximize optimal care to patients.
Footnotes
Authors' Contributions
E.D.: Investigation, conceptualization, formal analysis, writing—original draft, data curation. J.Z.S.: Conceptualization, methodology, investigation, writing—review and editing. A.M.P.A.: Formal analysis. N.K.: Supervision, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.