
Abstract
Purpose:
To compare the efficacy of Brinzolamide-Brimonidine (BB) (1%+0.2%) with the gold standard Latanoprost-Timolol (LT) (0.005%+0.5%) in treating primary open-angle glaucoma (POAG) and ocular hypertension (OHT).
Methods:
A 1-year prospective study, spanning from May 2022 to May 2023, conducted at a tertiary eye-care hospital. Participants, aged 40–60, with a baseline intraocular pressure (IOP) >21 mm Hg, requiring a >30% reduction, were enrolled. Group A (n = 100) received BB, and Group B (n = 100) received LT. Outcomes were assessed at 1 month (IOP difference from baseline), 3 and 6 months (mean diurnal variations).
Results:
The mean age at presentation was 55.5 ± 4.5 years in Group A and 54.7 ± 4.2 years in Group B. At 1 month, Group A exhibited a mean IOP of 18.7 mm Hg, while Group B had 17.6 mm Hg, with no statistically significant difference (P = 0.53). No significant diurnal variation was observed in either group (P = 0.07). Target pressure was achieved in 88% of patients in Group A and slightly higher at 92% in Group B. Moreover, no serious side effects were reported, and compliance was higher in Group B (98%) compared to Group A (96%).
Conclusion:
Although LT showed slightly better and sustained IOP reduction, the difference was not statistically significant. Both BB and LT demonstrated comparable outcomes for managing POAG and OHT.
Introduction
Glaucoma remains one of the main causes of irreversible loss of vision worldwide. In 2010, it was estimated to have been responsible for over 8 million cases of blindness and by 2020, 79 million people worldwide will suffer from glaucoma.1–3
Glaucoma is characterized by increased or normal intraocular pressure (IOP), progressive optic neuropathy, and loss in visual field which corresponds to the optic nerve damage.2,3 Inadequate IOP control is a major risk factor for progression of glaucoma and increased IOP is associated with higher risk for vision loss.4,5 At present, IOP remains the only modifiable risk factor. Reducing the IOP to an individualized target pressure and maintaining it, decreases the risk of visual field loss and results are better. 6
A wide range of IOP reducing drugs with different mechanisms of action are available which include beta blockers, prostaglandin analogues, carbonic anhydrase inhibitors (CAIs), and alpha-2 adrenergic agonists. 6
Recommended first-line treatment for glaucoma is by use of a single IOP reducing medication. However, monotherapy may provide insufficient IOP reduction in some patients, thereby, necessitating the use of multiple IOP-lowering medications. Multidrug regimens may be complex and may increase the risk of preservative-related ocular symptoms. Fixed-combination medications, which provide 2 IOP-lowering therapies within a single solution, are available and may overcome some of these challenges.7–9
Fixed combination medications prevent drug washout, simplify dosing regimens, and may reduce costs. To address the barriers to optimal compliance with IOP reducing therapy, several fixed-combination medications, which facilitate instillation of 2 drugs in a single solution, have been developed.10–12
Among the fixed-dose combinations Latanoprost and Timolol has been commercially available for a long time with proven efficacy. However, the choice of fixed-dose combination for a given patient depends on the patient profile and tolerance of adverse effects. Head-to-head comparison between these fixed-dose combinations in terms of efficacy and adverse effects will help ophthalmologists to make the right choice.
The aim of this study is to compare the efficacy of 2 fixed-dose antiglaucoma drug combination of Brinzolamide-Brimonidine (BB) (1%+0.2%) with the gold standard of Latanoprost-Timolol (LT) (0.005% +0.5%) in primary open-angle glaucoma (POAG) and ocular hypertension (OHT).
Methods
This clinical double-masked randomized study was conducted from May 2022 to May 2023 at a tertiary eye-care hospital in Northern India. Comparison was carried out between 2 commercially available fixed-dose anti-glaucoma drug combinations, that is, Brinzolamide and Brimonidine (1%+0.2%; Simbrinza®; Alcon Laboratories, Inc., Fort Worth, TX) with the gold standard of Latanoprost with Timolol (0.005%+0.5%; Xalacom™, Pfizer, Inc., New York, NY) in POAG and OHT.
All already diagnosed cases of POAG and OHT, between 40 and 60 years old, who required >30% of reduction in IOP, that is, uncontrolled IOP with single anti-glaucoma drug, with IOP >21 mm of Hg, were included. Any case with history of previous ocular surgery within last 6 months, cases with primary angle closure suspect, primary angle closure glaucoma, and secondary angle closure/open glaucoma, pregnancy/lactating cases or any use of systemic medication known to affect IOP (unless both patient and dosage were stable for preceding 3 months and no change in dosage expected during study period) were excluded from the study. This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Ethics Committee (4825/2016). Informed consent was obtained from all participants included in the study.
Diagnostic criteria comprised significant optic nerve head damage and/or significant glaucomatous visual field changes. The idea was to reduce the IOP to lower-than-normal levels so that the progression of the glaucomatous damage is at least reduced, if not totally stopped. While, as far as the OHT cases are concerned, we selected only those patients in which there were chances of them getting lost to follow-up subsequently, or those who had a strong family history of glaucoma.
All the patients who were enrolled for the study underwent complete ophthalmological examination. The IOP was measured by Goldman applanation tonometry. The IOP measurement taken as mean diurnal IOP was the average of IOP measurements done at 8 AM, 10 AM, 2 PM, and 4 PM, at every follow-up. The IOP was adjusted for the central corneal thickness (CCT) reading, by anterior segment Spectral-domain optical coherence tomography (SD-OCT; Carl Zeiss, Jena, Germany) by standard method. The cornea was imaged with the anterior segment mode of the SD-OCT. Measurement of CCT with the integrated software was performed, and all optical coherence tomography (OCT) images were checked for correct identification of the corneal surface. High quality of OCT scans were selected for the study.
The patients enrolled also underwent pachymetry, OCT-retinal nerve fiber layer, gonioscopy, and perimetry for baseline evaluation and establishment of diagnosis.
In our study, there were several patients who were already on treatment with one of the drugs, which also formed part of the combination drugs that we used in our study. Most of them were on latanoprost or timolol, though a few of them were also on either brinzolamide or brimonidine too.
All patients underwent a “washout period” to discontinue any previous IOP-lowering medications before the study initiation. The washout period duration was recorded.
The period was observed to be 2 weeks for alpha-adrenoreceptor agonists and epinephrine-related agents and 4 weeks for all other agents, and 3 days washout period for CAIs.
The eligible patients were assigned randomly to either of the 2 treatment groups using randomization envelopes. Two groups were made, Group A who were prescribed a fixed-dose combination of BB at twice daily dosing and Group B who were prescribed LT combination, at once daily dosing. Patients in Group B also underwent electrocardiography and chest X-ray before starting the drugs to rule out any cardiac and respiratory illness. Patients were followed up at 1, 3, and 6 months. Outcome measures included difference in IOP from baseline to follow-ups, and mean diurnal variations at third and sixth month. All the patients were assessed for compliance and tolerability with a questionnaire, using binary responses. Clinical success was judged based on IOP lowering effect; patient satisfaction, compliance, and tolerability, answered in Yes or No. Patients were assessed for any adverse effects after the use of drug combination. The percentage of patients having the side effects of blurred vision, ocular hyperemia, eye irritation, dry eye, foreign body sensation, dry mouth, and change in iris color in both groups were calculated.
Statistical analysis
Data were entered in Microsoft excel sheet. Double entry and accuracy of entered data were rechecked. SPSS version-23.0 (SPSS, Inc., Chicago, IL) was used for statistical data analysis. For normality of data, Shapiro–Wilk test was used. Categorical variables have been presented as percentage and continuous variables as mean ± standard deviation. Repeated measures of analysis of variance was used to evaluate IOP values between treatment groups. Student's t-test was used for inter- and intragroup comparisons. Dunnett's test was performed for post hoc analysis. Fisher's exact test was used to evaluate adverse events. Confidence interval was kept at 95%. A P-value of <0.05 was considered statistically significant. The study adhered to an Intent-To-Treat analysis approach, considering all randomized subjects in the final analysis, maintaining the integrity of randomized allocation.
Results
Out of the 100 patients in the Group A (BB), the mean age was 55.5 ± 4.5 years, and there were 61 females (61%) and 39 males (39%). Whereas in the Group B (LT) (n = 100), the mean age of presentation was 54.7 ± 4.2 years, and there were 63 females (63%) and 37 males (37%). All patients were of Asian ethnicity. There were 146 cases of POAG and the rest were of OHT. There was no significant difference between the mean baseline IOP between the groups (range: 26–28 mm of Hg; P > 0.05).
While comparing IOP at 1- versus 6-month, the mean IOP changed from 18.7 mm Hg (Group A) and 17.6 mm Hg (Group B) in the first month to 18.2 mm Hg (Group A), and 17.3 mm Hg (Group B) at 6 months (Fig. 1).
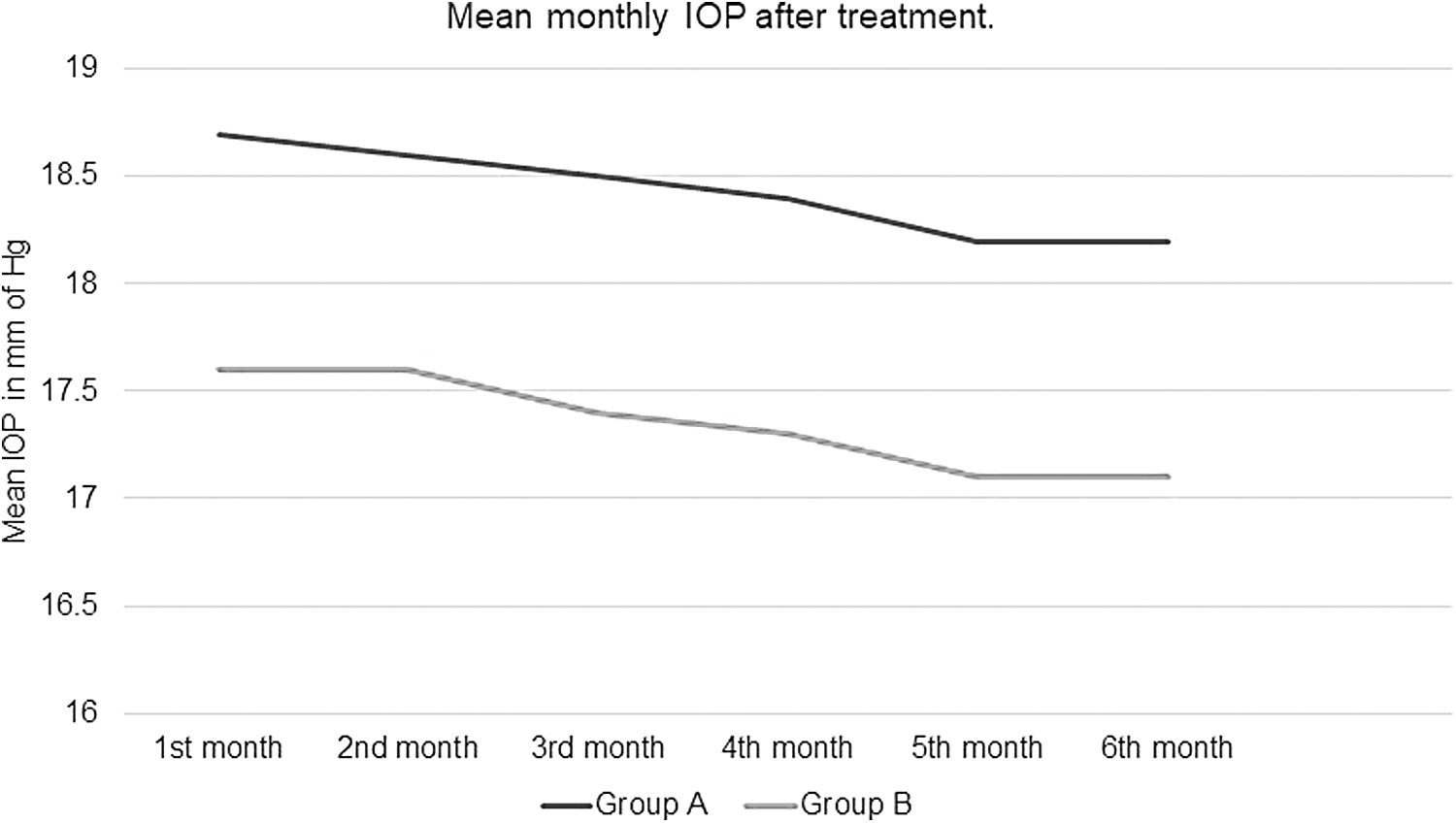
Mean monthly IOPs in Group A and Group B after starting the fixed-dose anti-glaucoma drugs. IOP, intraocular pressure.
The mean IOP at 3 months, at 0800 h, in Group A was 18.6 mm Hg (ie, a fall of 4.7 mm Hg) and in Group B was 17.6 mm Hg (ie, a fall of 5.2 mm Hg). Figure 2 depicts diurnal variation of mean IOP in both the groups every 4 h. The findings showed no significant diurnal variation in each group, and the IOP control was well maintained throughout the day in both the groups (P = 0.07). Figure 2 also shows change in mean IOP as diurnal variation from baseline IOP at 3 months.

Mean diurnal variation and change as diurnal variation from baseline IOPs in the Group A and Group B at 6 months after starting the fixed-dose anti-glaucoma drugs. The findings showed no significant diurnal-variation in each group and the IOP control was well maintained throughout the day in both the groups (P = 0.07, ANOVA test). ANOVA, analysis of variance.
The mean IOP at the end of 6 months, in Group A, was 18.6 mm Hg, and, in Group B, was 17.4 mm Hg. While comparing mean IOP between Groups A and B, lower mean IOP was observed in Group B (receiving latanoprost and timolol combination) as compared to Group A (receiving brimonidine and brinzolamide combination), but not statistically significant (P = 0.53).
Also, in Group A, the target pressure was achieved in 88% of patients, whereas in Group B, it was achieved in 92% of the patients.
The common side effects encountered by patients in both the group are enlisted in Table 1. None of them suffered from any serious side effects, which would warrant stopping the drugs. At the end of 6 months, the compliance was higher in patients of Group B on latanoprost and timolol combination (98%) as compared to the patients of Group A receiving brimonidine and brinzolamide combination (96%).
The Side Effects of Fixed-Dose Anti-Glaucoma Drug Combination Encountered by Patients of Group A and Group B
BB, Brinzolamide-Brimonidine; LT, Latanoprost-Timolol.
Discussion
Treatment for glaucoma hoovers on lowering IOP to a level at which the progression of damage is paused and the visual field is well preserved. Its first-line treatment involves a single IOP-lowering medicine. 13 Nonetheless, a prospective study reported that around 30% of patients need multiple anti-glaucoma drugs to attain and maintain their target IOP. 14 As a matter of a fact, the persistence with the IOP-lowering drugs have been reported low and found to be affected by the drug used and schedule prescribed.15–17 Thus, patients who require multiple concomitant drugs for IOP control are more likely to diverge from the prescribed schedule.
Multidrug regimens may be multifaceted and may increase the risk of preservative-related ocular symptoms and may potentially reduce overall drug exposure as a consequence of drug washout during closely timed sequential administrations; these hitches may reduce overall drug's effectiveness and decline patient's persistence with multidrug treatment regimens. 18 Fixed-combination drugs, that provide 2 IOP-lowering drugs in a single solution, are available and may overcome challenges like optimum adherence and persistence.
Earlier, prospective trials showed that when patients were switched from separate use of latanoprost (0.005%) and timolol (0.5%) to a fixed-combination of LT, the significant number of patients (71%) reported never-missing-a-dose after the switch, when compared to before the switch (59.3%; P = 0.0115). 19
As previously stated, that the drug combination of BB effectively maintains clinically relevant IOP reductions throughout the day. 20 Similarly in our study, the combination of BB showed effective IOP-reduction in cases of POAG and OHT.
Prostaglandin analogs generally provide the greatest IOP-lowering efficacy (up to 33% reduction), followed by β-blockers (25%), an α2-adrenergic agonist (25%), and CAIs (up to 20%). 21 The similar trends in percentage of IOP reduction (from baseline) have been detected among fixed-combination drugs like combining prostaglandin with timolol (reduction up to 35%–36%). 22 Moreover, a better mean IOP reduction from baseline with fixed-dose combinations containing timolol after 3 months of treatment (LT, 2.6–10.2 mmHg) was found similar with mean IOP reduction from baseline with BB at 3 months (5.4–8.8 mmHg).23,24 This supports our study and underlines the fact that both the groups are effective in IOP-lowering activity with comparable outcomes.
Concerning side effects, blurred vision (4.5%–6.1%) and eye irritation (2.8%–5.4%) were two of the most commonly reported ocular side effects with BB after 3 months of treatment.23,25 Hyperemia was reported in up to 3.3% of patients receiving BB in 2 clinical trials, an incidence similar to that reported with LT fixed combinations across multiple studies (up to 2.8%).24–26 Similarly, in our study, BB reported more cases of blurring of vision as the common side effect (4%) when compared to LT group (2%); whereas hyperemia was more seen with LT group (5%). Our study also noted high rates of patient satisfaction and clinical success. Both regimens were safe and well tolerated; however, once daily administration of LT was found to be more effective than twice daily administration of BB in reducing IOP in patients with POAG or OHT.
All the currently available fixed-combination IOP-lowering drugs provide similar IOP-lowering efficacy,,25,23 and mostly (except BB) contain β-blocker timolol in their combination. Because glaucoma incidence increases with age, patients with POAG/OHT tend to have comorbidities or therapeutic regimens (such as systemic β-blockers) that make them vulnerable to adverse drug reactions.27–29 Thus, when both the combinations (BB and LT) show comparable outcomes for management of POAG and OHT, BB expands the available fixed-combination options for patients who need effective IOP lowering and for those in whom use of β-blockers is contraindicated.
One of the key outcomes of this study was the comparable percentage reduction in IOP between the 2 treatment groups. This observation implies that both BB and LT can achieve similar therapeutic outcomes in terms of IOP control. Clinically, this offers flexibility to ophthalmologists and allows them to tailor treatment plans to individual patient needs and preferences. It is important to note that patient-specific factors, such as ocular comorbidities or systemic conditions, may influence the choice of therapy.
The idea of our study was basically to show that there is hardly any difference in the IOP lowering effects of 2 of the most commonly available combination of anti-glaucoma drugs available in the market today. Nowadays, there are a large number of anti-glaucoma drugs are available in a confusing variety of combinations and also with varying strengths of combinations. Our study will also go a long way in clearing this confusion about which combination of drugs to be started initially in patients requiring shifting of treatment with a single drug to those who require a 2-drug regime. To the best of our knowledge, no comparison has been made specifically between LT versus BB fixed-dose anti-glaucoma drug combination.
While this study provides valuable insights into the IOP-lowering efficacy of BB and LT, it does have certain limitations. The short-term follow-up period of 6 months restricts our ability to draw conclusions about the long-term safety and efficacy of these combinations. Glaucoma is a chronic condition, and assessing the durability of IOP control over an extended period is crucial. Additionally, the absence of assessments for field changes is a limitation. Evaluating visual field progression is essential in glaucoma management, and future research should consider incorporating this aspect.
Another aspect worth discussing is the selection of participants for the study. The inclusion criteria for patients already on medication and the subsequent washout period may raise questions about the representativeness of the study population. Ideally, drug-naïve patients would provide a clearer understanding of the efficacy of these combinations as initial therapy. It is acknowledged that the differences in dosing frequency between BB (twice daily) and LT (once daily) could potentially affect masking. It is essential to explore methods that minimize bias in future research, particularly in studies comparing drugs with different dosing regimens.
Conclusion
The combination of BB does not offer any major advantage over the LT in terms of IOP reduction, side effects, or compliance. Though, the LT combination shows slightly better and well-sustained IOP reduction, the difference is not statically significant. Thus, both the combinations show comparable outcomes for management of POAG and OHT and the combination BB can be used in the cases where LT is contraindicated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.