
Abstract
Purpose:
Demodex infestation is a risk factor for several ocular surface diseases. However, the prevalence of ocular Demodex infection in the ultra-high altitude population is not clear. This study aimed to compare the prevalence and factors associated with Demodex in populations residing in ultra-high altitude region and sea level areas.
Methods:
Consecutive patients who visited Shigatse People’s Hospital (> 4,000 m) and Shanghai Tongren Hospital (sea level) for eye complaints between January 2023 and January 2024 were included. Subjects were divided into ultra-high altitude and sea level groups. All subjects underwent eyelash epilation for ocular Demodex identification and counting. Demographic and lifestyle information was also collected.
Results:
A total of 517 subjects were eligible, including 255 subjects in the ultra-high-altitude group and 262 subjects in the sea level group. In the overall analysis, the prevalence of ocular Demodex infection was significantly different between the ultra-high-altitude and sea level groups (15.7% vs. 33.2%, P < 0.001). Multiple logistic regression showed that age, time spent outdoors, and makeup were associated with ocular Demodex infection in both groups. In addition, in the ultra-high-altitude group, people who wear sun hats outdoors were more likely to be infected with Demodex.
Conclusion:
The infection rate of ocular Demodex in the residents of ultra-high altitude area was significantly lower than that in the residents of sea level area, which may be related to lower ambient temperature, lower humidity, and higher solar radiation. Additionally, age, time spent outdoors, and makeup may be associated with ocular Demodex infection.
Introduction
Demodex mites are the most common ectoparasites found in mammals. 1 Only two species of Demodex mites, Demodex folliculorum and Demodex brevis, have been identified as capable of infecting humans. 2 These parasites tend to cluster in the openings of lash follicles, sebaceous glands, and meibomian glands on the ocular surface. 3 Moreover, cylindrical dandruff (CD), which refers to gelatinous debris, is commonly found attached to the base of the eyelashes. 4 Several studies have indicated that ocular diseases, particularly ocular surface diseases such as blepharitis,5,6 keratitis, 7 dry eye,8,9 meibomian gland dysfunction,10,11 conjunctival inflammation, 12 periocular basal cell carcinoma, 13 chalazion, 14 and pterygium,15,16 are closely associated with ocular Demodex infestation. As a result, ocular Demodex infestation has become a crucial factor in ocular diseases and has gained increasing attention.
Recent reports from around the world show that the incidence of Demodex has been found to vary from 13.5% to 89.3%, with considerable geographical differences (refer to Table 1).17–28 Currently, there are few reports on the ecology and basic research of Demodex that infects humans. 29 Temperature and humidity are the most studied environmental factors affecting the viability of Demodex.30,31 Studies have shown that Demodex mites that infect humans prefer mild temperatures (16–22°C) and high humidity (98%), suggesting that Demodex may thrive in warm and humid environments. 30
Prevalence of Ocular Demodex Infestation in Different Regions of the World in the Past 10 Years
Altitude data from this website (https://zh-cn.topographic-map.com/).
These studies only provide the year of the survey.
High-altitude regions refer to areas above 1,500 meters in altitude, where approximately 2% of the world’s population resides. 32 Moreover, the Society of Mountain Medicine identifies three distinct altitude regions: high altitude (1,500 to 3,500 meters above sea level), ultra-high altitude (3,500 to 5,500 meters above sea level), and extreme altitude (above 5,500 meters above sea level). 33 In addition, a negative correlation has been observed between altitude and environment temperature, and relative humidity. 34 Shigatse City, located in southwest Tibet at an average altitude of over 4,000 meters, has different climatic conditions compared to Shanghai, a coastal city at sea level. According to the China Meteorological Administration (http://www.nmc.cn/), the average annual temperature in Shigatse is 6.3°C and the average annual relative humidity is about 30%, whereas the average annual temperature in the Shanghai area is 17°C and the average annual relative humidity is about 70%. These results suggest that Shigatse is colder and drier than Shanghai. Furthermore, the health conditions in the Shigatse area are relatively poor, and the local diet is distinctive, with ghee tea and tsampa being the main foods, which are high in fat and cholesterol. 35
However, no studies have been conducted on the prevalence of ocular Demodex and its risk factors in the Shigatse region. Therefore, this cross-sectional study was conducted to determine the prevalence of ocular Demodex infection in the population of Shigatse and to compare it with the incidence of ocular Demodex infection in the population of Shanghai. We also investigated various factors that may influence the prevalence of ocular Demodex infection in the local population.
Material and Methods
Ethics statement
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Shanghai Tongren Hospital, Shanghai Jiao Tong University School of Medicine (no. 2023-035-01). All participants were given a full explanation of the study and signed written informed consent.
Study design and participants
A total of 255 patients were surveyed between January 2023 and January 2024 at the Shigatse People’s Hospital in Tibet, and 262 patients, matched for age and sex, were surveyed between January 2023 and January 2024 at the Shanghai Tongren Hospital in Shanghai. Patients were excluded if they met any of the following criteria: <18 years of age, prior ocular surgery history, topical or systemic treatments for Demodex mites, or any systemic disease. Each participant completed a questionnaire regarding demographic information (age, sex, educational level, living habit, etc.)
Lash sampling and microscopic mite counting
Eyelash sampling and Demodex counting under a microscope were performed by an independent physician blinded to the patients’ clinical information. 36 Briefly, 3 lashes with typical CD, considered pathognomonic for Demodex infestation, were selected in advance. Then, 3 lateral, middle, and medial lashes were removed from each eyelid under a slit lamp microscope (Nikon, Japan) and placed on a glass slide for detection. The number of Demodex mites was determined under the microscope after applying a drop of saline to dissolve the lash CD. Demodex infection was defined as the detection of 3 or more Demodex mites in 12 eyelashes.
Statistical analyses
Data were analyzed using SPSS version 26.0 (IBM Corporation, Armonk, NY). Normally distributed data are expressed as mean (standard deviation [SD]), and non-normally distributed data are expressed as median (interquartile range). The prevalence rates of ocular Demodex infection for subjects were calculated. The association between age, gender, lifestyle, and other variables and the risk of ocular Demodex infection was estimated by the odds ratio (OR) and its 95% confidence interval (CI). The chi-squared test or Fisher’s exact test was used to analyze categorical variables. Potential risk factors were evaluated by univariate regression analysis. Multivariate logistic regression models were used to assess the independent effect of risk factors. A P-value of less than 0.05 was considered statistically significant.
Results
A total of 255 subjects were included in the ultra-high-altitude group, including 130 (51.0%) males and 125 (49.0%) females, with an average age of 49.6 ± 18.7 years. In the sea level group, 262 individuals were included, with 142 men (54.2%) and 120 women (45.8%), and an average age of 51.5 ± 20.4 years. Age and sex (p = 0.28 and p = 0.46, respectively, Table 2). Detailed demographic data of the two groups are shown in Table 2.
Characteristics of the Whole Subjects
Pearson’s chi-squared test was used in the table, except additionally mentioned. †Student t test.
As shown in Table 3, the Demodex infestation rate in the ultra-high-altitude group was 15.7% among the 40 participants, significantly lower compared to the sea level group, where it was 33.2% among the 87 participants (p < 0.001).
Demodex Infestation in Ultra-High-Altitude and Sea Level Subjects
Participants in both groups were divided into four subgroups according to age (18–39 years, 40–59 years, 60–79 years, and ≥ 80 years). Table 4 shows the prevalence of Demodex according to age subgroup and gender. Subjects in the ultra-high-altitude group were predominantly 18–39 years of age (38.0%). Around 34.4% of the subjects in the low-altitude group were 18–39 years of age. There were significant differences in Demodex prevalence between age groups in both the ultra-high-altitude group (χ2 = 15.34, P = 0.002) and the sea level group (χ2 = 13.51, P = 0.004), with prevalence increasing with age (Fig. 1). More than 20% of subjects ≥60 years of age in the high-altitude group tested positive for Demodex. Among those over 80 years of age, the prevalence of Demodex infestation in the ultra-high-altitude group was 39.1%. In the sea level group, Demodex was most prevalent in the ≥ 80-year age group (48.8%), followed by the 60–79-year age group (41.7%).
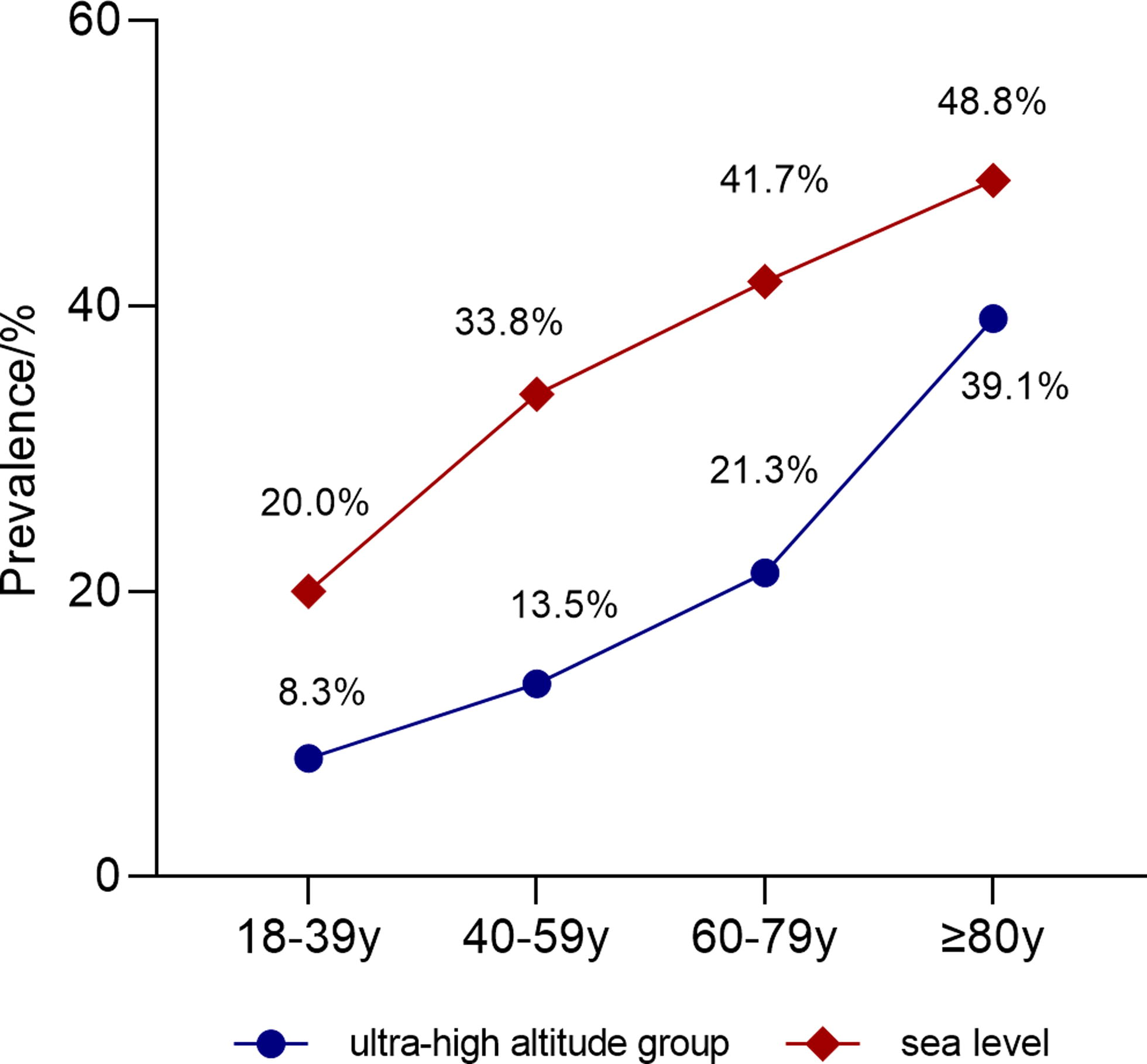
Ocular Demodex infection rates increased with age in both the ultra-high-altitude and sea level groups.
Prevalence of Demodex according to Age Subgroup and Gender
In the ultra-high altitude group, Demodex was found in 40 subjects, with 22 (16.9%) male and 18 (14.4%) female participants, and the difference was not significant (P = 0.58). Similarly, in the sea level group, the prevalence of Demodex infection was independent of sex (P = 0.41).
To investigate potential risk factors for ocular Demodex infestation, binary logistic regression analysis was performed, and the results are summarized in Table 5. Regarding the ultra-high-altitude group, univariate analysis revealed that age (P < 0.001), region of residence (P = 0.036), makeup (P = 0.044), and time spent outdoors (P = 0.004) were significantly associated with a higher prevalence of Demodex infestation. However, gender, educational background, smoking status, drinking status, eating spicy food, sharing towels, keeping a pet, and wearing a sun hat outdoors were not significant (all P > 0.05) in this group. Factors with probable significance (P < 0.2) were submitted to multiple logistic regression, 3 and the results revealed that age, makeup, time spent outdoors, and wearing a sun hat outdoors were significantly correlated with Demodex infection (all P < 0.05). In the sea level group, univariate analysis showed that Demodex infestation was associated with age, region of residence, makeup, and time spent outdoors (all P < 0.05). When all potential significant factors (P < 0.2) were submitted to multiple logistic regression, the results revealed that age was a risk factor for Demodex infestation (OR = 1.034, 95% CI:1.016–1.053; P < 0.001). Moreover, makeup (OR = 4.085, 95% CI: 2.005–8.322; P < 0.001), and time spent outdoors (OR = 0.415, 95% CI: 0.220–0.782; P = 0.006) were both associated with Demodex infestation in this group. Unlike the ultra-high-altitude group, wearing a sun hat outdoors was not correlated with Demodex infestation in the sea level group (OR = 1.641, 95% CI: 0.902–2.985; P = 0.105).
Risk Factors of Demodex Infection in Ultra-High-Altitude and Sea Level Subjects
Variables, where p < 0.20 were included in the multivariate ordinal logistic regression analysis. CI, confidence interval; OR, odds ratio.
Discussion
This study is the first cross-sectional study to compare the prevalence of ocular Demodex infections in populations at ultra-high-altitude with those at sea level. We recruited permanent residents from Shigatse (ultra-high altitude) and Shanghai (sea level), counted the prevalence of ocular Demodex, and analyzed some of the factors that may be associated with the prevalence of ocular Demodex, with the aim of filling the gaps in the study of ocular Demodex infections in ultra-high-altitude regions.
We found that the infection rate of the sea level population (33.2%, 87/262) was significantly higher compared with the ultra-high-altitude residents, which was 15.7% (40/255). This may be due to the fact that warmer and more humid environments may be better suited for the survival of Demodex. Zhao et al. found that the optimal temperature range for the survival of Demodex in a high humidity environment in vitro was 16–22°C30. They also observed that Demodex motility increased as the ambient temperature rose within the range of 16–30°C31. Moreover, it has been discovered that at a temperature of 36°C, high humidity (>95%) increases the survival rate of Demodex compared with low humidity. 37 Flores et al. reported a significant decrease in the number of patients who tested positive for Demodex during colder months. 24 Similar to these findings, Zhang et al. recently reported higher detection rates of Demodex in warmer and more humid indoor environments, and speculated that an increase in ambient temperature may cause Demodex to migrate to the skin, making them more easily detectable. 3 Therefore, in this study, the high Demodex infestation rate in the sea level region (Shanghai) may be related to its warmer and more humid environment compared with the ultra-high-altitude region (Shigatse).
Our finding of a Demodex prevalence of 15.7% among ultra-high-altitude residents is slightly higher than that reported by Gutiérrez et al., who found that Demodex was found in 13.5% of participants in Antofagasta. Antofagasta is located in the Atacama Desert, and higher temperatures (e.g., daytime surface temperatures up to 60°C) and lower humidity (17.3%–28.8%) have been reported in the Atacama Desert compared with Shigatse.38,39 Antofagasta tends to be warmer but drier than Shigatse, but both regions have strong ultraviolet exposure and prolonged solar radiation.17,39
Humans receive solar radiation mainly outdoors, and the amount of time spent outdoors may indirectly reflect, to some extent, on the amount of solar radiation received by humans. Our study found that in the ultra-high-altitude group, participants who spent more than 1.5 h per day outdoors were less likely to be infected by Demodex. Similarly, in the sea level group, participants engaging in outdoor activities for ≥1.5 h per day exhibited a 0.42-fold decrease in the risk of ocular Demodex infestation compared with participants with ≤1.5 h of daily outdoor activity exposure. Interestingly, we also found that in the ultra-high-altitude group, participants who used sun hats outdoors appeared to be 2.5 times more likely to be infected with Demodex than those who did not use sun hats. In the sea level group, outdoor sun hat use was not associated with Demodex infection. These results suggest that solar radiation may affect Demodex. Similarly, Gutiérrez et al. have proposed that exposure to the sun, including ultraviolet rays, may affect Demodex. 17
We found that age was positively associated with Demodex infestation. In our study, participants were divided into four subgroups according to age, and we found that the incidence of ocular Demodex increased with age in both the ultra-high-altitude and sea level groups. Our results are consistent with many other studies. 40 Some scholars also believe that aging causes damage to the skin barrier, resulting in dry skin and impaired immunity, which may be conducive to the proliferation of Demodex. 41 We also examined whether gender was associated with ocular Demodex infection. In our study, 16.9% of males and 14.4% of females in the ultra-high-altitude group had ocular Demodex infections, but this difference was not significant. Similarly, there was no significant difference in ocular Demodex infection rates between men (31.0%) and women (35.8%) in the sea level group. Most previous studies have shown that gender is not a risk factor for Demodex infection,40,42 but some studies have suggested that gender is associated with Demodex infection. 43 In our study, the rates of Demodex infection were comparable between males and females.
Living in rural areas, 3 educational level, 44 and pet ownership 45 have been recognized as risk factors for Demodex infestation. In this study, the above factors, except residence, had no significant effect on the presence of Demodex according to univariate regression analysis and multivariate logistic regression analysis. A comprehensive literature search revealed that the relationship between towel sharing and Demodex infection in adults is currently inconclusive. While some studies have indicated a potential association between towel sharing and Demodex infection, 46 others have not.47,48 Our study did not find a significant association between towel sharing and Demodex infection. Therefore, further research is needed to clarify the relationship between towel sharing and Demodex infection. Regarding residence, univariate regression analysis revealed that in the ultra-high-altitude group, the risk of Demodex infection was about twice as high for those living in rural areas compared with those living in urban areas, which was consistent with that in the sea level group. However, multivariate logistic regression analysis revealed that living in rural areas was not associated with Demodex prevalence.
In addition, we also found that a spicy diet, smoking, and drinking habits were not conducive to Demodex infection factors. Some studies have shown that in young populations (university students and young adults), makeup use appeared to reduce Demodex infection rates (34.3% of 160 Demodex-positive participants used makeup and 29.4% of 17 Demodex-positive participants used makeup, respectively).49,50 However, in a study that also involved young adults (university students), Vargas-Arzola et al. found that 47.4% of 118 people infected with Demodex used makeup, but there was no statistical difference compared with those who did not use. 28 In this study, we found that in the ultra-high-altitude group, the infection rate of Demodex in the subjects who used makeup was three times that of those who did not use makeup. In the sea level group, the ratio increased to four times. We speculate that since the average age of our study subjects was close to 50 years, they may have poorer hygiene practices compared with younger people, and that clogged skin pores caused by not removing or incompletely removing makeup increases Demodex infection.
The study has some limitations. Collecting clinical data in ultra-high-altitude areas is challenging due to inconvenient local transportation and negative attitudes toward medical treatment among the residents of Shigatse. Due to the harsh environment in the ultra-high-altitude area, our research team spent a relatively short time on this study. The study had a comparatively small sample size, which needs improvement in future research. Demodex infections may be related to several factors. This study focuses on the environmental factors and some lifestyle habits of residents in Shigatse and Shanghai. There were differences in other lifestyles of the residents of the two cities, such as dietary habits (high-fat diet or not), which may need to be further investigated to determine their association with Demodex infection.
To conclude, our cross-sectional study is the first to report a significantly lower ocular Demodex infection rate in ultra-high-altitude residents compared with sea level populations (15.7% vs. 33.2%). This may be associated with lower ambient temperatures, lower humidity, and higher solar radiation in the ultra-high-altitude region (Shigatse) compared with the sea level region (Shanghai). Moreover, we have found that age, time spent outdoors, and makeup are significantly associated with ocular Demodex infection in both populations at ultra-high altitude and at sea level. In additionally, at ultra-high altitudes, individuals who wear sun hats while outdoors are more likely to acquire Demodex infection, further suggesting that increasing sun exposure appropriately may reduce Demodex infection.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work has been supported by the
Data Availability
Data are available on reasonable request from the corresponding author, Q.Q. Data are not publicly available due to some restrictions.