
Abstract
Objective:
To describe the clinical effects of a novel, combined ocular lubricant for treating patients with dry eye disease.
Methods:
A noncomparative, retrospective cohort of 67 eyes (67 patients) with a confirmed diagnosis of dry eye disease using the ocular surface disease index (>12), tear osmolarity, and ocular surface parameters (noninvasive break-up time, meniscus height, and meibography) evaluated using the Cornea550 were included. All patients were treated with a combination of 0.5% carboxymethylcellulose, glycerin 0.9%, and trehalose 3% with a dosing regimen of one drop four times a day for 1 month with a final evaluation of the same parameters.
Results:
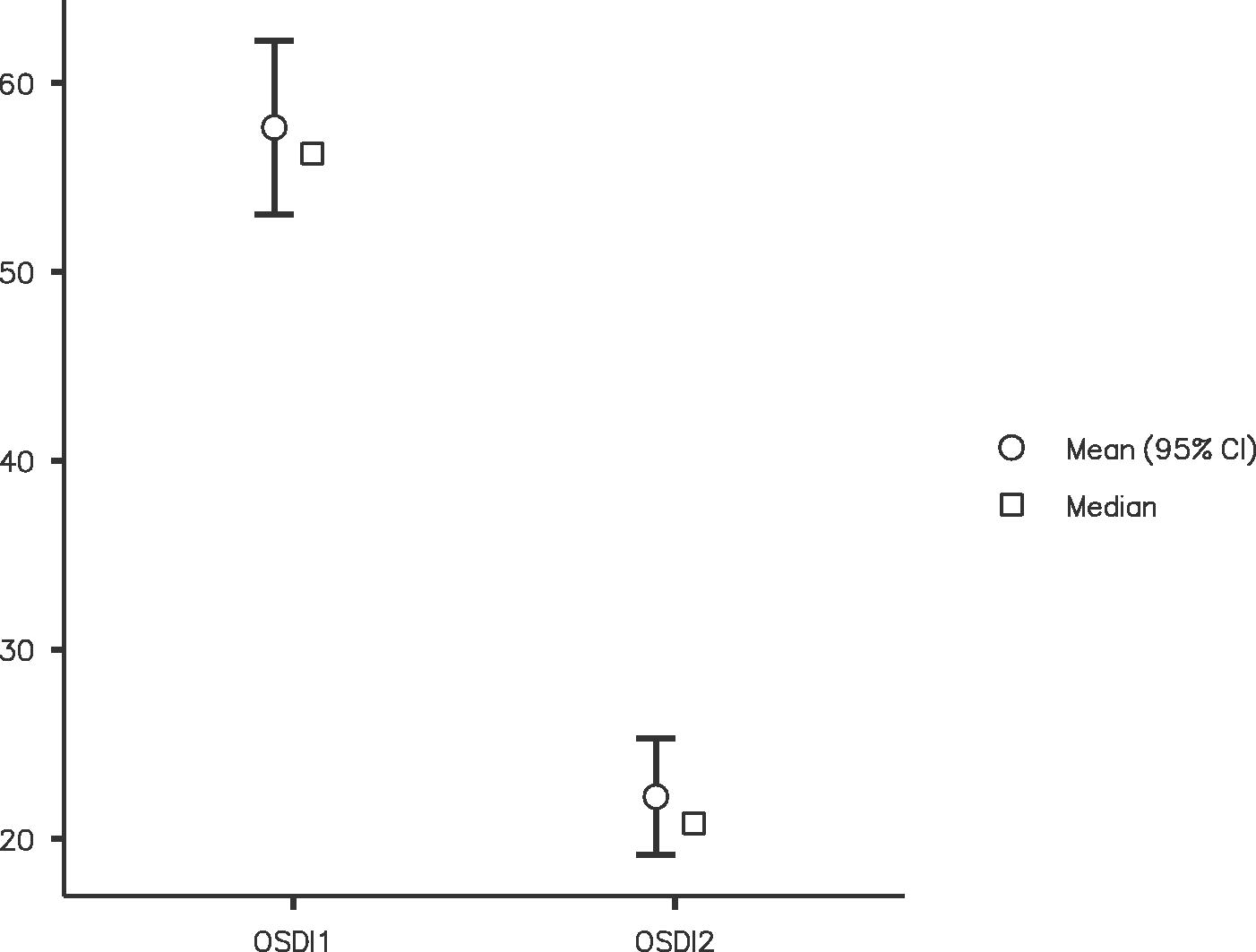
We included 67 eyes (80.6% females) with a mean age of 48.3 ± 16.2 years (standard deviation [SD]). In total, 37% of the subjects had comorbidities such as hypothyroidism (9%), ocular rosacea (4%), Sjogren’s syndrome (4%), and arterial hypertension (4%). Of these, 34% were taking systemic medications and 56.7% had previous ocular surgery. The mean ocular surface disease index score before treatment was 57.6 ± 17.2 (SD) and 22.2 ± 12.9 points (SD) after treatment (P < 0.05). Other parameters such as noninvasive break-up time, meniscus height, and meibography improved without a statistically significant difference.
Conclusion:
Cristal Tears Plus is a novel, combined, and multipurpose treatment for dry eye disease.
Introduction
Dry eye disease (DED) is a multifactorial entity of the ocular surface characterized by loss of homeostasis and instability of the tear film, accompanied by ocular symptoms, hyperosmolarity, ocular surface inflammation, and neurosensory abnormalities.1,2 Since 1995, patients with DED have been classified as either aqua-deficient or evaporative. Recently, the Dry Eye Workshop II (DEWS II) has recognized a third clinical group with a combination of water deficiency and excess evaporation called mixed DED.3,4 The prevalence of DED varies between 5% and 50% in different studies, with the evaporative type being the most frequent (65%–70%).5,6 The first line of therapy is the use of topical lubricants for different types of DED. The development of different diagnostic tests with higher sensitivity and specificity (>90%–95%) including validated dry eye questionnaires, 7 tear film osmolarity testing (TearLab Corp, Escondido CA, USA), 8 and computerized ocular surface parameters such as the noninvasive break-up time (NIBUT), meniscus height, and meibography have changed the state-of-the-art in DED diagnosis.9,10 Tear film osmolarity is the concentration of dissolved solutes in a solution (solvent), which is independent of its size, density, molecular weight, or electric charge. Cristal Tears Plus (CTP) is a novel lubricating eye drop composed of carboxymethylcellulose 0.5%, glycerin 0.9%, and trehalose 3%, is a combined ocular lubricant for the treatment of aqua-deficient, evaporative, and mixed DED. It has an osmolarity of 290–295 mOsm/L and comes in a multidose bottle with potassium sorbate as a preservative. 11 This study aimed to evaluate the clinical effect of CTP in the treatment of patients with DED diagnosed using a validated OSDI questionnaire, tear film osmolarity, and ocular parameters measured by an anterior surface topographer, Cornea550 (Essilor, Creteil, France), after treatment with CTP with a dosing regimen of one drop four times a day for 1 month.
Methods
This retrospective, open-label, noncomparative cohort study included 67 patients (67 eyes) in a consecutive manner until the estimated sample size was achieved. All patients came from the private practice clinic of the authors (P.-I.N.-N., A.C.-A., and G.A.-R.) and were recruited between August 2021 and February 2022. A complete ophthalmological examination and the ocular surface disease index (OSDI), a dry eye disease questionnaire validated in Colombian Spanish was administered to patients in whom a DED diagnosis was suspected. 12 All participants with an OSDI score >12 were included in the study. Other diagnostic parameters included in the study were tear film osmolarity (TearLab, California, USA), NIBUT, meniscus height, and meiboscore, which were evaluated using the anterior surface topographer Cornea550 (Essilor, Creteil, France). Tear film osmolarity is the concentration of dissolved solutes in a solution (solvent), which is independent of its size, density, molecular weight, or electric charge. With innovative and more accurate testing with anterior surface topographers, we can decrease intra- and interobserver variability to reduce measurement bias. The standardization of the clinical parameters in dry eye patients evaluated at the slit lamp, such as tear film break-up time (BUT), tear meniscus height, and meibomian gland (meibography) distribution increases the diagnostic accuracy of these tests in clinical and research settings. Cornea550 (Essilor, Creteil, France) is a reflection corneal topographer, anterior surface, which has an integrated video camera with a high resolution and an infrared LED system (890 µm) that allows the quantitative and qualitative evaluation of the tear film and meibomian glands. It evaluates 6144 spots on the ocular surface with a work distance of 78 mm. This topographer evaluates the degree of inflammation of the ocular surface, tear meniscus height, NIBUT, and meibomian gland population, allowing direct visualization of their morphology and estimating their proportion in the superior and inferior eyelids. There is a direct correlation between the number of meibomian glands and the lipidic component, which is a deficiency factor in patients with evaporative dry eye. The Cornea550 device classifies patients using a scale called meiboscore, which quantifies the loss of the meibomian gland population: 0 no loss; 1 < 33; 2: 33%–66%, and 3 > 66%. These results are highly correlated with meibum production and the functional state of the glands involved in the antievaporative effect of the tear film. 13 A regimen of one drop every 6 h (four times per day) for 1 month was administered, without the use of any other topical or systemic treatment, and a new evaluation was performed with the same baseline parameters. The primary outcome of this study was to estimate the difference between OSDI scores before and after treatment. Inclusion criteria were: subjects >18 years old with an OSDI score >12 before treatment, who had no DED treatment at the start of the study, or those who had suspended the treatment at least 1 month before, and had signed the informed consent. Subjects who reported allergies to any compound from CTP, pregnant or lactating women, subjects with allergic or infectious conjunctivitis, a history of Stevens-Johnson syndrome, ocular pemphigoid or graft–host disease, and glaucoma patients with topical treatment were excluded. The quantitative variables measured were age, OSDI score, tear film osmolarity, NIBUT, meniscus height, and meibography. The qualitative variables included sex, occupation, autoimmune disease, systemic medications, and previous ocular surgery. All included subjects signed an informed consent and habeas data format.
Sampling
A sample was designed for a cohort study using Epidat 4.1 (Sergas, Spain) expecting a standardized difference for the OSDI score of 70% after treatment with CTP for one month. A confidence interval of 95% and a standard deviation of 2.00 were used for 66 eyes. The subjects lost during follow-up were calculated to be 20%, resulting in 13 more eyes for a total sample of 79 eyes.
Data analysis
A univariant analysis for the quantitative variables was performed to determine the distribution of the data (normality distribution of data was evaluated using the Kolmogorov–Smirnov test) and central tendency and dispersion measures were estimated. Qualitative variables were analyzed using frequencies and proportions. Bivariant analysis and correlation tests were used for quantitative variables (Pearson and Spearman tests) and qualitative variables (chi-squared, Mann–Whitney, and Kruskal–Wallis tests). Statistical analyses were performed using SPSS V21 (IBM, Armonk, New York, USA) and Jamovi (Jamovi Project V1.2).
Results
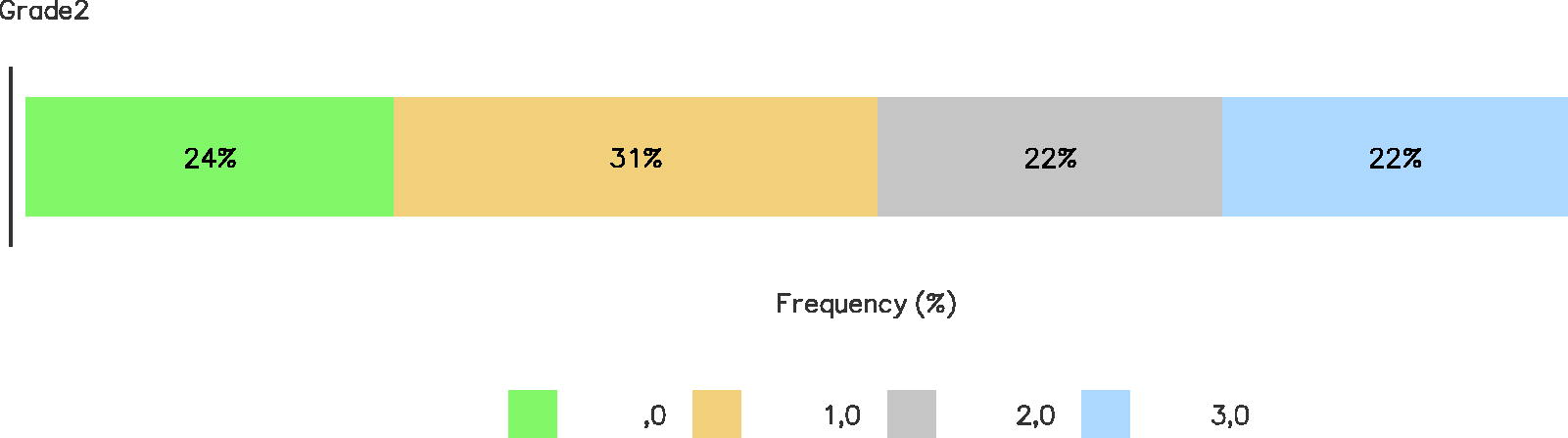
We finally included 67 eyes (67 patients, 80.6% females) with a mean age of 48.3 ± 16.2 years (SD). 67.2% were right eyes. Regarding the main daily activities of the subjects included in the study, 21% performed home activities, 15% were business administrators, 9% were lawyers, and 7% were engineers. In total, 37% of subjects had comorbidities including hypothyroidism (9%), ocular rosacea (4%), Sjogren’s syndrome (4%), and arterial hypertension (4%). Of all, 34% of subjects were under systemic medications such as thyroid hormones (18%), antidepressants (1%), beta-blockers (1%), and others reported different combined regimens. In total, 56.7% had previous ocular surgery as LASIK refractive surgery (24%), superficial refractive surgery (4%), phacoemulsification surgery (4%), or blepharoplasty (4%) (Table 1). The pre- and posttreatment results included a validated DED questionnaire, OSDI (mean pre- and posttreatment, 57.6 ± 17.2 and 22.2 ± 12.9 points) (Fig. 1), tear osmolarity (pre- and posttreatment, median values of 320.97 ± 20.43 and 317.48 ± 16.95 mOsm), NIBUT (pre- and posttreatment, median value of 6.80 ± 7 and 8.70 ± 11.1 s) (Fig. 2), tear meniscus height (pre- and posttreatment, median value of 0.21 ± 0.10 and 0.23 ± 0.07 mm) (Fig. 3), and meibomian gland population (pre- and posttreatment, a percentage of 45.7% and 43.3%, respectively). Regarding DED severity using the OSDI questionnaire, before treatment, 91% (61 eyes) of eyes had severe dryness, 7.5% (5 eyes) moderate, and only 1.5% (1 eye) were diagnosed with mild disease (Fig. 4) and after treatment, 22.4% (15 eyes) showed severe and moderate conditions, 31.3% (21 eyes) had mild disease and 23.9% (16 eyes) showed no disease (Fig. 5). With innovative and more accurate testing with anterior surface topographers, we decreased the intra- and interobserver variability to reduce measurement bias in contrast to clinical evaluation at the slit lamp of patients with DED.
OSDI 1–2 OSDI, ocular surface disease index.

(1) NIBUT 1–2 (Non-invasive break-up time).

(1) TMH 1–2 (Tear Meniscus Height).

(1) Dry Eye Severity 1.
(1) Dry Eye Severity 2.
Quantitative/Qualitative Variables
Mean − SD (standard deviation) / aMedian − IQR (interquartile range).
NIBUT, noninvasive break-up time; OSDI, ocular surface disease index.
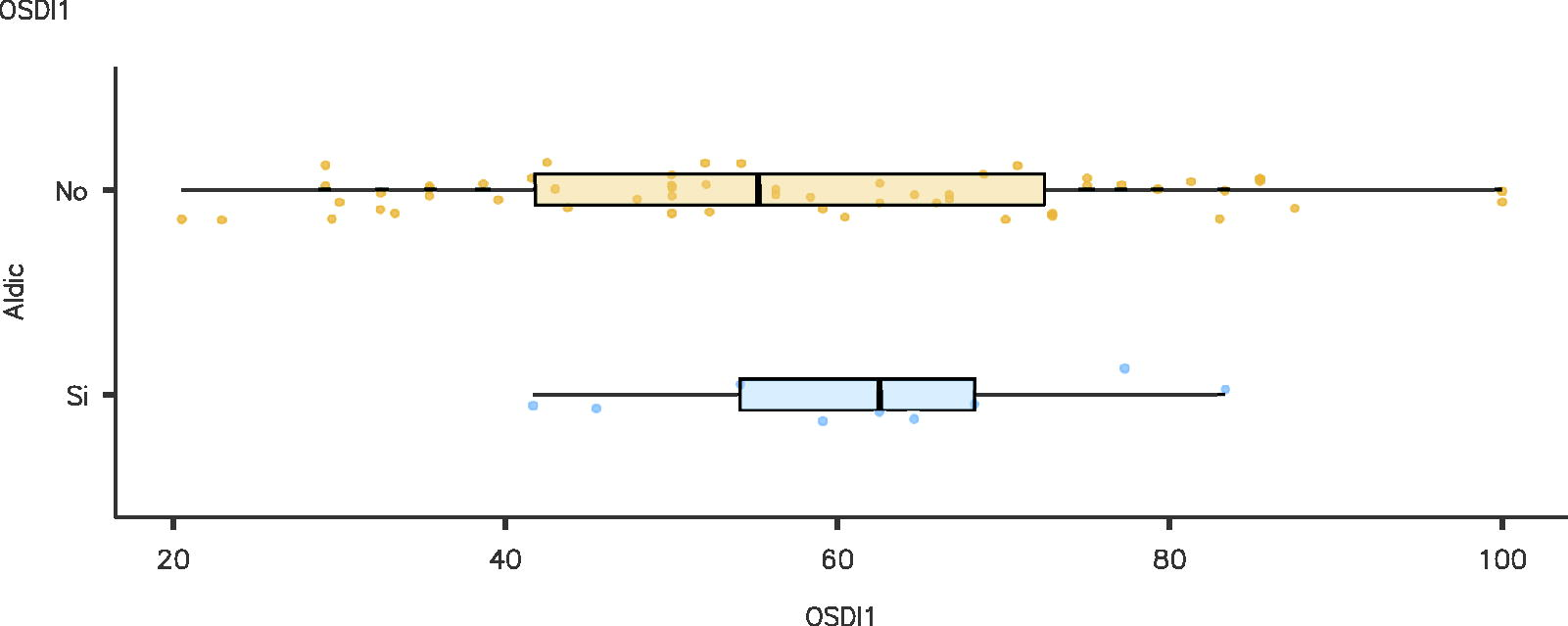
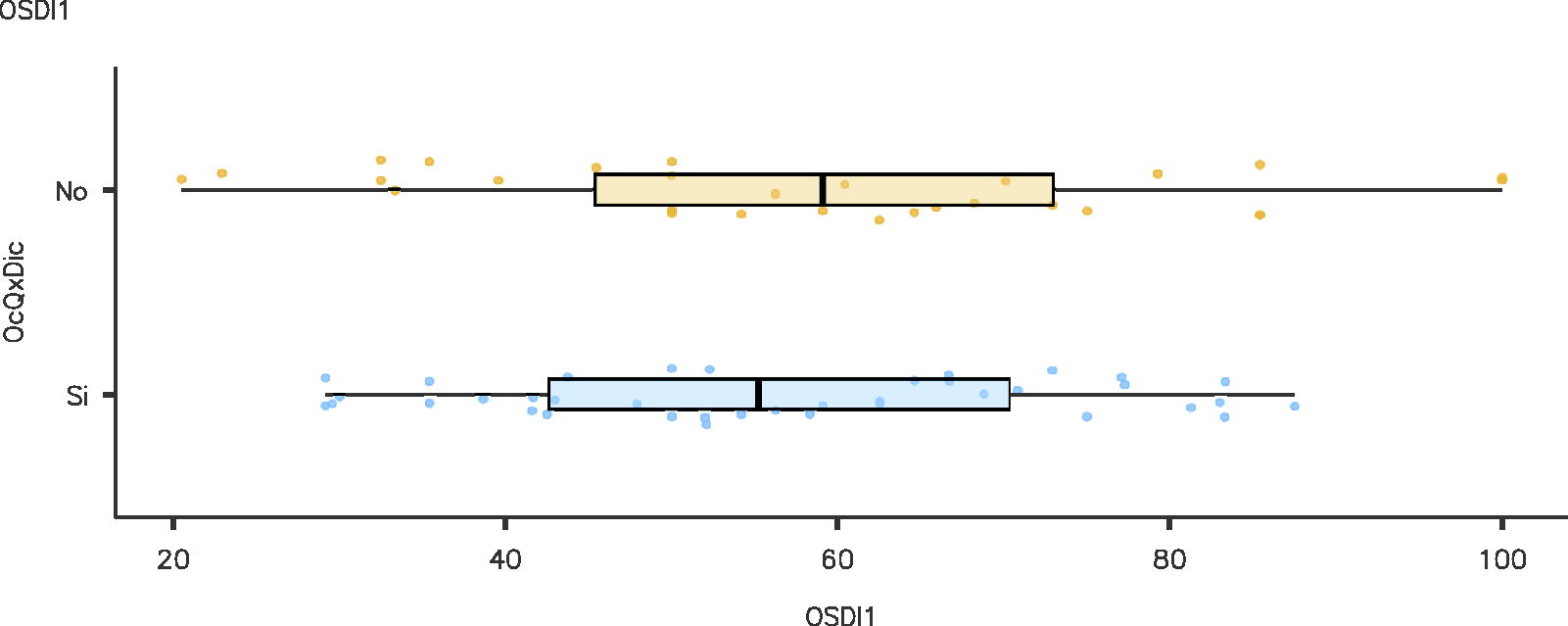
We did not find an association between dryness and the presence of autoimmune disease (Wilcoxon test, P = 0.42) (Fig. 6) or between dryness and previous ocular surgery, either (Analysis of Variance, ANOVA test, P = 0.30) (Fig. 7). Subgroup analysis by disease severity confirmed the change in OSDI score in the moderate and severe groups of patients (P = 0.022 and P = 0.000, respectively) with a statistical trend change in the NIBUT parameter in eyes with moderate dryness before and after treatment (P = 0.060).
(1) OSDI/autoimmune disease.
(1) OSDI/previous ocular surgery.
Discussion
We report for the first time the clinical experience of using a novel, combined, multipurpose ocular lubricant (carboxymethylcellulose 0.5%, glycerin 0.9%, and trehalose 3%) in a retrospective cohort of 67 eyes (67 patients) with aqua-deficient, evaporative, and mixed DED. All patients were treated with CTP at a dosing regimen of four times a day for 1 month without using any other topical or systemic treatment, such as steroids or oral anti-inflammatory medications.
After the treatment, we found a statistically significant difference in the OSDI score (primary outcome) from 57.64 ± 19.16 (SD) to 22.22 ± 12.93 (SD) points. Other evaluated parameters such as tear osmolarity, NIBUT, and meniscus height also showed improvement without a statistically significant difference (P < 0.05). There was no change in the percentage of meibomian gland loss before and after treatment. The standardization of diagnostic ocular surface tests in patients with DED with new computer-based technology (Cornea550, Essilor, Creteil, France) has increased the reliability of parameters such as noninvasive tear film BUT (NIBUT), tear meniscus height, and meibomian gland evaluation in clinical settings. These anterior surface topography systems decrease intra- and interobserver variabilities. Regarding the stratified analysis performed by disease severity, we observed a reduction in the proportion of eyes with severe disease (from 91% to 22%) and a significant increase at the end of the study in the mild dry eye group (from 1% to 31%. At the end of the study, 24% of eyes were normal according to the OSDI score.
DED is a multifactorial disease that affects a large part of the world’s population, with a prevalence of 5%–50%.4–6 It is more frequent in women, older adults, Asians, and in some health conditions such as autoimmune diseases, especially Sjogren’s syndrome. Some risk factors for DED are modifiable such as reduced time spent using computer screens or cell phones 6 and the time of use of contact lenses but also improving the degree of severity of endocrine diseases that affect the production of tears such as hypoestrogenism, hypoandrogenism, and hypothyroidism. It is recommended to improve the environmental conditions of low humidity with an excess evaporation rate (ventilation systems, air conditioning, and screen use time). In addition, the rational use of antihypertensive drugs such as beta-blockers, antiallergics (antihistamines), antidepressants (serotonin reuptake inhibitors, SSRIs), anxiolytics, and antiacne therapy (isotretinoin). 4
One of the novel characteristics of CTP is the presence of the 3% trehalose molecule, a disaccharide with bio- and osmoprotection properties used by certain plants and nonvertebrate animals to defend themselves against periods of extreme drought, using their water retention capacity in rainy seasons. This molecule was originally described by Marceline Berthelot in the XIX century, which allows cells to survive in adverse environments and anhydrobiosis.13,14 Trehalose has a high-water retention capacity with bio and osmoprotection properties. Different in vitro and in vivo studies have confirmed that trehalose prevents apoptosis and protects corneal cells against oxidative stress caused by UV radiation, accelerates corneal wounding, and decreases the concentration of inflammatory cytokines in the conjunctiva. It also has other properties such as intracellular cleaning (autophagia) and decreased inflammation (lower concentration of interleukin 6 [IL-6], IL-8, tumor necrosis factor [TNF], and MMP-9).15,16
In 2007, Chiambaretta and the Trehalose Study Group conducted a randomized, controlled, multicenter clinical trial (France and Tunisia) to evaluate the efficacy and safety of a combination of hyaluronic acid (HA) trehalose (TH) (n = 52) and HA (n = 53) in patients with dry eye syndrome. They used ocular lubricants at doses of three to six times a day for a period of 84 days with staining of the corneal surface as the primary outcome, using the Oxford score on day 35 of the study. In addition, they evaluated the results using the validated OSDI questionnaire, Schirmer test, NIBUT, and conjunctival hyperemia at the beginning and on days 35 and 84 of the study, respectively. The results of this study demonstrated a reduction in Oxford staining of −2.5 ± 2 (HA + TH) versus −2.7 ± 1.7 (HA) (95% CI: −1.34 to 0.40) demonstrating a noninferiority result for the group with a combined treatment of HA + TH compared to the control group (HA). In addition, they reported a reduction in the OSDI score of −20.6 ± 17.2 (HA + TH) versus −17.6 ± 16.2 (HA) points without finding a statistically significant difference (P = 0.060). 17 In our study, the degree of severity of DED observed after treatment decreased in a greater population of patients with severe DED similar to the observed effect found by Chiambaretta et al. (P = 0.04), with the appearance of a proportion of healthy eyes after one month of treatment. In our study (n = 67), we observed an important decrease in the OSDI score with a reduction of 35.4 ± 4.4 points (P < 0.001, 95% CI: 31–39.8) after a month of treatment compared to the initial values. Similarly, we agree that there was an increase in the proportion of eyes with less severe disease after treatment (1 m) in all subgroups (especially in mild DED), and the appearance of a new subgroup of patients with normal OSDI scores confirmed the clinical effectiveness of CTP (from 0% to 23.9%). The percentage of participants with mild DED increased from 1.5% to 31.3%. Our results also confirmed that the main subtype of DED was the evaporative with a median meniscus height prior to treatment of 0.21 mm, within the normal cutoff value, with a small increase in this parameter at one month after treatment (0.23 mm).
In 2022, Barabino et al. updated the classification of ocular lubricants into three categories based on their interaction with the ocular surface: wetting agents, multiple-action tear substitutes, and ocular surface modulators. Wetting agents lubricate the ocular surface for a limited time, whereas multiaction tear substitutes can improve quality and quantity without interacting with it. Rather, ocular surface modulators interact with and influence the ocular surface to decrease signs of DED. Among the main ingredients that make eye lubricants are agents that increase the viscosity of the tear film, electrolytes, osmotic protectors, lipid agents, antioxidants, and preservatives. Viscosity-increasing agents are the most frequently used and are also known as demulcents or lubricants, including cellulose derivatives, dextran, gelatins, liquid polyols, polyvinyl alcohol, and povidone (FDA). It has been demonstrated that these molecules increase the thickness of the tear film and its retention; in addition, their ability to retain water prevents evaporation. 18 Carboxymethylcellulose, a component of CTP at 0.5% concentration, is a vegetable derivative that has shown benefits in patients with mild and moderate SOS by improving surface moisture and maintaining tear film integrity. Additionally, the properties of reconstitution and maintenance of the mucin layer have been recognized, depending on the concentration used. In addition, it can change its properties upon contact with the ocular surface, gelling, and increasing the maintenance time on the ocular surface to partially compensate for the lack of mucin in the tear film. 18
The presence of lipids in the tear film plays an important role in the control of surface tension and therefore in the wetting of the ocular surface. The tear evaporation rate is increased in patients with a deficiency of the lipid component; therefore, lipids have been incorporated into ocular lubricants in the form of liposomes (phospholipids in spherical vesicles) or nanoparticles. We also found them in the form of emulsions, which can be nonionic, anionic, or cationic, the latter being the ones that best interact with the mucinous layer (negative charge) giving greater stability to the tear film and increasing the BUT. The presence of glycerin 0.9% in CTP improves tear film stability in patients with evaporative or mixed DED and meibomian gland dysfunction. Trehalose is a molecule that protects the ocular surface from oxidative stress and prevents apoptosis of the corneal and conjunctival epithelial cells. In addition, its ability to reduce the concentration of inflammatory factors such as IL-6, IL-8, and TNF and the activation of corneal metalloproteinases (MMP-9) has been confirmed. 19 This unique ability of this molecule reduces the inflammatory component of the ocular surface in patients with DED.
This study has certain limitations such as its retrospective design (retrospective cohort, n = 67), the absence of a control group, and a short follow-up time (1 month) to evaluate the change in clinical parameters suggested by the authors. Due to the retrospective design, the risk of the presence of information bias is evident, especially memory bias, so we tried to control it by recording the results directly on the Cornea550 equipment (Essilor, Creteil, France) and reducing the measurement biases and intra- and interobserver variability compared to clinical measurements at the slit lamp evaluation. The absence of a control group does not allow us to compare our results with other molecules currently used in the treatment of DED in the short term (especially lubricants based on sodium hyaluronate and others with antievaporative components) currently recognized as the standard of care. However, reviewing the literature and previous publications, we could observe that a short follow-up time in dry eye studies is not infrequently used, although undoubtedly for future studies it would be interesting to follow-up patients longer than 1 month to confirm the therapeutic effect in the medium and long term. Finally, from the methodological point of view, we would like to highlight the achievement of the proposed study sample size according to the authors’ assumptions (SMD of 70% in OSDI results at 1 month with a 95% CI and loss rate of 20%).
In conclusion, we report for the first time, the clinical effectiveness of a new multipurpose-combined ocular lubricant (0.5% carboxymethylcellulose, 0.9% glycerin, and 3% trehalose, CTP) in subjects with DED diagnosed using a validated dry eye questionnaire (OSDI), lacrimal osmolarity and ocular surface parameters (NIBUT, meniscus height, and meibomian gland population) through a computerized anterior surface topographer (Cornea550, Essilor, Creteil, France) to decrease measurement bias and intra/interobserver variability.
Footnotes
Acknowledgment
All authors want to acknowledge Daniela Duran-Moreno, MD, for her work doing the translation from Spanish to English language of the final article.
Authors’ Contributions
P.-I.N.-N.: Concept and design, data collection, data analysis and interpretation, and drafting of the article. A.C.-A. and G.A.-R.: Data collection and interpretation. All the authors have read and agreed to the published version of the article.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Considerations
This study was evaluated and approved by the Ethics Committee in Human Beings Investigation, CEISH, Fundación Universitaria de Ciencias de la Salud, in accordance with the Helsinki Declaration. It was classified as a research study without risks and a retrospective design study with no intervention or modification of biological, physiological, psychological, or social variables from study participants.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
P.-I.N.-N., A.C.-A., and G.A.-R. received financial support from Mega-Labs Inc. Laboratories.