
Abstract
Purpose:
To evaluate the efficacy of human placental extract (HPE) eye drops compared to that of carboxymethylcellulose (CMC) and human peripheral blood serum (HPBS) eye drops in a mouse model of experimental dry eye (EDE) and corneal alkali burns.
Methods:
EDE and alkali burn models were induced in C57BL/6 mice using desiccating stress and NaOH, respectively. In both the EDE and alkali burn models, treatment groups received CMC, HPBS, or HPE eye drops. In EDE model, tear volume, tear break-up time (TBUT), and total corneal fluorescein staining score (CFSS) were measured. ROS were detected with 2’,7’-dichlorodihydrofluorescein diacetate. Conjunctiva goblet cells were identified by periodic acid-Schiff staining, and corneal epithelial apoptosis was detected by TUNEL assay. In alkali burn model, the area and diameter of epithelial defects were assessed in each group.
Results:
In the EDE model, tear volume, CFSS, and epithelial apoptosis were significantly improved in all treatment groups. Compared to the CMC group, the HPE group showed a better improvement in the production of tear volume, TBUT, CFSS, ROS, and conjunctiva goblet cell density. There were no significant differences in parameters between the HPBS and HPE groups except for TBUT at 14 days. In the alkali burn model, the HPE group had a smaller area compared to the control and CMC groups and a shorter diameter compared to the control group.
Conclusion:
HPE eye drops were as effective as HPBS eye drops in improving the clinical signs and ocular surface oxidative damage of EDE and in promoting corneal epithelialization after alkali burn.
Introduction
Ocular surface disease (OSD) affects the surface layers of the cornea and conjunctiva. 1 Dry eye is a prevalent OSD characterized by symptoms such as ocular discomfort and visual disturbance, tear film instability, ocular surface inflammation, and neurosensory abnormalities.2,3 Some studies have shown that increased tear film osmolality can trigger pro-inflammatory responses, leading to cell damages on the ocular surface.4,5 Common treatments for OSD include lubricants, anti-inflammatory drugs, and secretagogues, which are effective in relieving symptoms and improving the tear film and ocular surface system. 6
Biological tear substitutes such as autologous serum, platelet-rich plasma, and cord blood serum, are effective treatment options for severe OSD, such as dry eye associated with Sjögren’s syndrome, graft-versus-host disease, Stevens-Johnson syndrome, and alkali burns.7–12 These blood-derived eye drops are known to contain high concentrations of nutrients, vitamins, fibronectin, and growth factors, such as epithelial or nerve growth factors. 7 Several in vivo and in vitro studies have shown that the blood-derived eye drops can enhance corneal epithelial wound healing caused by diverse factors. 10
Human placental extract (HPE) is homologous in nature as it is derived from the human placental tissue. HPE has been approved in Japan and Korea for subcutaneous injection as a prescription drug for treating menopausal disorders and improving liver function. 13 In addition, HPE has potential applications in the fields of neurology, gynecology, and dermatology as it has anti-inflammatory, analgesic, antioxidant, cellular, and radio-protective properties.14,15 In addition, HPE increases the levels of transforming growth factor (TGF-β) and vascular endothelial growth factor, which affect the wound healing process. 16 Containing a diverse bioactive components like growth factors, cytokines, and regenerative molecules, HPE offers enhanced healing and anti-inflammatory effects compared to artificial tears, providing biologically relevant tissue repair mechanisms.17–19 Based on these properties, HPE may be effective in treating dry eye and promoting ocular surface wound healing. However, currently there is no research on the topical application of HPE for managing OSD.
In this study, we evaluated the effectiveness of applying HPE topically to treat OSD. We evaluated the effectiveness of topical HPE in treating dry eye by assessing tear film parameters, corneal fluorescein staining score (CFSS), ROS production, corneal epithelial apoptosis, and conjunctival goblet cell density, and further investigated its efficacy in promoting epithelial healing in a mouse model of corneal alkali burn, comparing these results to the application of carboxymethylcellulose (CMC) and human peripheral blood serum (HPBS).
Materials and Methods
Mouse models and experimental procedures
This study was approved by the Chonnam National University Medical School Research Institutional Animal Care and Use Committee (approval no. CNUHIACUC-22014). All animals were treated by the ARVO Statement for Use in Ophthalmology and Vision Animals Research. The study employed a sample of female C57BL/6 mice, aged 7–8 weeks, and all experiments were performed thrice.
For the experimental dry eye (EDE) model, the mice were exposed to 30% humidity and given subcutaneous injections of 0.5 mg/0.2 mL scopolamine hydrobromide (Sigma-Aldrich, St. Louis, MO) three times daily (9:00 am, 1:30 pm, and 6:00 pm). The mice were divided into 5 groups according to the topical eye drop treatment protocol: normal control, EDE, CMC, HPBS, and HPE groups.
We randomly selected one healthy donor per one experiment set for HPBS collection. We obtained informed consent from all healthy donors. A 60–80 ml blood sample was collected, stored at ambient temperature for 2 h, and then centrifuged at 3,000×g for 10 min at 4°C. Portioned, and stored in UV-protected 5 ml sterile tubes. HPBS and HPE were prepared on a sterile bench. HPE was extracted from sealed ampoules of Placein M Inj (Daehan New Pharm Co, Seoul, Korea). Both HPBS and HPE mixed with normal saline, sub-packaged in UV-protected 5 ml sterile tubes, and the tubes were stored in a refrigerator at 4°C. Both HPBS and HPE were prepared at a concentration of 50%, with each diluted 1:1 with normal saline. Refresh Plus® (Allergan, Westport, Ireland) was used as 0.5% CMC.
In the experimental dry eye model, both eyes of each mouse were treated with 2 μL of eye drops three times a day (9:30 am, 2:00 pm, and 6:30 pm). Tear volume, TBUT, and CFSS were quantified at 7 and 14 days. After 14 days, the production of ROS was assessed using a 2’,7’-dichlorodihydrofluorescein diacetate assay, corneal epithelial apoptosis was detected with a TUNEL assay, and the density of conjunctival goblet cell was determined by PAS staining.
In the alkali burn model, 2 μL of 0.5% proparacaine hydrochloride eye drops were applied to the right eye of the mice. A 2 mm piece of paper soaked in 2 μL of 0.1 M NaOH was placed on the cornea for 7–8 s, followed by rinsing with sterile saline and removal of the corneal epithelium. The mice were divided into four groups: control, CMC, HPBS, and HPE groups. Each group received eye drops three times daily (9:30 am, 2:00 pm, and 6:30 pm). The epithelial defect area and diameter were measured 3 and 5 days treatment. On day 5, the TGF-β levels were measured using ELISA.
Assessment of dry eye parameters
Dry eye parameters were measured more than 2 h after administering the eye drops.20,21 The tear volume was detected with a phenol red-soaked cotton thread (Zone-Quick; Oasis, Glendora, CA). The thread was positioned on both the middle and outer parts of the outer corner of the eye for 20 s, after which a microscopic examination was conducted (SMZ1500; Nikon, Melville, NY). Tear volume was determined by measuring the length of the red portion of the thread.
A 1% sodium fluorescein solution (1 μL) was instilled into the conjunctival sac. TBUT was determined with a slit lamp microscope (BQ-900; Haag-Streit Bern, Switzerland) under cobalt blue illumination. The corneal surface was examined for punctate staining 90 s after administration. The CFSS was scored by dividing the cornea into four quadrants and utilizing a 4-point scaling system for each quadrant, with a total score ranging from 0 to 16. 22
2’,7’-Dichlorodihydrofluorescein diacetate assay (DCFDA)
The generation of extracellular ROS was quantified using a CM-H2DCFDA kit (Invitrogen, Carlsbad, CA, USA) following the manufacturer’s guidelines. 23 The cornea and conjunctiva were excised, cut into small pieces, and incubated in phosphate-buffered saline with type D collagenase (0.5 mg/mL) at 37°C. ROS generation was confirmed and characterized using a FACSCalibur flow cytometer (BD Biosciences, San Jose, CA), employing excitation at 488 nm and emission at 530 nm, respectively. The results were evaluated compared to the normal control tissue, expressed as the average percentage increase in DCFDA fluorescence emission, were evaluated using CellQuest software (version 5.2.1; BD Biosciences).
Histological assessment
For PAS staining, the conjunctival tissues were fixed in paraformaldehyde (4%) overnight and embedded in paraffin. Serial sections (6 μm) were cut from each sample. The sections were subjected to a staining procedure utilizing 0.5% PAS to facilitate the identification of goblet cells. The cells were visualized with the aid of a microscope and digital camera. The number of goblet cells were quantified in three sections from each eye’s superior and inferior conjunctiva was quantified image analysis software (Media Cybernetics, Silver Spring, MD). The number of goblet cells is expressed as the mean count per 100 μm.
TUNEL staining
The eyes and surrounding tissues were excised and fixed overnight in paraformaldehyde (4%) at 4°C. They were then paraffin-embedded or cryosectioned for immunofluorescence staining. The DeadEnd™ Fluorometric TUNEL system (Promega, Madison, WI) was used by the manufacturer’s instructions, with DAPI staining and mounting in ProLong Gold Antifade Mounting Medium (Invitrogen, Carlsbad, CA). The tissues were analyzed using a confocal laser scanning microscope from Leica Microsystems (Heidelberg, Germany). TUNEL staining was visualized with 405 nm excitation and an emission wavelength of 424–472 nm, while DAPI staining was visualized with an excitation wavelength of 488 nm and an excitation wavelength of 502–550 nm. The results are expressed as the average count of TUNEL-positive cells.
Multiplex immunobead assay
A multiplex immunobead assay (Luminex 200) was used to measure corneal levels of TNF-α, IL-1β, and IL-6. Corneal tissues were collected from six eyes (three mice) per experiment for each group, incubated in lysis buffer with protease inhibitors, and centrifuged at 14,000 × g for 15 min. The supernatants were stored at −70°C, and protein concentrations were measured. Samples were pipetted into assay plates containing cytokine/chemokine beads and antibodies. After washing and incubation with a detection antibody, reactions were analyzed using xPONENT software. Cytokine concentrations were calculated based on standard curves from known recombinant cytokines.
Parameters of corneal epithelial defects
The images were acquired using a Nikon Millet stereoscopic microscope (SMZ® 1500). 24 Following staining with a solution containing 0.1% fluorescein, the area and largest diameter of corneal epithelial defects were quantified using Image-Pro Plus® software. 25 TGF-β protein levels in the cornea were quantified using a sandwich ELISA (Quantikine®; R&D Systems, Minneapolis, MN) method employing specific capture and detection antibodies. To ensure the accuracy of the ELISA, it was performed three times.
Statistical evaluation
The data were statistically analyzed using SPSS (version 18.0, Chicago, IL, USA). The results were expressed as mean ± standard deviation. The analysis employed a one-way ANOVA followed by Tukey’s post hoc test. All comparisons have been subjected to a statistical significance test with a P < 0.05.
Results
Clinical parameters of the tear film and ocular surface
The mean tear volumes were as follows: normal control 0.041 ± 0.005 μL, EDE 0.019 ± 0.005 μL, CMC 0.020 ± 0.003 μL, HPBS 0.019 ± 0.005 μL, and HPE 0.022 ± 0.004 μL initially. After 7 days, tear volume showed significant improvement in the HPE group compared to the EDE group (P = 0.03). There were no significant differences detected between the CMC and HPBS groups. On day 14, tear volumes were as follows: normal control 0.039 ± 0.005 μL, EDE 0.014 ± 0.004 μL, CMC 0.021 ± 0.004 μL, HPBS 0.023 ± 0.005 μL, and HPE 0.025 ± 0.004 μL. All treated groups demonstrated significantly enhanced tear volumes compared to the EDE group (all P < 0.01). In addition, the HPE group showed a significant improvement in tear volume compared to the CMC group (P = 0.01; Fig. 1A). However, no statistically significant differences were observed between the HPBS and HPE groups at 7 and 14 days.

The average tear volume
After 7 days of treatment, the TBUT values were as follows: normal control 1.78 ± 0.24 s, EDE 0.77 ± 0.22 s, CMC 0.85 ± 0.19 s, HPBS 0.89 ± 0.16 s, and HPE 0.85 ± 0.18 s. There were no statistically significant differences observed among the treatment groups on day 7. On day 14, the TBUT values were as follows: normal control 1.53 ± 0.18 s, EDE 0.65 ± 0.16 s, CMC 0.74 ± 0.20 s, HPBS 0.82 ± 0.20 s, and HPE 1.00 ± 0.21 s. Both the HPBS and HPE groups exhibited significantly higher BUT values compared to the EDE group (both P < 0.01). However, the HPE group demonstrated significantly higher TBUT values compared to both the CMC and HPBS groups (P < 0.01; Fig. 1B).
After 7 days of treatment, the CFSS values was as follows: normal control 3.89 ± 1.03, EDE 11.43 ± 1.47, CMC 10.34 ± 1.64, HPBS 9.16 ± 1.15, and HPE 8.95 ± 1.54. CFSS was notably decreased in all treatment groups compared to EDE (all P < 0.01), and both the HPBS and HPE groups exhibited significantly lower CFSS compared to the CMC group (both P < 0.01). On day 14, the CFSS values was as follows: normal control 5.43 ± 1.10, EDE 13.73 ± 1.47, CMC 9.55 ± 1.53, HPBS 7.93 ± 1.56, and HPE 7.91 ± 1.55. All treatment groups showed significantly lower CFSS compared to the EDE group (all P < 0.01). Additionally, CFSS scores were significantly lower in the HPBS and HPE groups compared to the CMC group (both P < 0.01; Fig. 1C). However, no statistically significant differences were observed CFSS between the HPBS and HPE groups at 7 and 14 days.
ROS levels in the cornea and conjunctiva
In representative images of corneal and conjunctival tissues Figure 2A. The DCFDA intensities was measured as follows: normal control 100 ± 0.0%, EDE 324.5 ± 40.1%, CMC 291.8 ± 27.4%, HPBS 201.8 ± 1.8%, and HPE 168.9 ± 20.4%. Compared to the EDE group, the intensity of DCFDA in the cornea was significantly lower in the HPBS and HPE groups (both P < 0.01). Additionally, compared to the CMC group, corneal DCFDA intensity was lower in the HPBS group (P = 0.01), and significantly lower in the HPE group (P < 0.01; Fig. 2B). Similarly, in the conjunctival tissue, the DCFDA intensities was as follows: normal control 100 ± 0.0%, EDE 315.0 ± 50.7%, CMC 276.1 ± 47.4%, HPBS 184.3 ± 3.8%, and HPE 158.3 ± 7.6%. The HPBS group showed slightly lower DCFDA intensity compared to the EDE group (P = 0.02). The HPE group exhibited a significantly lower intensity compared to the EDE group (P < 0.01; Fig. 2C). Compared to the CMC group, the HPE group also showed a slight decrease (P = 0.01). However, no statistically significant differences were observed in DCFDA intensity between the HPBS and HPE groups.
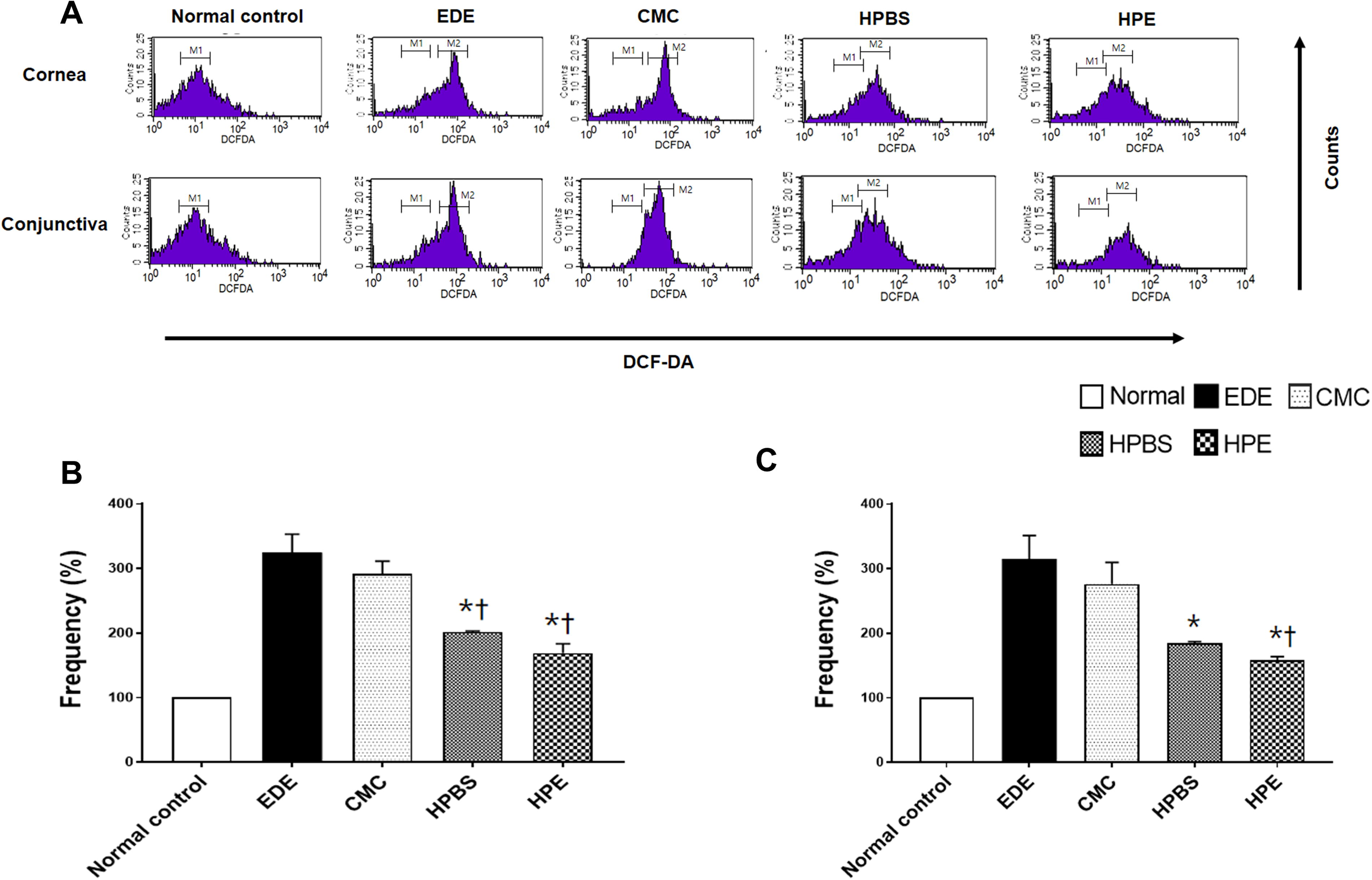
The representative image
Density of goblet cells in the conjunctiva
Representative histological images of conjunctival goblet cells are shown in Figure 3A. The mean goblet cell densities were as follows: normal control 37.33 ± 3.10 cells/100 µm, EDE 8.33 ± 1.25 cells/100 µm, CMC 12.33 ± 0.47 cells/100 µm, HPBS 19.33 ± 3.40 cells/100 µm, and HPE 25.67 ± 2.50 cells/100 µm. Compared to the EDE group, goblet cell density was significantly higher in the HPBS and HPE groups (both P < 0.01). Additionally, the HPE group exhibited a higher density of goblet cells compared to the CMC group (P < 0.01; Fig. 3B). However, no statistically significant differences in goblet cell density were observed between the HPBS and HPE groups.
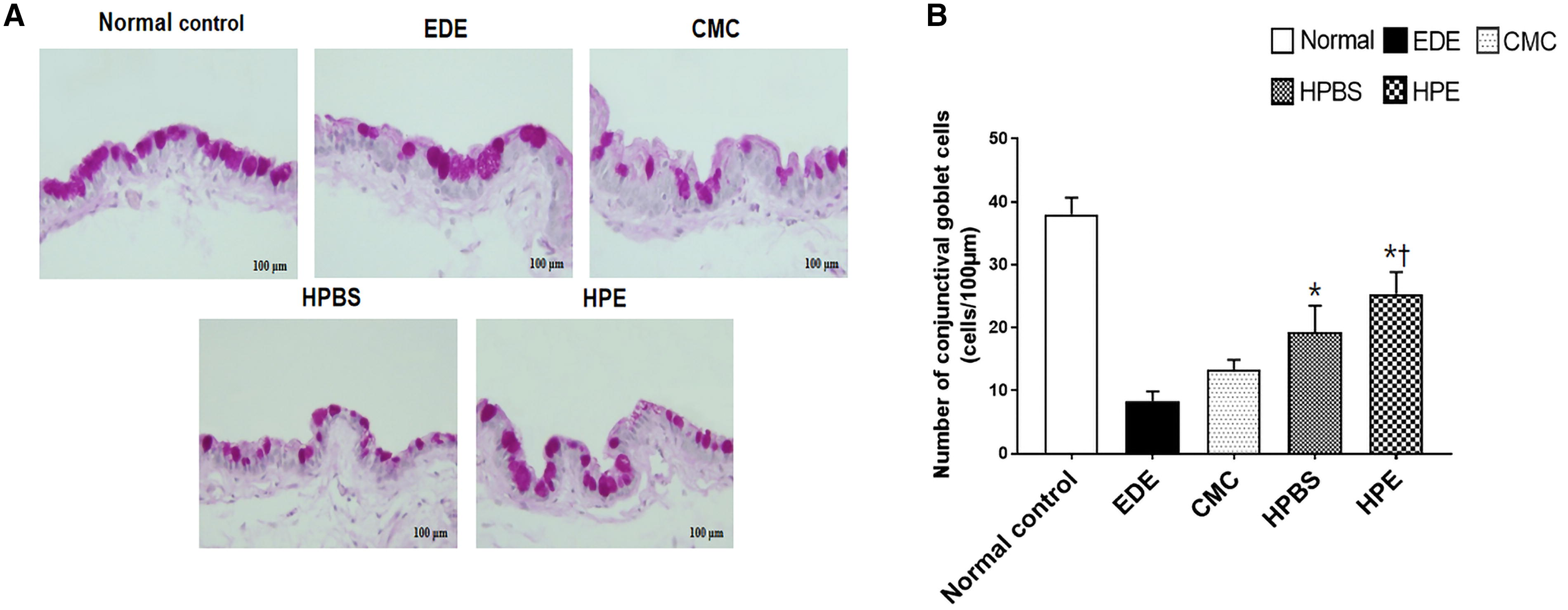
The representative images of PAS staining
Corneal epithelial apoptosis
Magnified images of typical corneal sections stained with TUNEL (green) and DAPI (blue) are shown in Figure 4A. The mean number of epithelial apoptotic cells were as follows: normal control 1.25 ± 0.83 cells/100 µm, EDE 12.00 ± 3.24 cells/100 µm, CMC 6.00 ± 0.71 cells/100 µm, HPBS 3.75 ± 0.83 cells/100 µm, and HPE 2.75 ± 0.43 cells/100 µm. Compared to the EDE group, apoptotic cell numbers were significantly observed in the CMC, HPBS, and HPE groups (all P < 0.01; Fig. 4B).
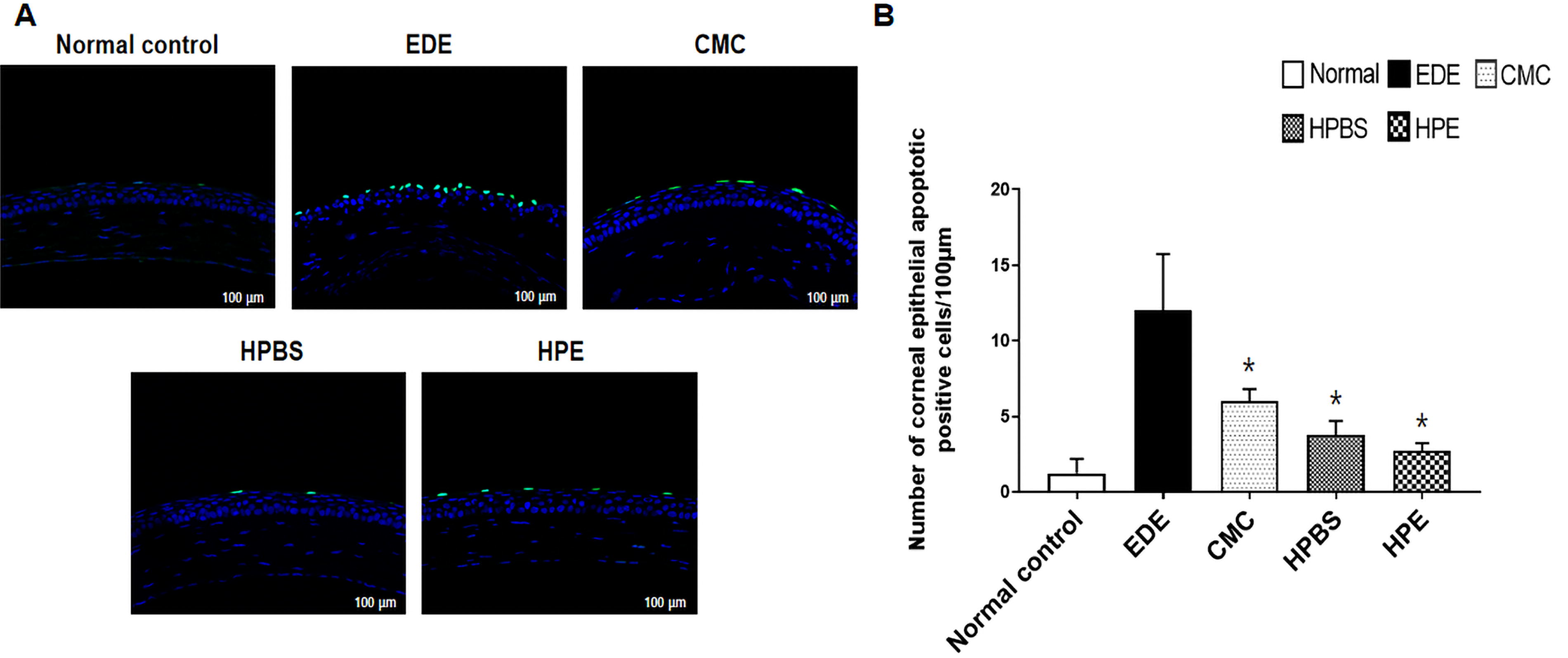
The representative images of TUNEL staining
Inflammatory cytokine level in corneal tissues
The corneal levels of TNF-α were 0.30 ± 0.05 pg/mL in the normal control, 4.48 ± 0.14 pg/mL in EDE, 2.70 ± 0.18 pg/mL in both the CMC and HPE groups, with HPBS at 3.14 ± 0.17 pg/mL. For IL-1β, the levels were 9.17 ± 1.16 pg/mL in the control, 14.54 ± 3.25 pg/mL in EDE, and reduced to 7.43 ± 2.44 pg/mL in HPBS and 9.17 ± 3.04 pg/mL in HPE. Similarly, IL-6 levels were 25.69 ± 5.05 pg/mL in the control, 32.56 ± 7.04 pg/mL in EDE, 17.50 ± 5.56 pg/mL in HPBS and 17.13 ± 4.84 pg/mL in HPE. Although the levels of TNF-α, IL-1β, and IL-6 were lower in all treatment groups compared to EDE, there were no significant differences between the treatment groups.
Parameters of corneal epithelial defects in alkali burn model
Three days after treatment, the defect areas were as follows: control 2.77 ± 0.94 mm2, CMC 2.54 ± 0.75 mm2, HPBS 2.00 ± 1.19 mm2, and HPE 1.93 ± 0.90 mm2. The HPE group showed a slightly smaller defect area compared to the control group (P = 0.03). Five days after treatment, the defect areas was as follows: control 1.07 ± 0.95 mm2, CMC 0.67 ± 0.74 mm2, HPBS 0.48 ± 0.33 mm2, and HPE 0.37 ± 0.55 mm2. After 5 days of the treatment, the area was reduced in the HPBS (P = 0.04) and HPE (P < 0.01) groups compared to the control group. Additionally, the area of the HPE group was smaller than that of the CMC group at 5 days (P = 0.04; Fig. 5A).
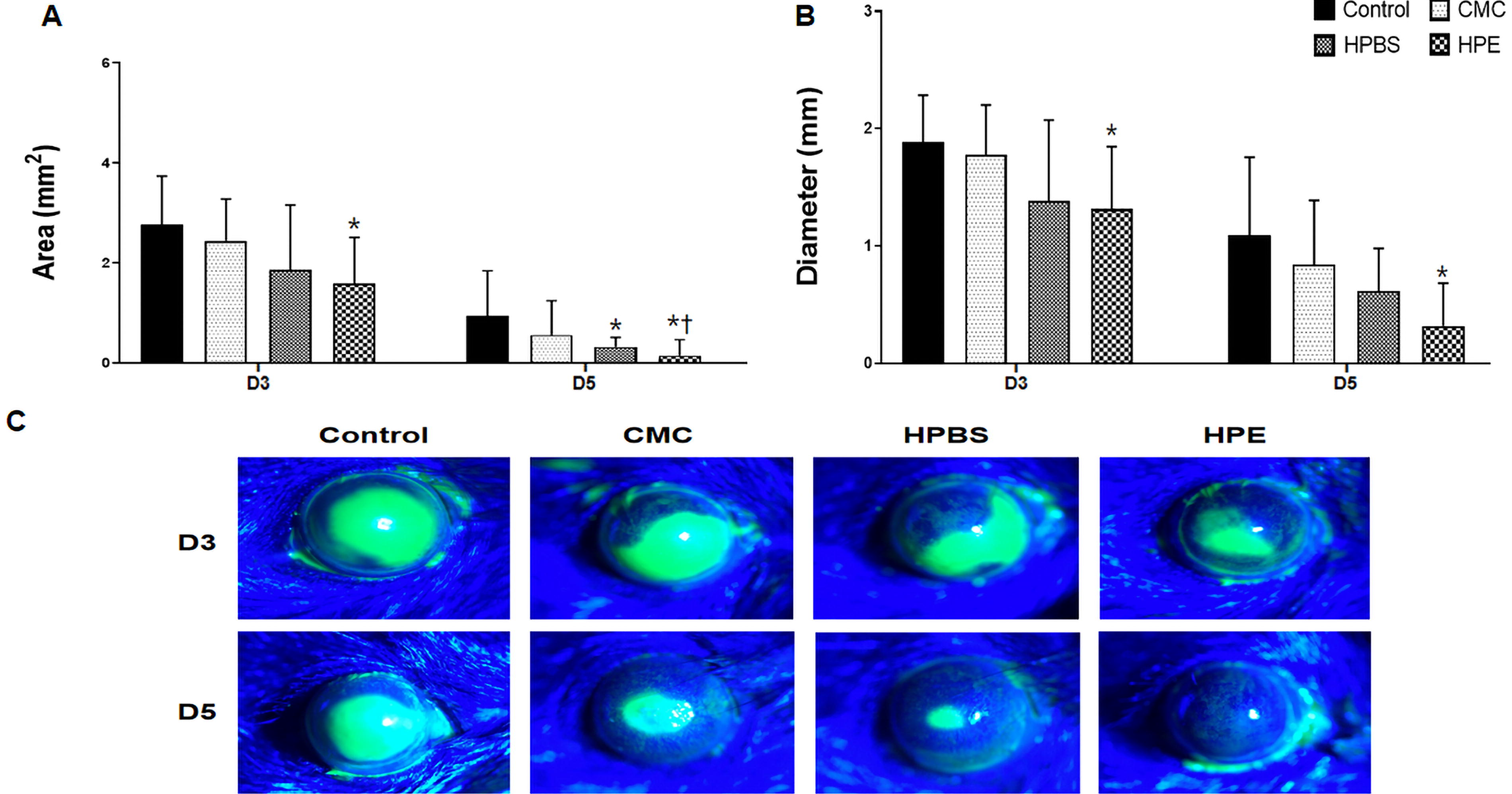
The changes in the area
Three days after the same treatment, the defect diameters were as follows: control 1.89 ± 0.39 mm, CMC 1.77 ± 0.41 mm, HPBS 1.64 ± 0.46 mm, and HPE 1.38 ± 0.54 mm. The defect diameter in the control group was slightly larger than that in the HPE group (P = 0.02). Five days after the same treatment, the defect diameters were as follows: control 1.02 ± 0.60 mm, CMC 0.79 ± 0.49 mm, HPBS 0.68 ± 0.28 mm, and HPE 0.51 ± 0.52 mm. The diameter was shorter in the HPE group compared to the control group (P < 0.01; Fig. 5B). However, no statistically significant differences in diameter were observed between the treatment groups.
The concentration of TGF-β was 416.8 ± 115.3 pg/mL in the control group, 500.6 ± 70.4 pg/mL in the CMC group, 508.0 ± 92.1 pg/mL in the HPBS group, and 448.5 ± 75.1 pg/mL in the HPE group. The levels of TGF-β were improved in all experimental groups, with no significant differences observed between the experimental groups.
Discussion
Blood-derived eye drops such as autologous serum, platelet-rich plasma, and allogeneic PBS, provide a benefit over traditional treatments, in that they provide both lubrication to the ocular surface and contain biochemical components, such as nutrients and growth factors.25–27 The impact of blood-derived products on cell proliferation, vitality, and the influence of blood-derived products on the growth and movement of corneal epithelial cells have been extensively studied both in laboratory cultures and in living organisms. 10 These eye drops have been employed in the treatment of diverse OSDs such as dry eye, persistent corneal epithelial defects, recurrent corneal erosion, and limbal stem cell deficiency.28,29
However, blood-derived eye drops sometimes have limitations due to several factors. The production of blood products is regulated by national laws or legal requirements for disease transmission through blood. 27 Issues of production optimization, storage (−20°C), and contamination issues have not been fully resolved.30,31 Concerns remain regarding the use of autologous sources in patients with active systemic inflammation and chronic anemia. Therefore, new concepts for eye drops using standardized and approved human derivatives may be effective. 32
HPE is homologous in nature and is derived from the healthy maternal placenta. The placenta contains a storehouse of cytokines, hormones, bioactive peptides, enzymes, growth factors, vitamins, and minerals. 15 Placental extracts are created by purifying the placenta through a process involving dialysis, heat, and hydrolysis. Therefore, they contain various biologically active substances, such as aminopeptidase, minerals, and growth factors. Low molecular weight reduces the risk of allergic reactions. 15 Several studies support the low immunogenicity of processed HPE for medical applications including wound healing and tissue regeneration. 16 Additionally, the immune-privileged properties of the ocular surface mitigate the risk of immune reactions and enable safe application. 16
Several studies have shown that HPE have potential applications in neurology, gynecology, and dermatology. 13 HPE components have anti-inflammatory, analgesic, antioxidant, cellular, and radio-protective properties.14,33–35 In addition, HPE increases the levels of TGF-β, fibroblast growth factors, and vascular endothelial growth factors, which influences the wound healing process. 36 Another in vitro study showed that HPE could suppress the production of lipopolysaccharide-induced inflammatory cytokines, such as IL-6 or IL-8. 37 Tablets containing HPE can effectively promote the migration of keratinocytes and epithelial cells and the formation of new blood vessels, thereby improving the quality of wound healing.17,19 The other study showed that HPE had anti-inflammatory effects, fibroblast growth factor-2 activation, and collagen deposition facilitated the healing process of skin wounds in both normal and diabetic mice. 19 This agent may help to repair the damaged corneal epithelial cells, reduce inflammation, and increase the number of conjunctival epithelial cells.16,37 Therefore, these actions may be effective in the recovery of dry eye and corneal injury caused by burns.
While both HPBS and HPE contain regenerative factors crucial for ocular surface healing, HPBS faces challenges in terms of production, consistency, and patient-specific efficacy. HPE, on the other hand, offers a more standardized approach, being mass-produced with relatively consistent concentrations of growth factors and cytokines. 38 This ensures that HPE can be applied to a wider range of patients, including those with poor general health or systemic inflammation, who autologous PBS may not be as effective. 39 This study investigated to demonstrate that HPE could serve as a reliable treatment option for ocular surface diseases.
In this study, we confirmed the efficacy of topical HPE eye drops compared to those of CMC and HPBS eye drops in a mouse model with EDE and alkali burns. All treatment groups demonstrated significant enhancements in the tear volume, TBUT, CFSS, and conjunctiva goblet cell density. The HPBS and HPE groups showed reduced ROS production, increased conjunctival epithelial cell density, and reduced corneal epithelial apoptosis compared to the EDE group. Previous research proposed that placenta extracts induced the expression of antioxidant enzyme genes and protected the cells from H2O2-induced cell death in vitro experiments. 40 They showed that placental extract treatment increased the expression of superoxide dismutase-1 and 3 and catalase. Our study also showed decreased ROS production as measured by DCFDA and corneal apoptosis as analyzed by the TUNEL assay in the EDE mouse model.
In the mouse model of alkali burns, all treatment groups showed significant improvements in the area and diameter of corneal epithelial defects. There were no significant differences in TGF-β levels between any of the experimental groups. TGF-β is an important component of wound healing. TGF-β plays a role in controlling the migration and proliferation of corneal cells during wound healing. However, elevated levels of TGF-β have been demonstrated to induce tissue fibrosis. In several studies, post-treatment TGF-β levels were often lower in the treatment group; but in this study, there was no difference between groups.41,42 This may be due to the nature of biological eye drops containing high levels of growth factors. 38
While our analysis indicated a trend of decreased cytokine levels in the treatment groups compared to the EDE control, the differences were not statistically significant. This may be attributed to the limited sample size, potentially affecting the statistical power. However, the observed trend suggests that HPE may have a reducing effect on pro-inflammatory cytokines like IL-6, supporting its potential anti-inflammatory role. Future studies with larger sample sizes will be necessary to confirm these preliminary findings and further elucidate HPE’s mechanism of action in ocular surface healing.
This study had several limitations. Although human serum was used for comparison with HPE, the xenogenic nature of human serum in a mouse model could have introduced variability, which should be considered when interpreting the results. CMC was used as a control group in the alkali burn model, its limited efficacy in treating severe ocular injuries may affect the generalizability of our results. Additionally, due to the restricted availability of corneal samples, we were unable to perform analyses on cell proliferation and migration. While our current results highlight therapeutic potential of HPE, future studies with larger sample sizes and detailed molecular investigations will be essential to fully elucidate these mechanisms and validate our findings in alkali burn model. Furthermore, despite strict regulatory controls and intravenous use in Japan and Korea with few safety concerns, the risk of unexpected infectious transmission cannot be fully eliminated. Further safety studies and clinical trials are essential before applying HPE in ocular therapies. In addition, future research should include quantitative biochemical analyses to compare active ingredients and further explore their therapeutic relevance.
Conclusion
In conclusion, HPE eye drops were as effective as HPBS eye drops in improving the clinical signs and oxidative damage in the ocular surface of EDE. HPE also promoted epithelialization and wound healing on the ocular surface after alkali burns. These results demonstrated that topical treatment using HPE had a therapeutic efficacy equivalent to that of the biological tear substitute using HPBS eye drops in dry eye and ocular alkali burns.
Footnotes
Authors’ Contributions
K.C.Y. designed the experiment and revised the article. H.J., E.Y.J., J.T.L., H.S.Y., and J.Y.M. performed the experiments. H.J., E.Y.J., J.T.L., H.S.Y., and J.S.C. analyzed and interpretedthe data. H.J. and H.J.Y. drafted the article. All authors read and approved the final article and agree to be accountable for all aspects of the research in ensuring that the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Supported by the Chonnam National University Hospital Biomedical Research Institute (BCRI23039 and BCRI24084), Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2022R1F1A1075034), and a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2020-KH088567).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.