
Abstract
Purpose:
Cyclosporine A (CsA) is a primary treatment for dry eye disease (DED). Ophthalmic solutions containing CsA are available in concentrations of 0.05%, 0.09%, and 0.1%. While 0.1% CsA solutions have been used to treat DED, their safety and effectiveness remains somewhat uncertain. Therefore, we conducted a meta-analysis to evaluate their safety and efficacy.
Methods:
We searched PubMed, Cochrane Database, Embase, and Web of Science for randomized controlled trials (RCTs) that compared 0.1% CsA solutions with their vehicle. Statistical analysis was performed using Review Manager 5.4.1.
Results:
We included six RCTs (2,170 patients) with follow-up periods ranging from 4 weeks to 6 months. A total of 1,119 patients (51.56%) with DED were treated with 0.1% CsA. The mean age of patients was 57.9 ± 4.8 years, with 79.7% being female. The total corneal fluorescein staining (tCFS) at last follow-up [mean differences (MD) −0.49; 95% confidence interval (CI) (−0.73, −0.24); P < 0.0001], at 4 weeks [MD −0.64; 95% CI (−1.07, −0.22); P = 0.003], and central corneal fluorescein staining (cCFS) [MD −0.19; 95% CI (−0.35, −0.03); P = 0.02] scores were lower in patients treated with 0.1% CsA compared with vehicle. The Lissamine Green conjunctival staining (LGCS) [MD −0.51; 95% CI (−0.78, −0.24); P = 0.0002] and ocular surface disease index (OSDI) scores [MD −3.04; 95% CI (−5.84, −0.23); P = 0.03] were lower in the 0.1% CsA group compared with vehicle. Adverse events associated with 0.1% CsA solution in the treatment of DED varied across studies, but were generally mild to moderate. Notably, similar events were also significantly present in the vehicle group, supporting the safety profile of this treatment.
Conclusion:
Ophthalmic 0.1% CsA seems safe for treating DED, and significantly reduced tCFS, cCFS, LGCS, and OSDI scores compared with vehicle solutions.
Introduction
Dry eye disease (DED) is one of the most common ocular disorders globally, with an estimated prevalence of around 8% in the United States. 1 DED is a multifactorial condition characterized by tear film composition and volume changes, leading to ocular surface disturbance.2,3 Its subtypes are aqueous-deficient, marked by diminished lacrimal gland secretion, evaporative, caused by an abnormal tear film lipid layer, or a combination of both.1,4,5 Various risk factors have been linked to DED, including increasing age, female sex, Meibomian gland dysfunction, contact lens use, corneal refractive surgery, antihistamines, antidepressants and anxiolytics, low humidity environments, prolonged exposure to air-conditioned rooms and screens, autoimmune diseases such as Sjogren’s Syndrome (SS). 6 Common symptoms are eye discomfort, pain, burning sensation, and blurred vision, which are usually associated with inflammation. 2 This disorder negatively impacts patients’ lives by decreasing overall quality of life, reducing work productivity, and increasing expenditures on ophthalmic medications.7–9
The pathophysiology of DED involves a vicious cycle of tear film instability and hyperosmolarity, apoptosis of conjunctival and corneal cells, and ocular surface inflammation, which perpetuates tear film instability.10,11 Experimental research has revealed a complex interaction between mitogen-activated protein kinases, proinflammatory cytokines such as IL-1, TNF-α and IL-6, chemokines, and matrix metalloproteinases including MMP-3 and MMP-9, and a T-cell immune response in the pathogenesis of DED. 12
Current initial management typically involves artificial tears, eyelid hygiene, and environmental modifications. 13 If symptoms persist, eye drops such as short-term corticosteroids and CsA may be prescribed to minimize the inflammatory process.14,15 Cyclosporine, a T-cell immunomodulatory agent, has shown itself very effective in patients with inflammatory symptoms, decreasing the expression of proinflammatory cytokines and other mediators of immune response. 16 Multiple dosages of CsA are available for commercialization combined with different vehicle types such as glycerin and castor oil emulsion (0.05% Restasis®), nanomicellar aqueous solution (0.09% Cequa®), water-free semifluorinated alkane (SFA) solution (0.1% Vevye® in the United States and 0.1% Vevizye in Europe), and cationic emulsion (0.1% Ikervis®).
This meta-analysis was designed and conducted to evaluate randomized controlled trials (RCTs) comparing the safety and effectiveness of 0.1% CsA eye drops to vehicles. We explored populations with DED, and studies with up to 24 weeks follow-up time. This is particularly relevant as many of the articles analyzed here were not available at the time previous studies were published, in which they analyzed the effects of other concentrations of CsA.12,17 This approach enhances the precision of outcomes to better guide clinical practice.
Methods
Our study was performed and reported according to the guidelines of the Cochrane Collaboration Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement. 18 The protocol was prospectively registered in the International Prospective of Systematic Reviews (PROSPERO) under protocol number CRD42024571344.
Data source and search strategy
We systematically searched PubMed, Embase, Cochrane, and Web of Science databases. Our search was last updated in May 2024. The detailed search was: [“dry eye” OR “Dry Eye Syndromes” (Mesh) OR keratoconjunctivitis] AND (“CyclASol” OR “Vevye” OR “Restasis” OR “Ikervis” OR “Tj Cyporin” OR “Clacier” OR “CEQUA” OR “Zirun” OR “CsA” OR “cyclosporine” OR “ophthalmic solution” OR “ophthalmic emulsion” OR “nanomicellar” OR “nanomicel*”) AND “vehicle”. Two authors, Y.I. and D.A., independently assessed all records, and a decision regarding full-text retrieval was arbitrated by consensus between them. Full texts were retrieved by Y.I. and D.A., and inclusion and exclusion criteria were discussed. References of eligible articles and systematic reviews were also searched for additional studies of interest. Conference abstracts and prospective trials were also searched.
Eligibility criteria
There was no restriction regarding the publication date. We considered studies eligible for inclusion if they (1) were randomized clinical trials (RCT), (2) directly compared 0.1% CsA with vehicle, and (3) included patients with DED. The exclusion criteria were as follows: (1) animal studies and (2) case reports, abstracts, editorials, letters, and conference proceedings without sufficient data.
Endpoints and subanalyses
Our clinical outcomes of interest were: (1) total corneal fluorescein staining (tCFS) at last follow-up, (2) tCFS at 4 weeks, (3) water-free (SFA-based) solution tCFS, (4) central corneal fluorescein staining (cCFS), (5) dryness score, (6) blurred vision score, (7) Lissamine Green conjunctival staining (LGCS), (8) ocular surface disease index (OSDI) score, and (9) safety regarding adverse events (AEs). The articles included in this study used the National Eye Institute (NEI) and modified-Oxford grading scales to assess total and central fluorescein staining scores, and the visual analog scale (VAS) to evaluate dryness and blurred vision scores.
Leave-one-out analysis
Subgroup analysis was conducted based on the type of CsA solution: water-free (SFA-based) or cationic emulsion to identify if heterogeneity of results would arise from different design settings. Moreover, a leave-one-out sensitivity analysis (Table 1) was conducted to determine each study’s effect on the estimated pooled analysis by excluding each study step-by-step.
Leave-One-Out Analysis
cCFS, central corneal fluorescein staining; LGCS, Lissamine Green conjunctival staining; OSDI, ocular surface disease index; tCFS, total corneal fluorescein staining.
Quality assessment
Two independent authors (Y.I. and D.A.) assessed the risk of bias in the included RCTs using the Cochrane tool for assessing the risk of bias in RCTs (RoB-2). 19 Disagreements were resolved through consensus.
Statistical analysis
We applied the Mantel-Haenszel random-effects model with a restricted maximum likelihood variance estimator for all outcomes. We pooled mean differences (MD) with 95% confidence interval (CI) for continuous endpoints, collecting the MD from follow-up to baseline in each group, when available. P-values less than 0.05 were deemed significant for treatment effects. As needed, we extracted data from graphs using the WebPlotDigitizer tool. We assessed heterogeneity with Cochrane’s Q and I2 statistics, with P ≤ 0.10 indicating statistical significance for heterogeneity. A random-effects model was used for all analyses. Review Manager 5.4.1 (Cochrane Centre, The Cochrane Collaboration, Denmark) was used for statistical analysis.
Results
Study selection and baseline characteristics
As detailed in Figure 1, a total of 687 studies were identified: 114 from PubMed, 199 from Embase, 222 from Cochrane, and 152 from Web of Science. After removing 368 duplicate studies, 319 unique studies remained. Of these, 308 were excluded based on our exclusion criteria, leaving 11 articles for further assessment and full review. Subsequently, five additional articles were excluded. Finally, six studies were included in this review, all of which were RCTs. A total of 1,119 patients received the intervention (0.1% CsA), while 1,051 received the vehicle solution. The characteristics of these studies are reported in Table 2.
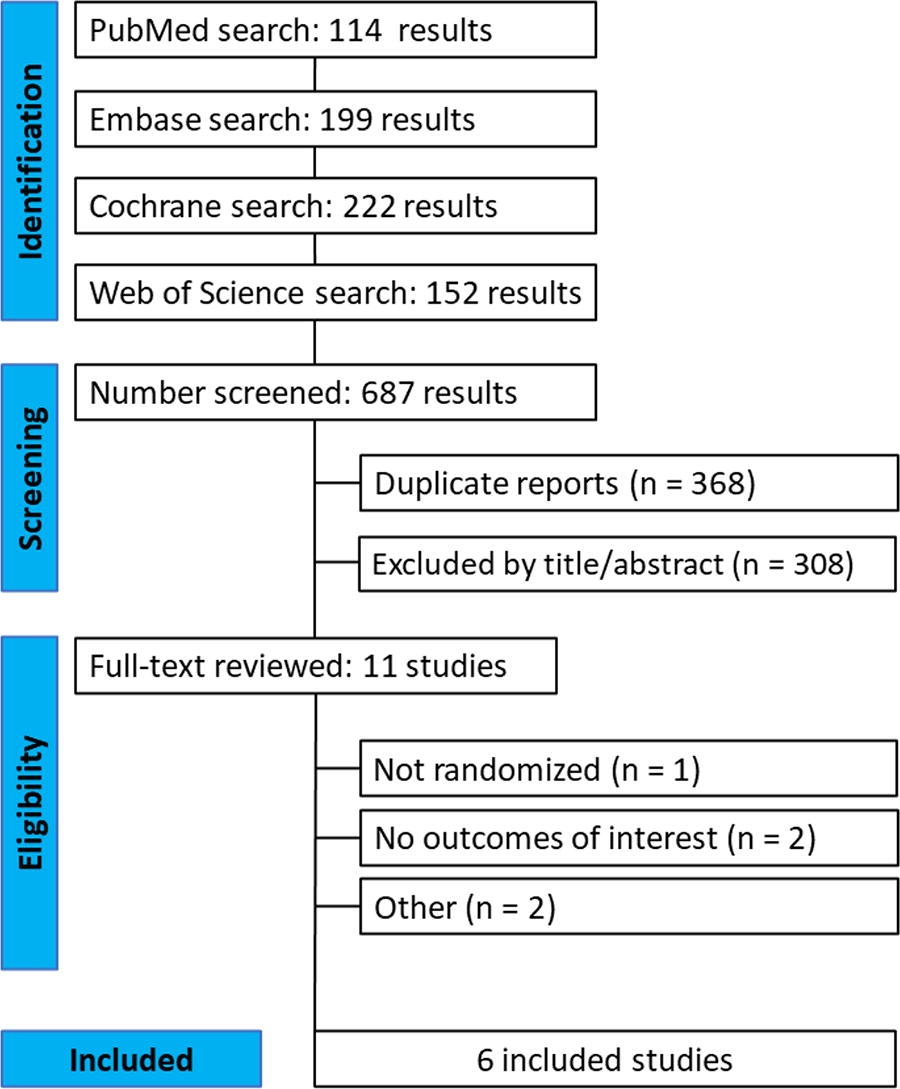
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram of study screening and selection.
Baseline Characteristics of Included Studies
C, control; cCFS, central corneal fluorescein staining; CsA, cyclosporine; DED, dry eye disease; I, intervention; LGCS, Lissamine Green conjunctival staining; NEI, National Eye Institute; OSDI, ocular surface disease index; RCT, randomized controlled trial; SS, Sjogren’s Syndrome; ST, Schirmer test; tCFS, total corneal fluorescein staining; VAS, visual analog scale.
Pooled analysis
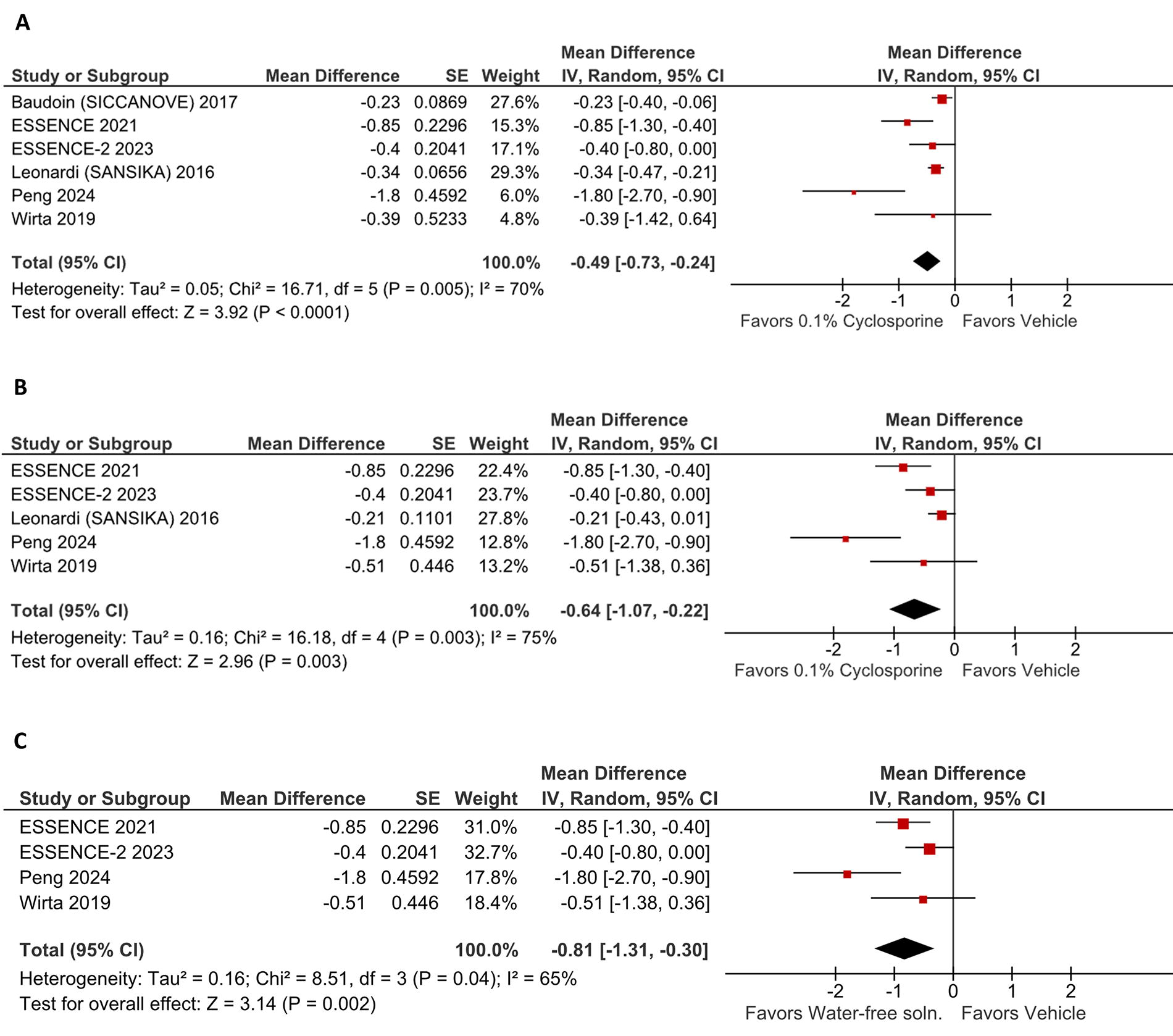
All articles included reported the tCFS score at last follow-up. The studies utilized 0.1% CsA water-free solution and cationic emulsion as interventions and demonstrated a significant difference between the 0.1% CsA and vehicle groups [MD −0.49; 95% CI (−0.73, −0.24); P < 0.0001; I2 = 70%; Fig. 2A]. The results indicated that the use of 0.1% CsA improved tCFS more than the vehicle.
Five studies reported tCFS at 4 weeks, using 0.1% CsA water-free solution and cationic emulsion as interventions. The results demonstrated a significant difference between 0.1% CsA and the vehicle [MD −0.64; 95% CI (−1.07, −0.22); P = 0.003; I2 = 75%; Fig. 2B]. This indicates that 0.1% CsA improves tCFS more effectively than the vehicle as early as 4 weeks.
We conducted a subgroup analysis of the 0.1% CsA water-free (SFA-based) solution for the outcome of tCFS at 4 weeks, including four studies. The pooled results showed a significant difference between the 0.1% CsA water-free (SFA-based) solution and its vehicle (F4H5) [MD −0.70; 95% CI (−0.97, −0.43); p < 0.00001; I2 = 65%; Fig. 2C]. These findings indicate that the 0.1% CsA water-free (SFA-based) solution is superior to its vehicle in improving tCFS at 4 weeks.
Three studies reported cCFS at 4 weeks. They all used 0.1% CsA water-free solution as an intervention. These studies showed a significant difference between 0.1% CsA water-free solution and its vehicle [MD −0.19; 95% CI (−0.35, −0.03); P = 0.02; I2 = 46%; Fig. 3]. The results indicated that 0.1% CsA water-free solution improves cCFS better than its vehicle for this outcome.
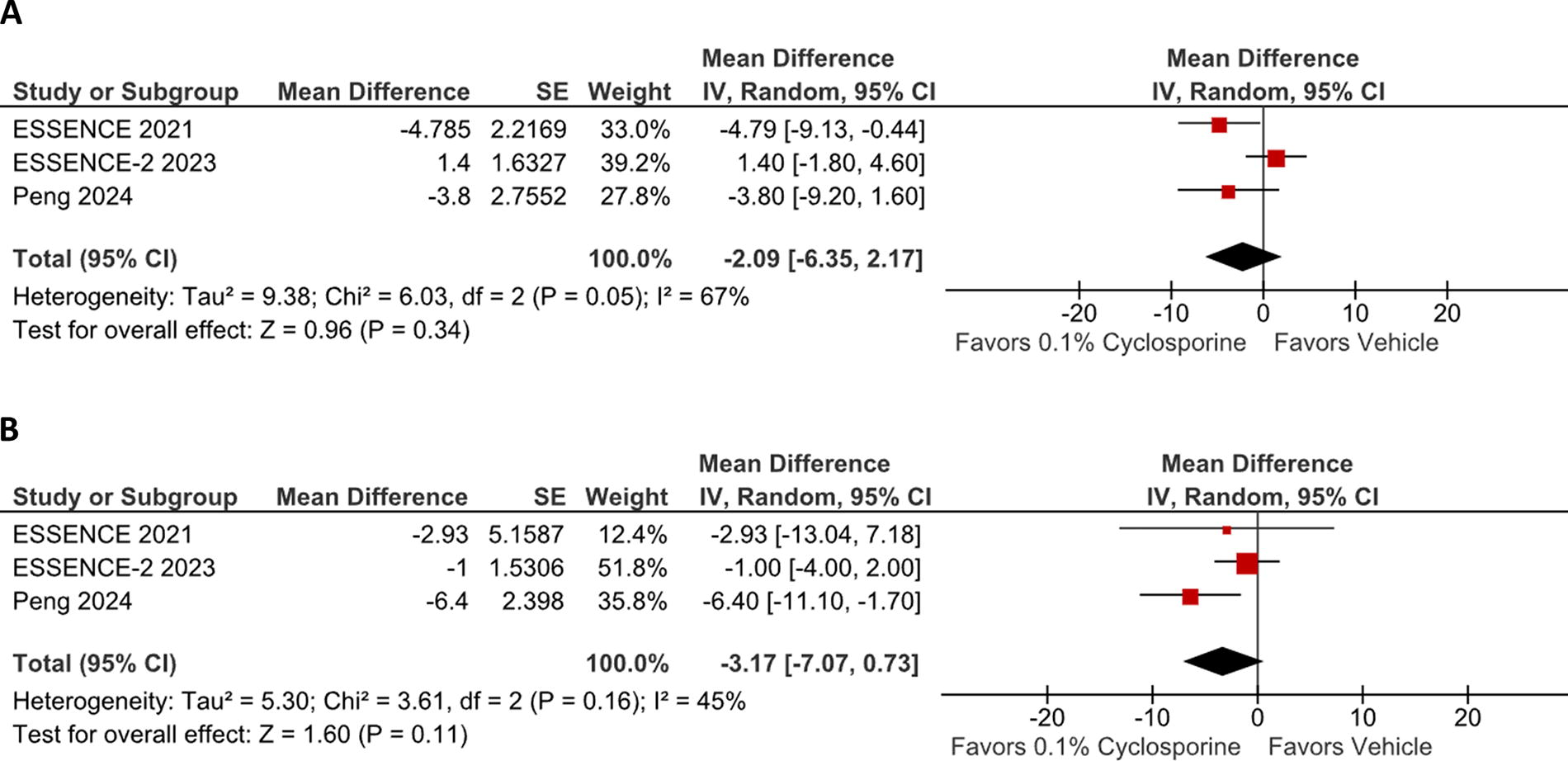
Three studies reported dryness scores, all using 0.1% CsA water-free solution as the intervention. The results revealed no significant difference between 0.1% CsA water-free solution and its vehicle [MD −2.09; 95% CI (−6.35, 2.17); P = 0.34; I2 = 67%; Fig. 4A].
Three studies reported blurred vision scores. They all used 0.1% CsA water-free solution as the intervention. These studies revealed no significant difference between 0.1% CsA water-free solution and its vehicle [MD −3.17; 95% CI (−7.07, 0.73); P = 0.11; I2 = 45%; Fig. 4B].
Three studies reported LGCS scores, all using 0.1% CsA water-free solution as the intervention. The results revealed a significant difference between 0.1% CsA water-free solution and its vehicle [MD −0.51; 95% CI (−0.78, −0.24); P = 0.0002; I2 = 26%; Fig. 5A]. The results indicated that 0.1% CsA water-free solution improves LGCS scores compared with its vehicle.
Three studies reported OSDI scores using 0.1% CsA water-free solution and cationic emulsion as interventions. The results revealed a significant difference between 0.1% CsA and vehicle groups [MD −3.04; 95% CI (−5.84, −0.23); P = 0.03; I2 = 0%; Fig. 5B]. The results indicated that 0.1% CsA improves overall OSDI scores more effectively compared with vehicles.
Leave-one-out sensitivity analysis
We performed the leave-one-out analysis for all outcomes. No significant results were found when each study was removed from its respective outcome.
Quality assessment
Figure 6 represents the risk of bias assessment for each study. Only two studies showed some concerns about RoB-2 due to missing outcome data. Those studies used 0.1% CsA cationic emulsion as an intervention. Other than that, all studies showed low overall risk of bias.

cCFS was significantly lower in the 0.1% cyclosporine group. cCFS, central corneal fluorescein staining.

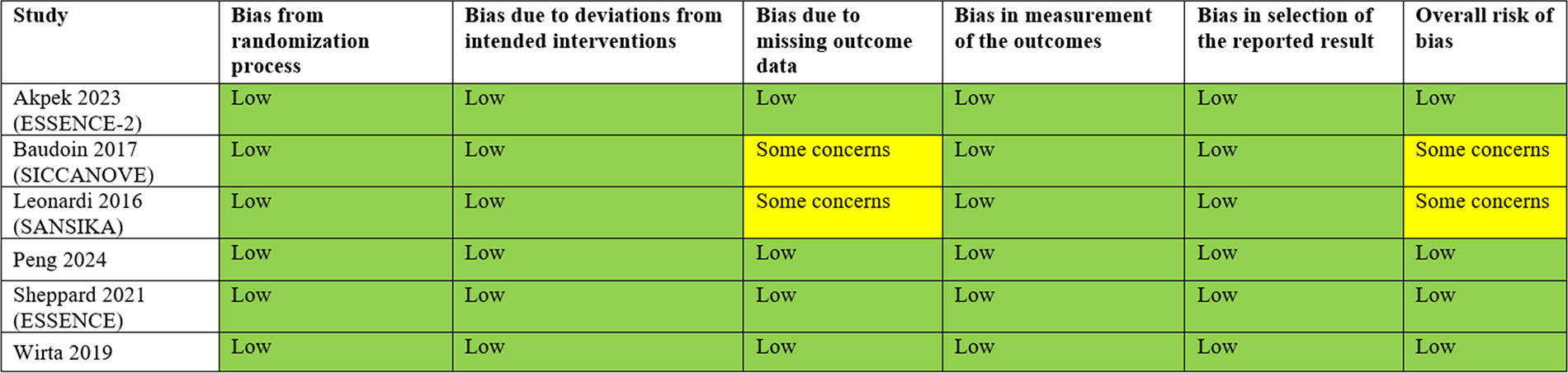
Risk of bias summary for randomized studies (RoB-2).
Safety and tolerance
AEs associated with CsA solutions in the treatment of dry eye syndrome varied across studies, but were generally mild to moderate in severity, supporting the safety profile of this treatment.
In the ESSENCE-2 trial (Akpek et al., 2023), treatment-emergent serious adverse events (TE-SAEs) were infrequent, with two cases (0.5% of patients) reported in the CsA group and three (0.7%) in the vehicle group. Visual acuity reduction was observed in 7 (1.7%) patients in the CsA group compared with 13 (3.2%) in the vehicle group, while mild to moderate instillation site reactions were slightly more common in the CsA group [43 (10.2%) vs. 36 (8.8%)]. No severe instillation site reactions were reported in either group. Discontinuation due to AEs occurred in two (0.5%) participants treated with CsA and three (0.7%) in the vehicle group.
Similarly, Baudoin et al. (2017) reported ocular treatment-emergent AEs in both the CsA and vehicle groups, but with a higher incidence in the CsA group [103 (42.6%) vs. 67 (26.8%)]. The most common AEs included eye irritation [39 (16.1%) vs. 6 (2.4%)], instillation site irritation [22 (9.1%) vs. 4 (1.6%)], and eye pain [17 (7%) vs. 7 (2.8%)]. Severe ocular AEs were more prevalent in the CsA group (87 (36%) vs. 28 (11.2%)], and discontinuation due to AEs occurred in 24 (9.9%) patients receiving CsA compared with 18 (7.2%) in the vehicle group.
Leonardi et al. (2016) reported any ocular treatment-emergent AEs in 112 (73%) participants in the CsA group compared with 44 (49%) in the vehicle group. Severe ocular treatment-emergent AEs were observed in 19 (10.4%) participants in the CsA group compared with 8 (8.9%) in the vehicle group. Instillation site pain was more common among CsA-treated patients (29.2% vs. 8.9%).
In the Peng et al. (2024) study, ocular treatment-emergent AEs were again higher in the CsA group [42 (40.8%) vs. 27 (26.2%)]. Key events included visual acuity reduction [13 (12.6%) vs. 18 (17.5%)], ocular discomfort [4 (3.9%) vs. 2 (1.9%)], and instillation site reactions [3 (2.9%) in the CsA group, none in the vehicle group].
In the Wirta et al. (2019) study, discontinuation due to AEs was reported in two (3.8%) patients in the vehicle group and none in the CsA group, while visual acuity reduction occurred in four (7.8%) patients in the CsA group compared with one (1.9%) in the vehicle group.
Finally, in the ESSENCE-1 trial (Sheppard et al., 2021), ocular treatment-emergent AEs were reported in 31 (19.1%) participants in the CsA group compared with 23 (13.8%) in the vehicle group. Instillation site pain was more frequent in the CsA group (2.5% vs. 1.2%), while blurred vision was slightly more common in the vehicle group (2.4% vs. 1.2%).
A summary table of the AEs recorded in each included study is presented in Supplementary Table S1.
Discussion
In this systematic review and meta-analysis of six studies, we compared for the first time the use of ophthalmic 0.1% CsA in 1,119 (51,56%) patients, while 1,051 (48,44%) received the vehicle solution in the treatment of DED. Our results revealed significant efficacy of 0.1% CsA in DED compared with their vehicle with the following key findings: (1) CsA improves tCFS more effectively as early as 4 weeks (MD −0.64; P = 0.003), (2) 0.1% CsA water-free solution improves cCFS (MD −0.19; P = 0.02), (3) 0.1% CsA water-free solution improves LGCS score (MD −0.51; P = 0.0002), (4) 0.1% CsA improves overall OSDI scores (MD −3.04; P = 0.03), (5) 0.1% CsA solution had a higher incidence of ocular AEs than vehicle, but these were mostly mild to moderate, highlighting their favorable tolerability. No significant differences were found in dryness scores and blurred vision scores. Notably, this meta-analysis represents an important updated synthesis of data in this domain since three articles selected were published after the two existing meta-analyses, had more than double the number of patients, and made an unprecedented comparison between existing studies.17,20–23
Our meta-analysis found that 0.1% CsA significantly improves tCFS as early as 4 weeks into treatment. Notably, the data contributing to the effect at 4 weeks predominantly came from the water-free (SFA-based) 0.1% CsA solution program. This emphasizes the importance of considering formulation differences when interpreting these results. Previous studies have documented the efficacy of CsA compared with vehicles in reducing corneal staining due to its fast anti-inflammatory action. 24 Cyclosporine acts by inhibiting the activation of T-cells by inhibiting calcineurin, the nuclear factor of activated T-cells, and interleukin-2, thus reducing the inflammatory process, which contributes to symptom relief. 5 Some studies report a longer time for significant improvement in tCFS, ranging from 6 to 12 months.25,26 However, the reason for these differences in treatment time was neither explained nor discussed in the studies evaluated. Also, of all studies used in this analysis, four (Essence-1 and -2, Peng and Wirta) used the NEI score while two (Baudoin and Leonardi) used the modified-Oxford scale to assess corneal staining. The Oxford scale goes from 0 to 5, divides and assesses the whole cornea, and is graded by a log-linear increase in the number of dots, whereas the NEI scale goes from 0 to 15, divides the cornea into five zones (superior, inferior, central, nasal, and temporal), and the grades increase with number and density of dots. 27 While both scales use drawings to depict the location of corneal staining, they cannot be directly translated into each other. This, however, does not invalidate our findings since we used standardized MD to calculate this outcome as described in the Cochrane Handbook. Additionally, differences in the studied populations may have influenced the results. While all studies enrolled patients with moderate-to-severe DED, the Leonardi study included only patient population with severe DED due to the inclusion criteria which translates into a higher basal tCFS score (grade 4 on the Oxford scale). This contrasts with other studies that included patients with moderate-to-severe DED and varying staining scores. This heterogeneity in baseline severity and different scales (NEI and Oxford) may impact the generalizability of the findings.
Our results also showed that 0.1% CsA water-free (SFA-based) solution improved cCFS. Previous studies have shown the central region of the cornea in DED is associated with worst symptoms and visual impairments.28–30 We were not able to evaluate this in 0.1% CsA cationic emulsion as none of the studies reported this outcome.
Compared with vehicles, 0.1% CsA was shown to significantly improve LGCS and OSDI scores due to its anti-inflammatory properties. which aligns with results from previous studies.31,32 Ayres and Park’s trials used 0.05% CsA and reported, respectively, improvement in OSDI and LGCS scores at 6 months, and OSDI scores showed significant improvements at 3 months.31,32 A different trial used 0.1% topical CsA in chondroitin sulfate emulsion for the treatment of dry eyes and showed an improvement in OSDI in just 3 months. 33 Although the vehicle may contribute to the stability and penetration of the medication, the pharmacological action of CsA probably results in the improvement of dry eye symptoms. The vehicle plays a critical role in DED treatment as it may influence the bioavailability and efficacy of the active agent, potentially contributing to symptom relief. Vehicles used in DED therapies can stabilize and enhance drug penetration, improving the pharmacokinetic profile of the medication. While the pharmacological action of CsA remains the primary therapeutic factor, the supportive role of vehicles in enhancing efficacy should not be underestimated. Future studies should evaluate the impact of different vehicles in the context of CsA formulations to better understand their contributions to treatment outcomes. Articles disputing this claim were not found, which reinforces these findings.
We found no significant difference in dryness score in the maximum follow-up of 6 months, but the short follow-up time evaluated may have influenced these results. This finding contrasts with some reports in the literature which suggested CsA could reduce dryness symptoms compared with vehicles. Yet, these were uncontrolled studies that had a follow-up time of 12 months.34–36 Similarly, there was no significant difference in the blurred vision score assessed by the VAS. While observational studies and the pooled analysis of ESSENCE-1 and -2 studies have reported improvements, our analysis showed no significant results, which may be attributed to variations in study designs, patient populations, different protocols, or follow-up time.34–37 Interestingly, blurred vision symptoms typically improve as cCFS is reduced, owing to an enhanced corneal surface that facilitates better image projection onto the retina.28,30 However, our study found that despite improved cCFS scores, this did not directly correlate with improvements in blurred vision symptoms. This suggests the need for further research to clarify the impact of these treatments on eye dryness and blurred vision.
This study has important limitations. Significant variability was noted in the treatment duration and follow-up period across studies. The longest follow-up time was 6 months in one study, which can be considered short since DED requires long-term treatment. 5 Therefore, long-term efficacy could not be assessed. Additionally, with the exception of two studies, most patients had aqueous-deficient DED, leaving it uncertain whether 0.1% CsA would be effective for other forms of DED.38,39 A recent study reports that there was only improvement among patients with aqueous-deficient dry eye and not with steroid-refractory mixed-type dry eye. 40 Furthermore, there was significant heterogeneity in the outcomes of tCFS and OSDI scores, which may impact the generalizability of the results. Finally, to achieve some of the study outcomes, we combined data from two different 0.1% CsA products [water-free (SFA-based) solution and cationic emulsion], which present slightly different pharmacokinetics and are compounded with different vehicles. Random effects, quality assessment, and sensitivity analysis were used to mitigate these limitations.
Conclusions
Overall, 0.1% CsA appears to be a good treatment option for DED improving tCFS, cCFS, OSDI, and LGCS. However, a larger sample with long-term follow-up RCTs and standardized outcome measures is needed to better understand its efficacy and safety profile.
Footnotes
Acknowledgments
The authors extend their gratitude to their adviser, Jaime Guedes, for his support, guidance, and motivation throughout this challenging project. They also thank Professor Rhanderson Cardoso for his teaching on meta-analyses. The authors are grateful for the encouragement from friends, mentors, and colleagues who kept them focused and helped them overcome many obstacles.
Authors’ Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Informed Consent
Informed consent was obtained from all patients involved in this study.
Author Disclosure Statement
The authors declare no competing interests related to this study.
Funding Information
The authors received no specific funding for this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.