
Abstract
Purpose:
Steroid-induced ocular hypertension is poorly understood in children, despite its frequent occurrence. Significant knowledge voids exist in steroid responsiveness, especially in the pediatric population. Therefore, highlighting the most critical risk factors in pediatric patients can help ophthalmologists identify who is at increased risk of developing a high steroid response.
Methods:
A manual search was conducted in PubMed and Google Scholar in search of relevant articles on the steroid-induced glaucoma subtopic.
Results:
Key risk factors for high steroid response include glaucoma family history, previous glaucoma diagnosis, young age, steroid type, administration route, and diseases such as vernal keratoconjunctivitis (VKC) and uveitis. Clinically, it presents similarly to primary glaucoma, except for steroid usage history. Steroid cessation or reduction can normalize intraocular pressure (IOP) levels; however, in some cases, pressure-lowering drugs are necessary for treatment.
Conclusion:
Topical ocular steroids are frequently used by pediatricians and ophthalmologists alike. Understanding the importance of risk factors allows for a timely diagnosis of steroid response and adequate treatment before glaucomatous vision loss can occur.
Introduction
Steroids are routinely used in ophthalmological practice. They act through the cytoplasmic glucocorticoid receptor, forming a complex with the ligand to induce downstream effects at a genetic and epigenetic level, intending to reduce inflammation. 1 Corticosteroid drops can increase intraocular pressure (IOP), which may lead to steroid-induced glaucoma (SIG). Other side effects include cataracts, ptosis, globe rupture, systemic toxicity, and uncontrolled hyperglycemia. 2
Armaly and Becker divided population into three groups according to IOP response to potent steroids. (FIG. 1.). High responders developed IOP above 31 mmHg or a rise of more than 15 mmHg above baseline with topical steroid application; moderate responders, who had IOPs between 20 and 31 mmHg, or a pressure rise of 6–15 mmHg; and nonresponders, who had pressure increases of less than 6 mm Hg, and IOPs of less than 20 mmHg. High responders correspond to approximately 4%–6% of the population; moderate responders, approximately one-third of the population; and nonresponders, the remaining two-thirds.3,4
Although previously stated otherwise, young children exhibit more aggressive responses than adults, and it has been stipulated that the phenomenon is more frequent in proportion. Ohji et al. found a difference when dexamethasone was administered to children under the age of 10, where 9 out of 11 patients had significant IOP rises, and 5 were high responders. Those above the age of 10 also treated with dexamethasone did not achieve IOP values above 20 mmHg. 5
Most children who are administered steroids do not present risk factors associated with steroid responsiveness in adults such as previously diagnosed primary open-angle glaucoma (POAG), advanced age, diabetes mellitus, or rheumatoid arthritis. 6 Because children differ from adults, understanding factors predisposing them to steroid response is crucial. 5
The exact mechanisms by which steroids induce IOP elevation have yet to be fully elucidated 7 ; however, recent investigations suggest multiple pathways increase resistance to aqueous humor outflow.
Trabecular membrane extracellular matrix
Steroids increase the expression of multiple extracellular matrix (ECM) proteins, which deposit in the trabecular meshwork, causing glycosaminoglycans (GAGs) to accumulate in the juxtacanalicular region’s extracellular spaces and beneath the Schlemm canal’s endothelial lining. (FIG. 2.). Also, thickened trabecular beams and decreased intertrabecular spaces are observed. GAG deposition attracts water, creating thickened and edematous trabecular beams that decrease intertrabecular spaces, further decreasing aqueous humor outflow.8,9 These GAGs include mainly fibronectin, laminin, and collagen type IV. In addition to increased ECM deposition, in vitro studies of trabecular meshwork cells show cellular changes consistent with increased protein synthesis and posttranslational modifications.10,11
Cross-linked actin networks
Steroid exposure rearranges cytoskeletal actin stress fibers into cross-linked actin networks (CLANs). Increased CLAN presence in trabecular meshwork cells of glaucomatous subjects suggests they have a role in steroid response pathophysiology. 11 Current evidence suggests that trabecular meshwork cell contraction, where actin plays a role, helps regulate aqueous humor outflow. Duffy et al. proposed that a TGFβ1/Smd pathway induces CLAN formation, reducing trabecular meshwork cell contraction and elevating IOP. 12 In addition, changes in actin microfilaments decrease phagocytosis by trabecular meshwork cells, contributing to outflow resistance and IOP elevation. 13
Decreased degradation of proteins
Steroid therapy inhibits tissue plasminogen activator, which functions as a matrix metalloproteinase (MMP) that regulates ECM protein deposition. Snyder et al. studied cell and organ culture supernatants where dexamethasone inhibited tPA and 92 kD type IV collagenase. 14
Genetics and pathways
Rozsa et al. described an increased expression of the MYOC gene after dexamethasone treatment of the trabecular meshwork, which induces protein accumulation in the intertrabecular spaces.10,15 Badrinarayanan et al. established an association with variants in the CRPPA, PLOD1, and ARHGAP1 genes influenced a secondary IOP rise in subjects treated with triamcinolone through a deregulated metabolic pathway and Rho GTPase-mediated cytoskeletal regulation pathways. 16 Kasetti et al. demonstrated that dexamethasone also increases the concentration of TGFβ2 in human eyes, triggering the SMAD pathway and increasing ECM synthesis and deposition, thereby elevating IOP. 17 Lütjen-Drecoll hypothesized that TGFβ plays a role in POAG development. Eyes treated with TGFβ show increased ECM protein concentration, including plasminogen activator inhibitor, downregulating MMPs and increasing αβ crystalline, myocilin, fibronectin, and type I collagen expression through the SMAD signaling pathway.15,18,19
Myofibroblasts
Zhu et al. suggested that dexamethasone induces myofibroblast guanine nucleotide exchange factor (GEF) ARHGEF26-mediated transdifferentiation in trabecular meshwork cells. GEFs are proteins that activate Rho GTPases, which regulate multiple cytoskeletal processes. In the study, knockdown of ARGHEF26 protected trabecular meshwork cells from dexamethasone-induced transdifferentiation into myofibroblasts. Myofibroblast presence suggests alterations in cell morphology, migration, contraction, proliferation, and ECM production. 20
Methods
PubMed and Google Scholar databases were manually searched using the keywords “pediatric,” “steroid,” “response,” and “glaucoma” from August 2024 to November 2024, no time limitations were used. Afterward, cite search of previously selected studies was performed to obtain new sources of information on the topic. Every type of study was included in the literature review. Results were screened on the following criteria: (1) articles needed to contain at least one of the keywords, (2) the topic of studies needed to be SIG or steroid-induced hypertensive response and contribute significantly to the narrative approach of this literature review, and (3) publications were not book chapters or abstracts.
Results
Age
Ohji et al. reported that in children younger than 10 treated with dexamethasone, 9 out of 12 had IOP elevation greater than 5 mmHg, and 4 of those were higher than 10 mmHg; in contrast, no patients above 10 years old, treated with dexamethasone, suffered from IOP elevation greater than 5 mmHg. 5 In addition, Sugiyama et al. found that IOP of children younger than 9 was significantly influenced by dexamethasone compared with patients older than 10. 21 Krag et al. stated that pediatric steroid responders tended to be younger (median age 9, range of 5–15) than nonresponders (median age 15, range of 7–17). 22 In a prospective study, Takano et al. described a cutoff value of 11 years of age, and Alotaibi et al. provided a meta-analysis indicating risk peaks around age 6.23,24
Race and ethnicity
Even though Black and Hispanic pediatric populations have an increased risk of being glaucoma suspects, no conclusive association has been found between race and ethnicity and risk for developing SIG.13,25 Krag et al. hinted at the possibility of steroid responsiveness being greater in Asian children; however, Nuyen et al. reported no association existed between SR and a particular race or ethnicity.13,22 Multicentric studies regarding SIG should be conducted to determine race and ethnicity’s relevance in steroid response.
Glaucoma family history
Tripathi et al. acknowledged that family history is a risk factor for developing high steroid responses. 8 Ozturk et al. investigated IOP elevation in children administered intranasal steroids for allergic rhinitis, noting that elevations were more clinically significant in children with positive family history of POAG. 26 Ang et al. found that none of the patients who developed a steroid response had a positive family history of glaucoma; however, they acknowledge that small sample size was a limitation in their study. 27 Therefore, because previous studies have inconsistent findings, studies with larger samples may determine whether family history is a risk factor.
Previous glaucoma diagnosis
Armaly stated that approximately 30% of glaucoma suspects and 90% of patients with POAG had a high response to 1-month dexamethasone therapy, and even those patients with POAG who were not high responders were classified as medium responders. In a literature review, Phulke et al. state that high responders have greater risk of eventually developing POAG; however, more studies are needed to characterize this association further.9,26
Steroid type
Pleyer et al. compared data from multiple studies regarding IOP elevation in older versus newer steroids, concluding that dexamethasone and prednisolone have a stronger IOP-raising effect compared with fluorometholone, rimexolone, and loteprednol. 28 Kwok et al. described a mean maximal IOP change and the mean peak IOPs were 15.48 ± 8.71 mmHg and 30.66 ± 8.71 mmHg, respectively, in patients treated with dexamethasone versus 5.83 ± 4.96 mmHg and 20.66 ± 6.03 mmHg in those treated with fluorometholone. Eyes that received dexamethasone exhibited intermediate to high response in 15 out of 16 patients, compared with one high responder in the fluorometholone group. 29 Ohji et al. found that steroid responses of children under the age of 10 treated with dexamethasone were greater than those treated with fluorometholone. 5 Al Hanaineh et al. achieved similar results comparing dexamethasone, fluorometholone, and rimexolone, stating that dexamethasone elicits greater responses. 30 Sen et al. also found that dexamethasone and betamethasone show increased mean peak IOP and disc cupping values compared with prednisolone or fluorometholone. 31
In a study by Morrison, high steroid responders were exposed to fluorometholone, and one out of three responded similarly to dexamethasone. 32 Fan et al., however, proposed that fluorometholone response in children occurs in a dose-dependent manner after their prospective study indicated that higher doses produced higher mean peak IOP and quicker onsets. In addition, the anti-inflammatory effects did not differ between groups. 33 A review by Mataftsi et al. further supports the claim that the IOP-elevating effect of fluorometholone is dose-dependent and dose reduction is a safe practice. 34
Slabaugh et al. reported a 50% incidence of steroid response following treatment against uveitis with difluprednate. Even though patients with uveitis are at increased risk of decreased aqueous humor outflow, difluprednate is a steroid highly associated with side effects. These factors combined may have contributed to high incidence of steroid response in this study. 35
Loteprednol has been reported to have a better side effect profile. Bartlett et al. conducted a crossover study in known steroid responders, demonstrating that treatment with loteprednol had a significantly lower IOP elevation when compared with prednisolone (4.1 mmHg versus 9 mmHg, respectively) and achieved similar anti-inflammatory effects. 36 Further investigation into the effect of loteprednol in the pediatric population with known steroid response is warranted.
Loading dose
Ng et al. stated that the hypertensive response to dexamethasone occurs dose-dependently. The net increase in patients treated with BID dexamethasone was 10.9 ± 5.8 mmHg compared with 14.5 ± 6.4 mmHg in the QID group. 37 Patel et al. described the safety profile of subtenon triamcinolone injections in pediatric patients with no risk factors, showing a favorable review of low doses. 38
Cingu et al. reported that retinal nerve fiber layer (RNFL) thickness in children treated for vernal keratoconjunctivitis (VKC) was negatively correlated with steroid therapy duration. Whether the decrease in RNFL thickness is due to glaucomatous nerve damage is hard to determine because performing visual field analysis in children is difficult. 39 Further investigation is required to determine the effect of steroid use on RNFL thickness in pediatric patients.
Administration route
Topical administration of steroids is common in ophthalmology, and approximately three-fourths of SIG cases occur with topical therapy due to its direct action and frequent use.1,8 Despite greater IOP elevation risk with topical steroids, Yamashita et al. report that steroid response to systemic steroids in children has been underestimated. In addition, Kaur et al. state that the effect of systemic steroids on IOP may be underreported because those exposed to long-term, high-dose steroid therapy often suffer from systemic conditions in which steroids are required. Also, ocular hypertension is usually asymptomatic, so children may not complain.40,41 According to de Queiroz et al., the main factors contributing to glaucoma with systemic steroid treatment are IOP level and duration of IOP elevation. 42
Several other authors have described cases where high-loading doses of strong systemic steroids produce aggressive IOP responses in children. These exaggerated responses were controlled with steroid cessation and/or antiglaucomatous medication.43–45 Kaur et al. report that steroid responses due to systemic steroids were more controllable with antiglaucomatous medications than responses elicited by topical steroids. 41
Inhaled steroids’ role in steroid response is unclear. Emin et al. studied asthmatic children treated in long term with inhaled fluticasone and concluded that an average dose of 320 µgdaily is not associated with ocular side effects. 46 Ozturk et al. reported a clinically significant increase in IOP in pediatric patients with glaucoma family history or previously cupped discs after using intranasal mometasone. 26 Yuen et al. concluded that intranasal beclomethasone, which has high bioavailability, did not precipitate an IOP increase in high-risk patients with either ocular hypertension or glaucoma. 47 In a meta-analysis by Lipworth, patients treated with inhaled or intranasal steroids continuously for more than three months were at a slightly increased risk of IOP elevation. Therefore, caution is recommended during long-term use of steroids through inhaled or intranasal route. 48
In a review by Razeghinejad et al., IOP response following intravitreal steroid injection was evaluated, and steroid response incidence ranged between 20% and 65%; this wide value range is explained by the analyzed studies varying in steroid dose, sample size, and inclusion of treatment-naïve subjects. In addition, younger patients were more likely to demonstrate a steroid response. Also, Breusegem et al. showed that known dexamethasone responders had stronger responses to intravitreal triamcinolone than nonresponders.6,49
Among periocular routes, subtenon injection presents increased steroid response risk compared with conjunctival routes because it reaches greater concentrations within the retina and vitreous. Liu et al. found that the posterior subtenon route presents greater risk than the anterior, 2.4 times more likely to cause IOP levels above 21 mmHg, and 5.3 times above 30 mmHg.1,50 Younger age, higher baseline IOP, increased triamcinolone dose, number of injections, myopia, and concomitant administration of intravitreal triamcinolone have been identified as risk factors for IOP elevation in studies investigating the subtenon route.1,38
Some reports previously suggested that topical periocular steroids can induce steroid response, possibly due to thinner stratum corneum of the periocular skin, higher blood vessel density, and higher absorption rate in the palpebral region compared with other locations.1,51 Haeck et al. evaluated the cumulative effect of periocular topical steroids for atopic dermatitis involving the eyelids in adult patients for 2–5 years and found that 1 of 88 patients developed a transient increase in IOP, which normalized despite continuous use of steroids; however, this study was limited due to possible recall bias and overestimation of steroid use by the pharmaceutical records. Literature investigating the cumulative effect of periocular topical steroids on IOP is sparse; therefore, further research is recommended. Still, IOP screening for patients who undergo long-term topical periocular steroid treatment is advised. 52
Uveitis
Uveitis is unique since both the disease and the treatment cause IOP increase and potential glaucomatous nerve damage; therefore, determining the exact cause of IOP elevation may be difficult. Studies have shown two IOP peaks in the disease: the first one within days attributed to steroid response and another one within months or years attributed to the disease. Nuyen et al. state that peripheral anterior synechiae upon gonioscopic exploration points toward angle changes due to the uveitic inflammation, while a normal anatomical appearance suggests steroid response. 13
IOP spikes have been reported with different types of uveitis, including juvenile idiopathic arthritis (JIA) uveitis, sarcoidosis uveitis, pars planitis, and idiopathic uveitis. Nuyen et al. stated in their literature review that JIA uveitis is more related to steroid response than non-JIA uveitis. Foster et al. reported that one-third of patients developed glaucoma after JIA uveitis, and due to the aggressiveness of JIA uveitis, it requires treatment with strong steroids, exacerbating risk for steroid response.13,53
Sallam et al. compared hypertensive responses between steroid responders and nonresponders in patients with uveitis, finding that known steroid responders whose aqueous humor outflow is already compromised experience more dramatic steroid responses. This study suggests that most cases of IOP elevation in uveitis were due to steroid response, and IOP was more manageable after steroid response than hypertension due to the inflammatory process. Among the eyes that experienced IOP spikes, 34.5% had glaucoma. 54 Additional research is required to determine how different types of uveitis affect steroid response in pediatric populations.
Vernal conjunctivitis
Among allergic conditions affecting the eye, the one that has demonstrated most association with steroid responsiveness has been VKC, which is a common disease affecting children worldwide and is treated with topical steroids. In a review by Nuyen et al., the incidence of SIG in patients treated for VKC was reported between 2% and 8%. Bonini et al. state that glaucoma incidence in patients treated for VKC was 2% and suggested that steroid misuse was an important factor leading to this complication. 55 Ang et al. reported a 5.5% incidence of SIG in Singaporean children with VKC. Limbal neovascularization, associated with VKC, indicated a 4- to 6-fold increased risk of developing SIG, and mixed VKC presented a 10-fold increase in risk with poorer long-term visual outcomes. 27
Mixed VKC is more associated with high steroid response and leads to poorer outcomes since it involves the tarsal conjunctiva and the limbus. 13 Sen et al. reported that mixed VKC was most associated with SIG, followed by the palpebral form. Various studies determined that many SIG cases were due to long-term misuse of steroids.27,31,56 Gupta et al. found that most SIG cases at their glaucoma center in India were due to steroids prescribed for VKC. 56
Clinical features
Clinical evaluation of children with steroid response or SIG differs slightly from adults since the upper limit of normal IOP in pediatric patients is lower. 13 IOP elevation generally occurs after 3–6 weeks of continuous steroid use and usually normalizes within 2 weeks of cessation if irreversible trabecular meshwork changes have not occurred. However, steroid response can develop as soon as few hours after initiation of steroid therapy. 1
Clinical presentation depends on the age of onset. In infants, SIG presents similarly to primary congenital glaucoma and includes signs such as decreased vision, increased IOP, optic nerve atrophy, and edematous, sometimes buphthalmic, corneas. 8 Hajiyev proposed that the younger a patient is exposed to steroids, the more likely buphthalmos develops because of IOP increase. 57 In older children and adults, clinical presentation of SIG is similar to POAG or juvenile open-angle glaucoma. The main difference between SIG and other types of glaucoma lies in steroid usage.2,8 Elevated IOP, unless rapid and severe, is typically asymptomatic and is found either coincidentally, or after irreversible visual field loss. 41
Time to peak IOP is apparently unrelated to any previously described risk factors, with studies finding no association between them.22,29 Previously, literature established that IOP responses occurred after at least 2 weeks of steroid therapy. Alotaibi et al. agree that steroid responses normally take 2 weeks to develop but can also occur within the first hours. 23 Lai et al. report a case where a leukemia patient developed high steroid response after 5 days on systemic dexamethasone, and Hutcheson reported a case of SIG after 7 days.43,58 In Krag et al.’s prospective study, mean time to peak IOP was 33 days, but with high variation range, with the earliest diagnosis being 11 days. 22
It is difficult to estimate risk of progression from steroid response to SIG because it depends on many factors, including individual patient circumstances. According to Senthil et al., among more than 4,000 patients who presented VKC, 91 had developed SIG and approximately one-third were bilaterally blind. 59 In a study of over 1,200 glaucoma patients by Gupta et al., 59 cases were due to steroids, and among these, 37.3% had glaucomatous nerve damage and 29% were unilaterally blind. However, both studies are retrospective and conducted in India; therefore, a multicentric study where patients come from different genetic, socioeconomic, and cultural backgrounds may offer a different outlook on the disease’s natural history.
Although mild IOP elevation may go unnoticed, significantly elevated IOP may cause corneal edema, blurred vision, vision halos, and ocular or ciliary pain. In some cases, significant IOP elevation is associated with the development of posterior subcapsular cataracts. This complication usually occurs when high IOP values are reached rapidly, similar to acute angle closure glaucoma. 6
Steroid-induced IOP elevation typically resolves within 1–4 weeks of steroid cessation; however, in about 3% of cases, usually in individuals with a family history of glaucoma or chronic steroid use, ocular hypertension does not improve. If it does not normalize, the use of antiglaucoma medications or IOP-lowering procedures is required. 2
Management and treatment
IOP should be monitored before and throughout steroid therapy. 2 Lower IOP leads to better prognoses, marking the importance of early diagnosis of steroid response. 41 Conversely, higher IOPs correlate with worse vision prognosis, long-term treatment requirement, and glaucoma surgery. 56
Since steroid response is usually reversible, complete cessation is recommended.1,13 If cessation is not possible, alternative methods such as lowering steroid concentration or switching to steroid-sparing agents, should be attempted.2,13 In the case of topical therapy, nonsteroid anti-inflammatory drugs can be considered, and in systemic steroid treatment, switching to immunomodulators.
If antiglaucoma medications are required, these cases are usually managed similarly to POAG. β-blockers are a popular first-line therapy, often followed by carbonic anhydrase inhibitors either by topical or systemic route.6,13 Prostaglandin analogs are commonly used antiglaucoma medications, and even though they have been tied to uveitis flares in some case reports, it is suggested they are safe in uveitis patients. 54
About 1%–5% of patients with SIG need surgery to control IOP levels appropriately. 60 Surgery is often needed in cases of uncontrolled SIG following steroid treatment for JIA uveitis, and various surgical techniques are effective.13,61 Argon laser trabeculoplasty is not effective for long-term prevention or treatment of patients with steroid response, and most require surgery within 3–6 months.1,62 Roberti et al. report that future therapies being considered for steroid response include tPA, which could help in ECM degradation, and gene therapy vector GC-MMP1. 1
Discussion
Steroid response was initially speculated to be less aggressive in children than in adults. In one of the first studies describing the phenomenon, Armaly stated that steroid response was greater in older than younger eyes. 3 Kwok et al. indicate that extensive studies about steroid response exist, but few study the pediatric population. 29 Kaur et al. conducted a retrospective study in pediatric patients under 12 and found that 24% of cases of acquired glaucoma were attributable to topical steroids. 41 Currently, there are no reliable estimates of the incidence and prevalence of pediatric steroid response or SIG. In addition, direct comparisons of steroid response between children and adults are scarce. Still, studies like Ohji et al. and Kaur et al.,5,41 among others, demonstrate evidence that pediatric patients show stronger steroid responses than adults.
Even though there is a poor understanding of the steroid mechanism of action, they have important effects on the trabecular meshwork. Following steroid application, TGFβ pathway genetic interactions result in increased ECM component expression, cell transdifferentiation to myofibroblasts, and reduced proteolysis and apoptosis in trabecular meshwork cells, disrupting the balance between deposition and proteolysis with subsequent reduction in intertrabecular spaces. Steroids also promote CLAN formation, interfering with phagocytic activity and increasing rigidity in trabecular meshwork cells. A rigid trabecular meshwork with decreased spaces increases resistance to aqueous humor outflow, increasing IOP and leading to glaucomatous nerve damage. Applying steroids in immature pediatric trabecular meshworks 63 adds another layer of outflow resistance, predisposing children to aggressive IOP spikes. In addition, the presence of certain genetic variants in the population may increase risk for steroid response, but more studies are needed to define what genes cause high steroid responses. 16
According to Reme and Lalive D’epinay, trabecular membrane maturity is reached approximately at the age of 8, making young children particularly prone to IOP spikes after steroid treatment. 63 Ohji et al. strengthened this hypothesis by applying the same steroid therapy to pediatric patients below and above the age of 10, and younger ones were more susceptible to high response. 5 Family history of glaucoma and previous glaucoma diagnosis are important risk factors. Ozturk et al. suggest that a family history of POAG directly influences steroid response in patients during the first week of treatment. Ozturk et al.’s study was conducted with intranasal steroids, which are less associated with steroid response and could signify family history is a risk factor. 26 Further studies in patients with known family history are warranted to establish its impact as a risk factor.
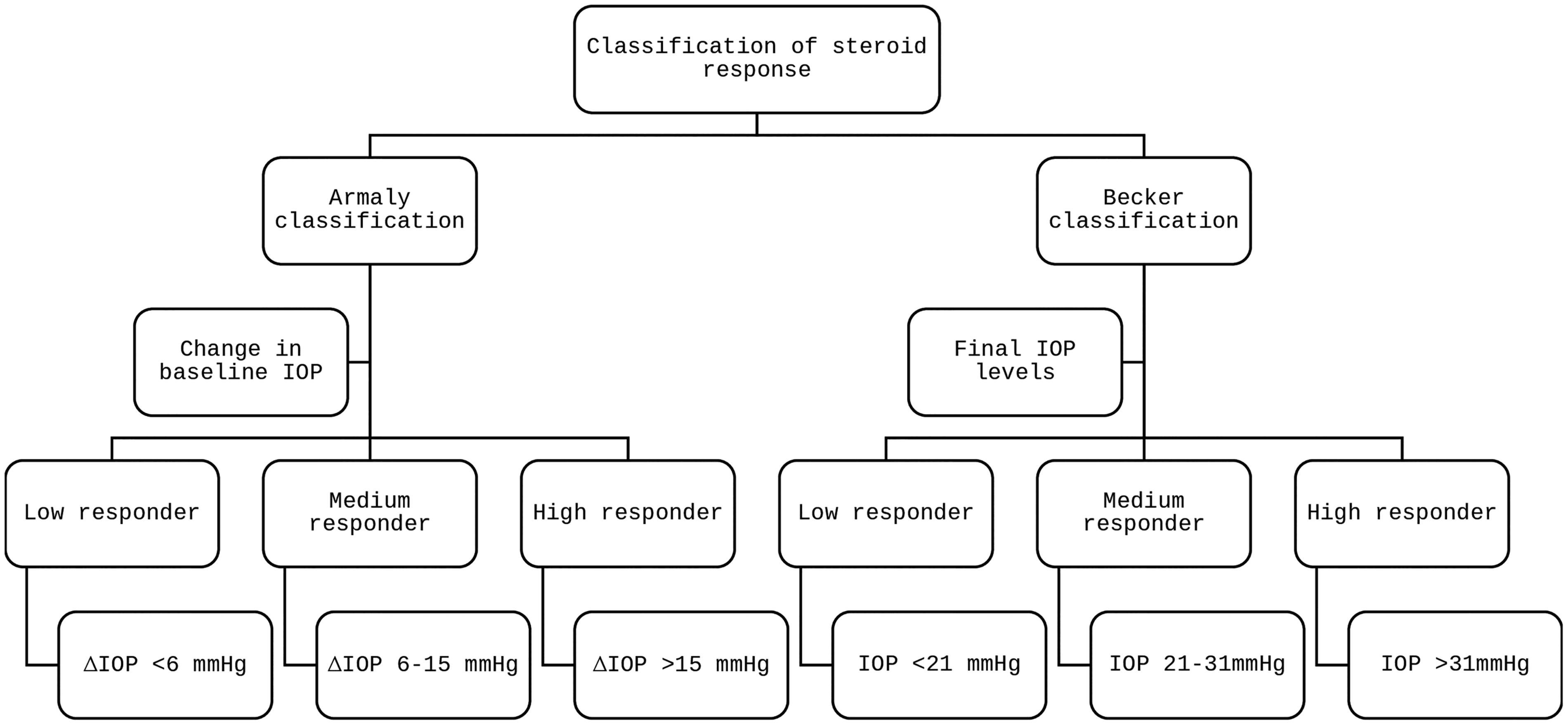
Diagram explaining steroid response’s classification.
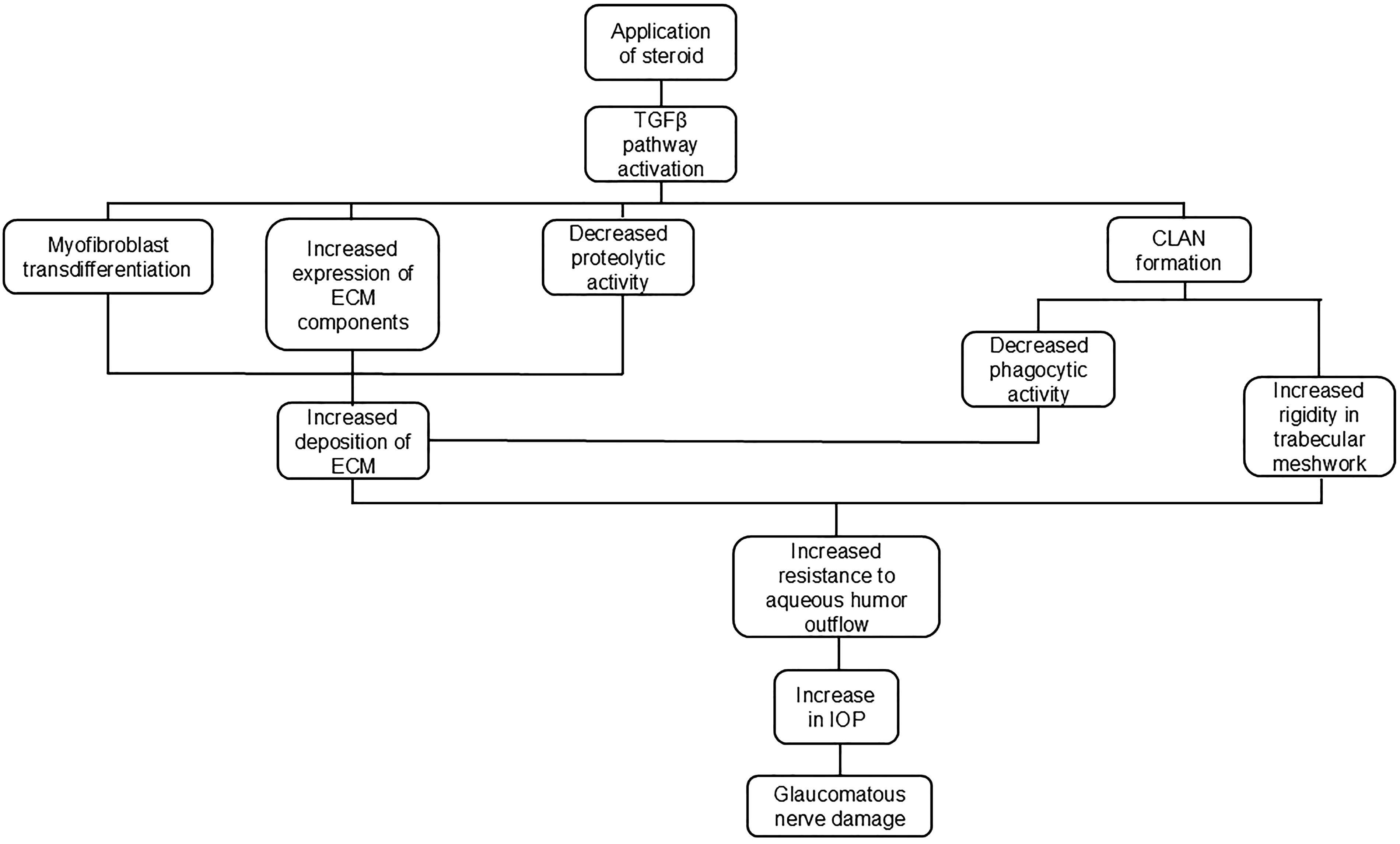
Diagram synthesizing steroid response pathophysiology.
Treatment with strong steroids, a high-loading dose, and direct administration can directly influence the steroid response. Among different types of steroids, dexamethasone, prednisolone, betamethasone, and difluprednate produce higher IOP spikes in comparison with softer steroids, even though fluorometholone produces high IOP elevation in known steroid responders. 32 For that reason, loteprednol has been proposed as a safe alternative, 36 but since it is not as strong, it is not routinely used first-line.
Most cases of SIG result from exogenous glucocorticoid administration by topical, periocular, or systemic routes. 8 Intravitreal and periocular steroids pose a significant risk for SIG because of their long duration of action, 9 increasing the importance of maintaining strict IOP surveillance. Multiple studies and case reports suggest that steroid response risk during systemic steroid therapy is low. However, maintaining high doses for long term increases the risk for IOP spikes that may go unnoticed. Finally, inhaled, intranasal, and periocular skin administration produce controversial evidence on SIG association. Nonetheless, IOP vigilance is advised if steroid medication, regardless of administration route, is used long term.
High myopia has been described in some instances as a risk factor; however, Park et al. could not find an association, and Cingu et al. did not find a correlation between high axial length and RNFL thickness in children.39,64 Even though most evidence suggests no association between high myopia and high steroid response, cautious observation should be exercised on high myopic patients.
Diseases such as VKC and uveitis are major risk factors for developing high steroid response. VKC is a common pediatric pathology treated with topical steroids. Since the mixed type is the most severe form, stronger steroids and doses are usually required, posing a risk for steroid response. 13 Gupta et al. reported that a high percentage of children with VKC were blind due to steroid misuse; however, their study was conducted in an Indian tertiary center, where steroid sales are less controlled, and incidence could be higher than in other countries. Uveitis is unique because the disease and the treatment can elevate IOP and be mutual confounders. Angular structure inflammation exists in uveitis; therefore, steroid side effects are expected to create an IOP spike. Sallam et al. cite that approximately one-third of patients with steroid response to uveitis treatment developed glaucoma, and Nuyen et al. report on another study that has similar results.13,54 One of the main reasons SIG develops worldwide is indiscriminate steroid use, so patient and parent education is fundamental to prevent SIG in children due to long-term, indiscriminate treatment.
In conclusion, since children have stronger and faster IOP responses than adults, strict vigilance during steroid therapy allows for timely responses. Steroid discontinuation usually normalizes IOP levels; however, antiglaucoma medications are required in failure to regress. Glaucomatous nerve damage can quickly develop if steroid response is undiagnosed or improperly managed. Identifying potential risk factors in patients allows for stricter vigilance to diagnose early a steroid response, allowing ophthalmologists to take action in preventing evolution to glaucoma, which is avoidable when steroid response is treated accurately. Further investigation is needed in children to establish guidelines to diagnose and treat steroid response, avoid glaucoma progression, and understand its impact on society.
Footnotes
Acknowledgments
The authors extend special thanks to Wisam Najdawi, BS, for guidance during the writing process.
Authors’ Contributions
S.L.: Conceptualization, methodology, validation, investigation, writing—original draft, writing—review and editing, visualization, and project administration. A.M.: Conceptualization, methodology, validation, investigation, writing—review and editing, and visualization. E.B.: Conceptualization, methodology, validation, investigation, visualization, writing—review and editing, supervision, and project administration.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was secured for this study.