
Abstract
Purpose:
Glaucoma, a neurodegenerative condition of the optic nerve is driven by increased intraocular pressure (IOP) due to fibrotic changes of the trabecular meshwork (TM). Interferon beta (IFN-β), a pleiotropic cytokine is known for its neuroprotective and antifibrotic potential. Hence, we investigated the intraocular status of IFN-β in patients with primary glaucoma.
Methods:
Aqueous humor (AqH) from patients with primary glaucoma [107 eyes; primary open-angle glaucoma (POAG), 59 eyes; primary angle-closure glaucoma (PACG), 48 eyes] and controls (70 eyes) were collected during cataract surgery and/or trabeculectomy. TM from patients with POAG (20 eyes) and PACG (18 eyes) was collected during trabeculectomy. IFN-β in AqH was measured using bead-based Enzyme-Linked Immunosorbent Assay (ELISA), and messenger RNA (mRNA) expression of IFN-β in TM was measured by quantitative PCR.
Results:
AqH-IFN-β levels were significantly (P < 0.05) lower in patients with glaucoma, particularly in patients with POAG compared with controls (area under the receiver operating characteristic curve = 0.723, P < 0.001; odds ratio of 5.1, P < 0.0001). AqH-IFN-β levels correlated positively with visual field index of both patients with POAG (r = 0.307; P = 0.0321) and PACG (r = 0.518; P = 0.0007). Whereas, AqH-IFN-β levels correlated positively with retinal nerve fiber layer thickness in patients with POAG (r = 0.460; P = 0.0042) only. TM-IFN-β mRNA expression was significantly lower in glaucoma patients with poor IOP control compared with those with good IOP control by IOP-lowering medications.
Conclusion:
Lower IFN-β in AqH and TM of patients with glaucoma and its association with clinical indices suggests its neuroprotective and antifibrotic role in glaucoma. The findings highlight the potential for IFN-β-based prognostication and therapy in the management of glaucoma.
Introduction
Glaucoma is an optic nerve degenerative condition that contributes to irreversible blindness. It is one among the top three causes of blindness in those aged 50 years and older.1,2 With an increase in aging population worldwide, glaucoma will continue to remain as one of the major causes of vision impairment with over 110 million expected to be affected by 2040.3,4 Hence, more efforts are being directed toward its prevention and treatment. Glaucoma is caused by retinal ganglion cell (RGC) degeneration, predominantly as a consequence of the sustained increase in intraocular pressure (IOP) due to disruption in the aqueous outflow pathways. 5 Primary glaucoma refers to glaucoma type where no underlying cause can be attributed to aqueous flow dynamics disruption and RGC degeneration, whereas in secondary glaucoma, the elevated IOP and RGC degeneration are often attributed to another ocular condition or injury. Patients with primary glaucoma have been categorized as those with open-angle glaucoma (POAG) or angle-closure glaucoma (PACG) based on the nature of disruption of the aqueous outflow mechanism. 5 Justly, elevated IOP is currently the only clinically modifiable factor that is being successfully treated in the management of glaucoma. 6 Strategies to lower the elevated IOP include the use of topical IOP-lowering medications (e.g., prostaglandin analogues, beta-blockers, alpha agonists, carbonic anhydrase inhibitors, Rho kinase inhibitors) and/or surgery (e.g., trabeculoplasty, trabeculectomy, trabeculotomy, goniotomy, iridotomy, minimally invasive glaucoma surgeries, glaucoma shunts). 7 However, disease progression despite good IOP control and failure of treatments to lower IOP were observed in a subset (up to 45%) of patients with glaucoma.8–18 This calls attention to the need to identify additional factors/mechanisms that influence RGC survival and trabecular meshwork (TM) response.
Continued decrease in visual function in patients with glaucoma with normal or low IOP suggests increased susceptibility to RGC death. Management strategies to improve RGC survival or visual function in addition to lowering IOP are being explored to reduce progression rate and disease burden. 19 The strategies in various stages of clinical trials include the use of alpha2-adrenergic agonist (brimonidine tartrate), nicotinamide, citicoline, memantine, neurotrophic factors (ciliary neurotrophic factor, nerve growth factor, brain-derived neurotrophic factor, glial cell-derived neurotrophic factor, hepatocyte growth factor, erythropoietin), reactive oxygen species scavengers/antioxidants, and anti-inflammatory agents.19–22 These approaches improve RCG survival by modulating apoptosis and adaption to oxidative stress, excitotoxicity, neurotrophins deprivation, and inflammatory stress.19–22 Failure of surgery and topical medications to lower and sustain IOP within the normal levels are often associated with aberrant pore closure or fibrotic response at the TM or abnormal wound healing at surgical sites. This has led to intraoperative and/or postoperative use of antifibrotic agents such as mitomycin C, 5-fluorouracil, and anti-Vascular Endothelial Growth Factor A to reduce failure rates following IOP-lowering surgical procedures. 23 In addition, the combined use of prostaglandin analogue and beta-blocker was shown to reduce pro-fibrotic factors and induce antifibrotic factor expressions in TM. 24 To further the ongoing effort to improve glaucoma therapeutics, it would be beneficial to identify endogenous factors with both neuroprotective and antifibrotic activity that are currently being harnessed for therapeutic benefits in clinics.
Interferon beta (IFN-β) is a pleiotropic cytokine and is one of the type I interferons that renders antiviral, antiproliferative, and immunomodulatory functions.25,26 In addition, IFN-β is also known for its neuroprotective27–29 and antifibrotic30,31 roles. Due to its pleiotropic nature, the status of endogenous IFN-β has been investigated in patients with dry eye disease, 32 keratoconus, 33 diabetic retinopathy, 34 and geographic atrophy. 35 While neuroprotective and antifibrotic role of IFN-β has been explored in other nonocular conditions, its role and expression status in patients with glaucoma is yet to be investigated. Since glaucoma pathogenesis includes degeneration of RGC and fibrotic changes of the TM, the current study investigated the status of IFN-β in aqueous humor (AqH) and TM of patients with primary glaucoma. The current study also investigated the relationship between intraocular IFN-β and clinical parameters that are indicative of degenerative and fibrotic changes in the RGC and TM, respectively.
Methods
Study cohort
The cross-sectional study was approved by the Institutional Ethics Committee. The study subjects were recruited, and sample collection was performed following informed consent as per institutional guidelines and as per the tenets of the Declaration of Helsinki. The study includes the collection of AqH or TM samples from patients with primary glaucoma. Glaucoma diagnosis was in accordance with the International Society of Geographical and Epidemiological Ophthalmology’s glaucoma classification working group guidelines. 36 Briefly, all study subjects underwent comprehensive clinical eye examination that include visual acuity assessment with refraction, IOP measurement, slit lamp evaluation, gonioscopy, fundus evaluation, and detailed optic nerve examination, including determination of vertical cup disc ratio. The evaluation includes determination of visual field index/status (VFI) using Humphrey field analyzer (Zeiss Humphrey systems, Dublin, CA) and/or retinal nerve fiber layer thickness (RNFLT) using RTVue-100 (Optovue Inc., Fremont, CA). AqH samples were collected from age-matched patients with primary glaucoma (n = 104, 107 eyes) undergoing cataract surgery and/or trabeculectomy and nonglaucomatous control subjects (n = 69, 70 eyes). Nonglaucomatous control subjects were those without glaucoma or any other retinal condition and were undergoing cataract surgery. Primary glaucoma subjects include patients with POAG (n = 58, 59 eyes) or PACG (n = 46, 48 eyes). In addition, TM from another cohort of age-matched patients with POAG (n = 19, 20 eyes) and PACG (n = 17, 18 eyes) were also collected during trabeculectomy. The clinical characteristics of study subjects are provided in Table 1. All the surgical procedures were performed as part of the preferred practice pattern, and the samples were collected without deviation from standard of care. Inclusion criteria were as follows: patients with primary forms of glaucoma (POAG and PACG) undergoing cataract surgery and/or trabeculectomy with a history of first-line IOP-lowering medications prior to the surgery. Exclusion criteria were as follows: patients with secondary glaucoma; primary glaucoma other than POAG and PACG; those with or history of other underlying retinal conditions; TM tissue with poor RNA yield; subject with age <18 years; subjects with seropositivity for Human Immunodeficiency Virus or Hepatitis B surface antigen or Hepatitis C virus or similar infectious conditions and autoimmune conditions; patients not on IOP-lowering medications or used it for less than a week prior to surgery; patients using IOP-lowering medications other than prostaglandin or beta-blockers, for example, alpha agonist, carbonic anhydrase inhibitors or cholinergic agonists only; and subjects without informed consent.
Study Cohort Characteristics
Data are shown as median (range).
Ordinary one-way ANOVA or Kruskal–Wallis test that compares controls, POAG, and PACG.
Statistical analysis performed between POAG and PACG only.
Indicates Mann–Whitney test.
Indicates unpaired t-test with Welch’s correction.
ANOVA, analysis of variance; IOP, intraocular pressure; MD, mean deviation; na, not applicable; ns, not statistically significant; PSD, pattern standard deviation; PACG, primary angle-closure glaucoma; POAG, primary open-angle glaucoma; RNFLT, retinal nerve fiber layer thickness; vCDR, vertical cup disc ratio; VFI, visual field index.
AqH and TM collection
AqH was collected from nonglaucomatous control subjects and patients with primary glaucoma via anterior chamber paracentesis during cataract surgery and/or trabeculectomy. Briefly, up to 50 μL of AqH was collected by inserting a syringe with 30-gauge needle through the peripheral cornea. The collected AqH samples were stored in sterile microcentrifuge tubes at −80°C till further processing. TM samples were collected while performing TM block excision during trabeculectomy, and iris was also collected while performing iridectomy. The TM tissue samples were collected in sterile microcentrifuge tubes containing Ringer’s lactate solution and stored at −80°C till further processing.
Measurement of IFN-β in AqH
The levels of IFN-β in the AqH were measured by bead-based ELISA (LEGENDplex™; Biolegend Inc.) as per the manufacturer’s instructions using a flow cytometer. Briefly, a flow cytometer (BD FACSCanto™ II; BD Biosciences) with BD FACSDiva software (BD Biosciences) was used to acquire the beads and record signal intensities following incubation of the samples with fluorescent capture beads conjugated with primary antibodies and subsequently with detection antibodies and PE-conjugated streptavidin. Absolute concentrations were determined from analyte-specific standards by using recommended analytical software (LEGENDplex Data Analysis Software Suite; Biolegend Inc.).
Measurement of IFN-β in TM
The status of IFN-β in the TM was assessed by measuring its messenger RNA (mRNA) status by quantitative PCR. Total RNA isolation from the collected TM and iris was performed using TRIZOL method according to the manufacturer’s protocol (Invitrogen). Following the assessment of RNA concentration and quality, the RNA for each sample was converted to complementary DNA (cDNA) using Bio-Rad iSCRIPT cDNA conversion kit (Bio-Rad). The quantitative real-time PCR cycle using SYBR green reagent (Kapa Biosystems Inc.) was performed on the CFX Connect™ real-time PCR detection system (Bio-Rad). The expression of IFN-β was determined by normalizing its expression to a housekeeping gene, β-actin, in the respective samples.
Statistical analysis
The distribution status of the data was determined by Shapiro–Wilk normality test. The differences in the study parameters including IFN-β levels or expression between the groups were statistically analyzed by either Mann–Whitney, one-way analysis of variance, or Kruskal–Wallis test with Dunn’s multiple comparison test. Spearman’s rank correlation was performed to determine the association between IFN-β and clinical parameters. Receiver operating characteristic (ROC) curve analysis to determine the area under the ROC curve (AUC), sensitivity, specificity, and odds ratio (OR) was performed. The optimal cutoff criterion (which maximizes the sensitivity and specificity) that was used for OR calculation was determined using ROC curve analysis. A P value <0.05 was statistically significant. Statistical analyses were performed with either GraphPad Prism 10.4.1 (GraphPad Software, Inc.) or MedCalc® Version 12.5 (MedCalc Software bvba).
Results
IFN-β levels in the AqH patients with primary glaucoma
The AqH levels of IFN-β were significantly lower in patients with primary glaucoma (median = 26.4; range = 1.7–2204) compared with nonglaucomatous controls (62.5; 9.7–347.2) as shown in Fig. 1a. Furthermore, the AqH-IFN-β levels in patients with POAG (21.8; 1.7–2206) were significantly lower compared with nonglaucomatous controls (Fig. 1b), whereas the AqH-IFN-β levels in patients with PACG (71.2; 2.4–1055) were not significantly different compared with controls (Fig. 1b). The AqH-IFN-β levels in patients with POAG were significantly lower compared with AqH-IFN-β levels in patients with PACG (Fig. 1b). ROC curve analysis was performed to determine the AUC, which would suggest the clinical importance and relevance of AqH-IFN-β levels in POAG pathobiology. The largest AUC observed for AqH-IFN-β levels while comparing POAG and nonglaucomatous controls was AUC = 0.723 with P < 0.001 (Fig. 2a). The cutoff value of ≤35 pg/mL of AqH-IFN-β was determined using the Youden index criterion in ROC curve analysis, showed 70% sensitivity, 70% specificity, and an OR of 5.3 [95% confidence interval (CI) 2.5–11.2, P < 0.0001] as shown in Fig. 2b.
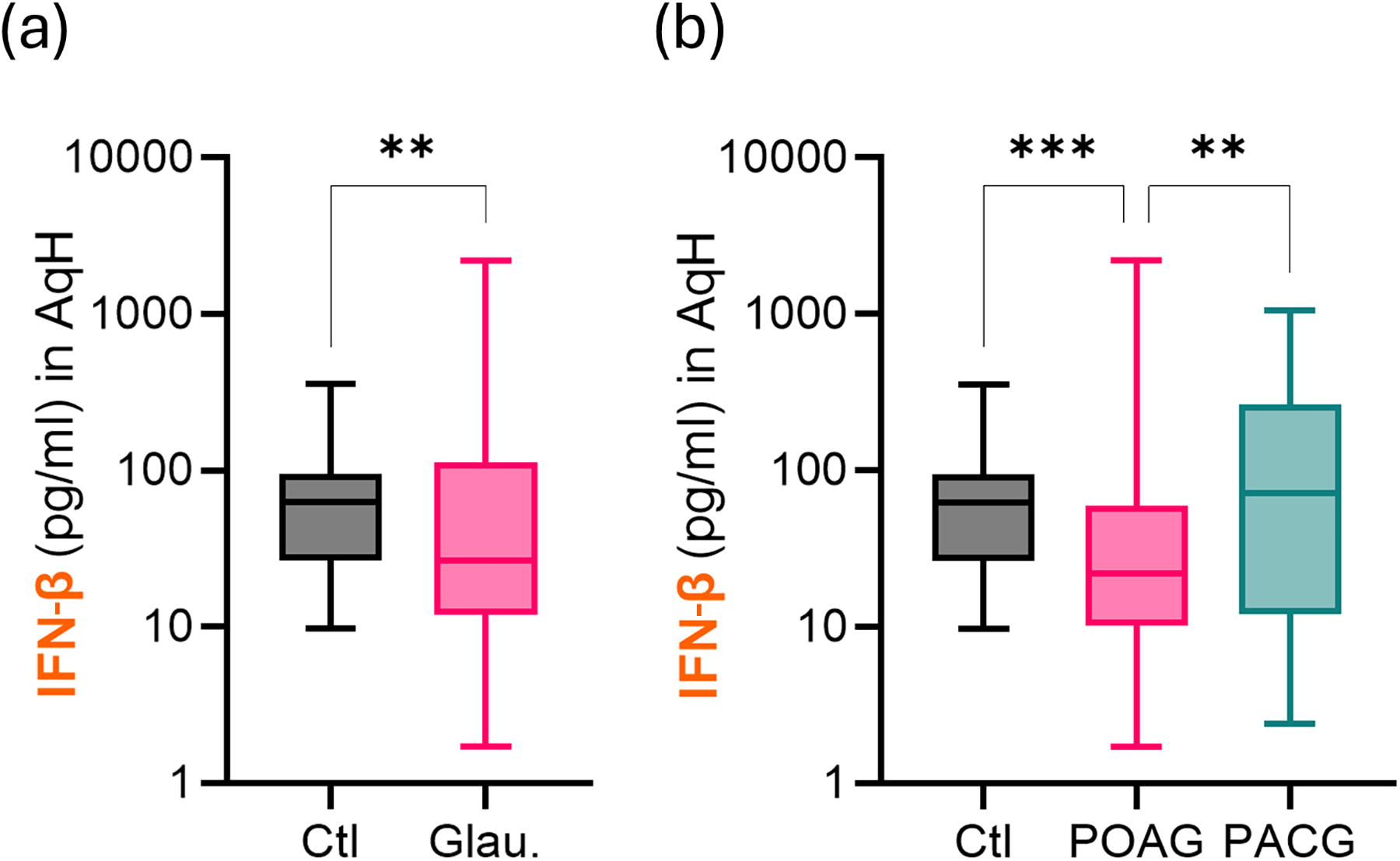
Levels of IFN-β in the aqueous humor of patients with primary glaucoma. Graphs indicate the concentration of aqueous humor IFN-β levels in (
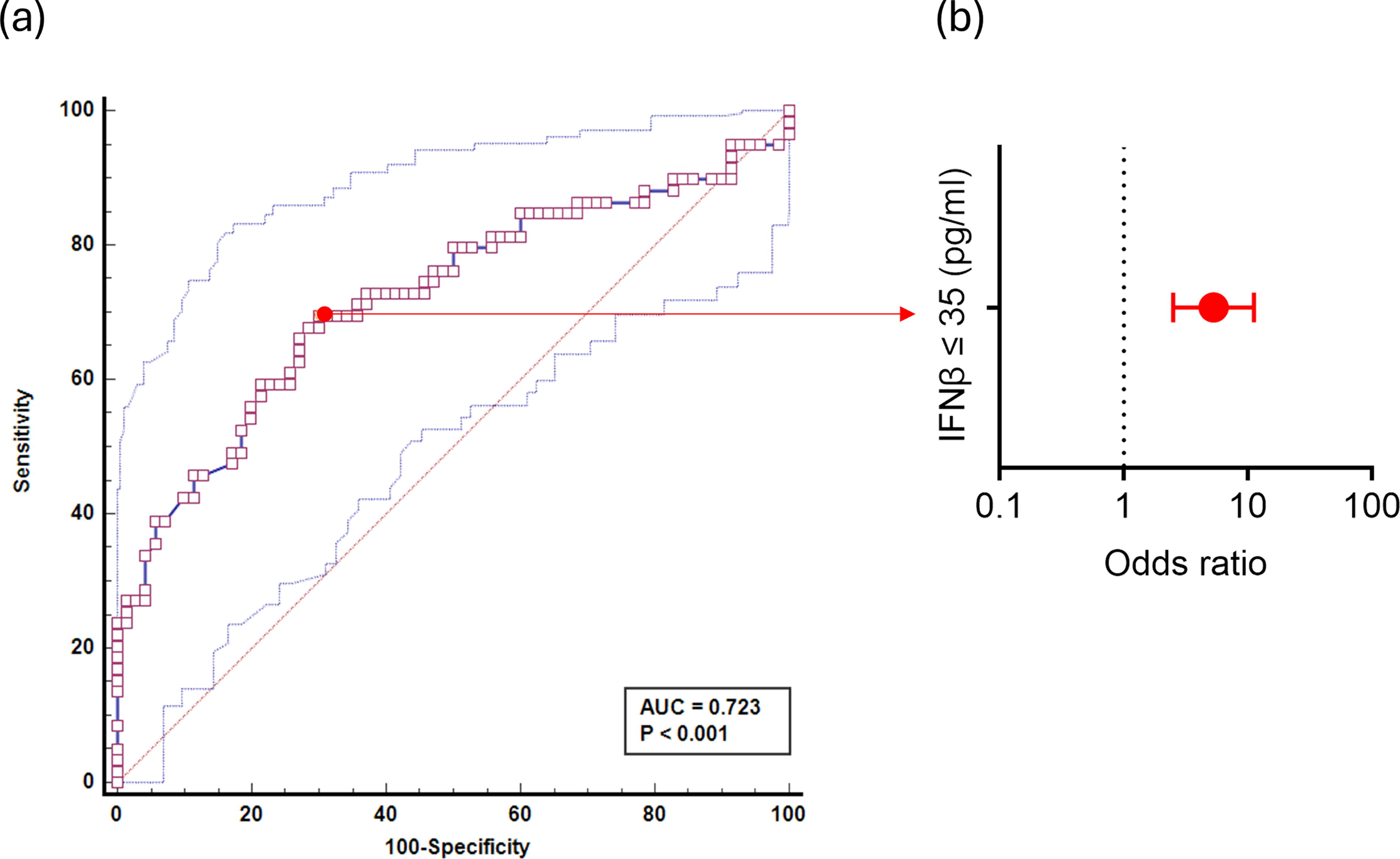
Strength of relationship between aqueous humor IFN-β levels and primary open-angle glaucoma. Graphs indicate (
Association between AqH-IFN-β levels with clinical parameters of primary glaucoma patients
The levels of AqH-IFN-β were positively correlated with VFI of patients with primary glaucoma (Table 2) and negatively correlated with pattern standard deviation (PSD) of patients with primary glaucoma (Table 2). The levels of AqH-IFN-β were positively correlated with VFI and RNFLT of patients with POAG (Table 2) and negatively correlated with PSD of patients with POAG (Table 2). However, the levels of AqH-IFN-β were correlated (positively) only with VFI of patients with PACG (Table 2). These observations suggest a potential neuroprotective or disease protective role of IFN-β in glaucoma.
Association Between Interferon Beta Levels in Aqueous Humor and Clinical Parameters
IOP, intraocular pressure (n = 107 eyes); PSD, pattern standard deviation (n = 88); PACG, primary angle-closure glaucoma; POAG, primary open-angle glaucoma; RNFLT, retinal nerve fiber layer thickness (n = 63 eyes); r, Spearman’s rank correlation coefficient; vCDR, vertical cup disc ratio (n = 62 eyes); VFI, visual field index (n = 88 eyes).
Relationship of IFN-β expression in the TM of patients with primary glaucoma with response to IOP-lowering medication and severity of the disease
Since IFN-β is known for its antifibrotic potential, we investigated its gene expression status in the TM of primary glaucoma patients with varying responses to IOP-lowering medications. The response to IOP-lowering medications can be attributed to the pore status of the TM. The patients were categorized either as responders or nonresponders to IOP-lowering medications based on the success in maintaining normal IOP following the use of medications. To determine the expression status of IFN-β specifically in the TM, the gene expression of IFN-β in TM tissue was normalized to the gene expression of IFN-β of the respective iris tissue (TM/iris ratio) for each patient sample. The tissue normalized expression of IFN-β in TM was observed to be significantly lower in patients with primary glaucoma with poor IOP control (nonresponders) compared with those patients with good IOP control (responders) as shown in Fig. 3a. The expression of IFN-β was markedly lower in the TM of nonresponders compared with responders; however, no differences were observed in the expression of IFN-β in the iris of nonresponders and responders (Supplementary Fig. S1). These observations suggest a potential antifibrotic role of IFN-β in the TM of patients with glaucoma.
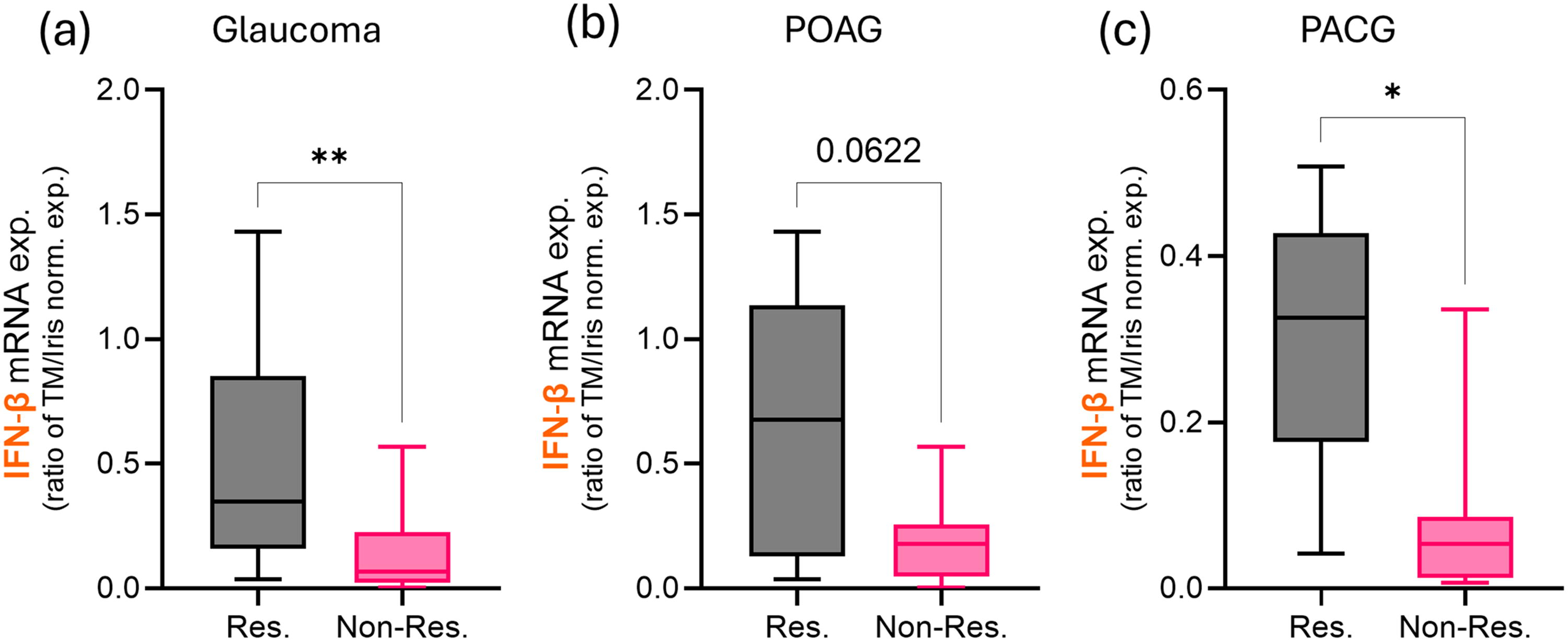
mRNA expression of IFN-β in the trabecular meshwork (TM) of patients with primary glaucoma grouped based on response to intraocular pressure-lowering medications. Graphs indicate mRNA expression of IFN-β in TM normalized to respective iris sample as TM/iris ratio in patients with (
We investigated the relationship between IFN-β gene expression status in the TM and the severity of disease in patients with primary glaucoma. The patients were categorized as nonsevere and severe based on the VFI score. VFI >40 was considered as nonsevere, and VFI <40 was considered as severe. We observed a significant decrease in the tissue normalized expression of IFN-β in the TM of patients POAG with severe form of the disease compared with those with nonsevere form of the disease (Fig. 4). The expression of IFN-β was significantly lower in the TM of patients POAG with severe form of the disease compared with those with nonsevere form of the disease; however, no differences were observed in the expression of IFN-β in the iris of patients POAG with severe form of the disease compared with those with nonsevere form of the disease (Supplementary Fig. S2). Overall, the observations indicate the homeostatic regulatory and protective role of intraocular IFN-β in patients with primary glaucoma.
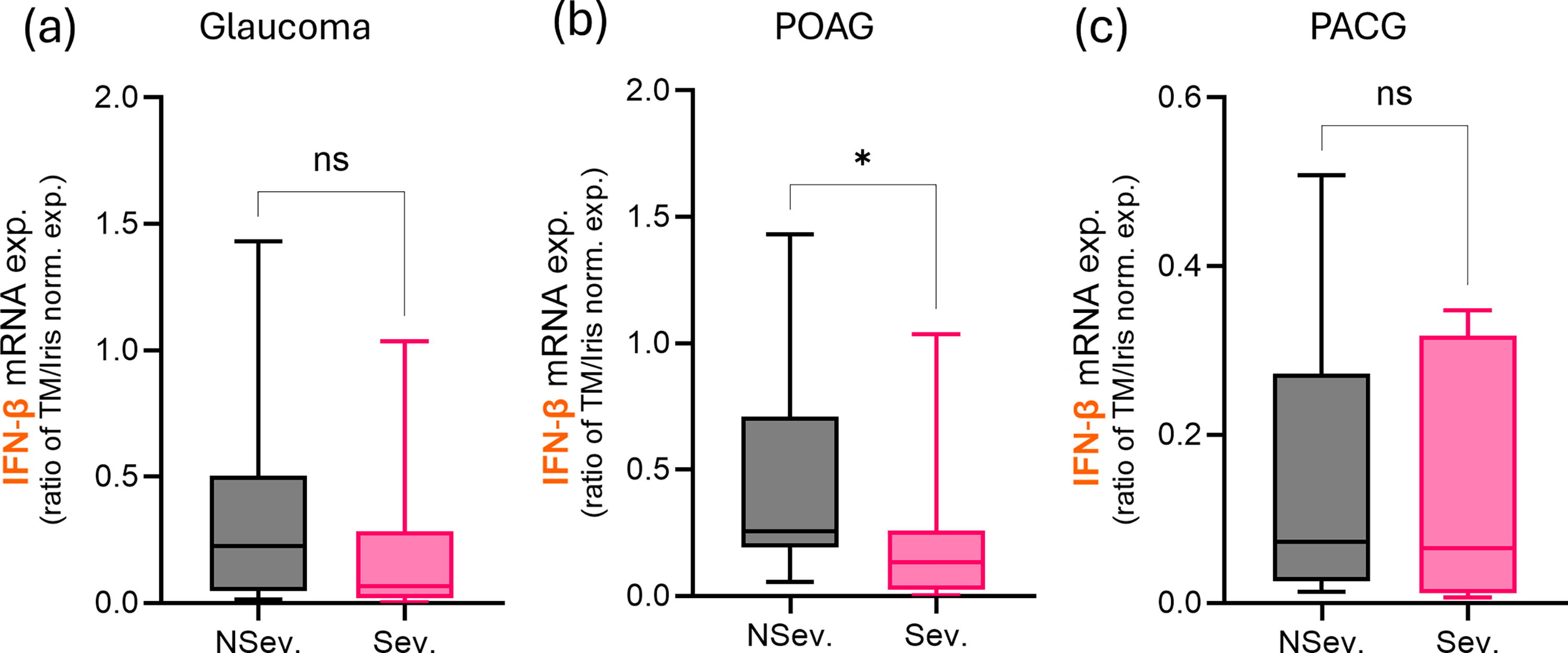
mRNA expression of IFN-β in the trabecular meshwork (TM) of patients with primary glaucoma grouped based on severity of the disease. Graphs indicate mRNA expression of IFN-β in TM normalized to respective iris sample as TM/iris ratio in patients with (
Discussion
Identification of strategies and newer targets to reduce the frequency of disease progression and failure to lower IOP has been an area of intense research to address the unmet clinical need in the management of glaucoma. Enhancing neuroprotection would reduce the rate of disease progression in patients with normal or well-controlled IOP. Several studies have demonstrated the neuroprotective potential of IFN-β in both animal models and patients with multiple sclerosis.27,28,37–39 Studies indicate that IFN-β renders its neuroprotection by suppressing activated microglia-induced neurotoxicity,27,40 immune dampening,40,41 induction of neurotrophic factors, 42 and reduction of reactive oxygen species levels. 43 Transcriptomic profiling in patients with multiple sclerosis after the injection of IFN-β shows induction of genes involved in the protective integrated stress response, synaptic transmission, nerve cell survival, and immunoregulation. 44 Though patients with multiple sclerosis did not have an increased risk for glaucoma, 45 IFN-β treatment was reported to reduce RNFLT loss in these patients compared with those without treatment. 46 Intramuscular IFN-β was reported to be superior than subcutaneous IFN-β in reducing ganglion cell inner plexiform layer thinning in patients with multiple sclerosis. 47 Other studies48–50 which reported on the effect of IFN-β in ganglion cell inner plexiform layer thinning in patients with multiple sclerosis cannot be relied upon as these studies did not subdivide the patients on IFN-β based on its route of administration as those receiving intramuscular or subcutaneous IFN-β. Our current study supports these observations by reporting significantly lower AqH-IFN-β levels in patients with POAG and demonstrating a positive relationship of AqH-IFN-β levels with VFI and RNFLT in these patients. These findings suggest the relevance of IFN-β in the protection of RGCs in glaucoma.
Restoration of IOP to normal levels and its sustenance remains elusive for a subset of patients despite switching/addition of IOP-lowering medications and use of antifibrotic agents alongside IOP-lowering surgical procedures. Paucity in endogenous regulation of pro-fibrotic response at the surgical site and TM may underlie these failures. Transforming growth factor beta (TGF-β) known for its role in the TM-associated fibrosis is elevated in patients with glaucoma,51–53 and other studies have shown that TGF-β inhibits the induction of IFN-β, a factor with known antifibrotic potential.54,55 IFN-β reduces injury-induced fibrosis in lungs, liver, and cardiac tissue models,30,31,56–58 and it renders its antifibrotic role by modulating TGF-β1, Basic fibroblast growth factor, Collagen 1A2, signal transducer and activator of transcription 1, and signal transducer and activator of transcription 2.30,31,56–58 IFN-β inhibits Th17 differentiation, 41 and Th17 is known for its role in the pathogenesis of fibrosis.59–61 Hence, IFN-β may also render its antifibrotic process indirectly by inhibiting Th17/IL-17 axis. More recently, IFN-β was reported to reduce pro-fibrotic factors, including Connective Tissue Growth Factor (CTGF), alpha smooth muscle actin (αSMA), and myocilin expression in the TM cells. 62 This is in accordance with the observations in the current study where the mRNA expression of IFN-β was significantly lower in the TM of nonresponders to IOP-lowering medications compared with patients who responded favorably to IOP-lowering medications. This suggests the relevance of a beneficial role of IFN-β in aqueous outflow regulation. However, a study that reported IOP increase following anterior chamber injection of IFN-β in mice was due to autophagy-associated dysfunction of TM 62 and did not use relevant controls, such as protein equivalent or dominant negative version of IFN-β, to attribute the increase in IOP exclusively to the biological action of IFN-β. Overall, the current evidence points toward the potential antifibrotic benefits of the use of IFN-β in the context of glaucoma.
A recent study has demonstrated an exaggerated cGAS–STING (2', 3'-cyclic GMP-AMP-Synthase - Stimulator of Interferon Genes) signaling in microglial cells to be a critical contributor in glaucoma pathogenesis, including the apoptosis of RGC in an animal model. 63 Furthermore, the study also shows that blockade of receptor-Interferon alpha/beta receptor 1 prevented glaucoma-induced losses of RGCs. 63 This implicates the role of type I IFNs in glaucoma pathogenesis as type I IFNs signal through heterodimeric receptors—IFNAR1 and IFNAR2. IFN-β belongs to a family of type I IFNs, which includes IFN-α (12 types), IFN-ε, IFN-ω, IFN-κ, IFN-δ, IFN-τ, and IFN-ζ, in addition to IFN-β. 64 Many studies that investigate the relevance of type I IFNs in various disease contexts failed to delineate the relevance or specificity of the species of type I IFNs involved in the responses. This is critical because several studies have demonstrated that IFN-α and IFN-β evoke similar and diverse biological responses, at times counter-regulate each other’s expression, despite the relative structural similarity and the use of identical receptors for mediating their actions.26,64 This dichotomy within the type I IFNs can be seen in patients as well, with IFN-α being more effective than IFN-β in the treatment of viral infections and IFN-β in the treatment of autoimmune diseases, such as multiple sclerosis, and the use of IFN-α over IFN-β in the management of ocular surface squamous neoplasia and conjunctival melanoma.65,66 One of the unique biological responses of IFN-β is its ability to render immune dampening by inducing a potent anti-inflammatory cytokine, IL-10, and immune checkpoint factor, Programmed Cell Death Ligand 1,67–70 which is attributed toward the various protective roles of IFN-β, including that seen in patients. A study that reported the immunomodulatory role of IFN-β over IFN-α in an animal model showed an increase in the levels of IFN-β following IFNAR1 receptor blockade, 67 emphasizing the preferential immunomodulatory role of IFN-β over IFN-α. In addition, IFN-β was more potent than IFN-α in reducing the expression of pro-fibrotic factors, including CTGF and αSMA, in TM cells. 62 These observations invite the need to study the status and selective blockade of key type I IFNs, including IFN-α and IFN-β, in glaucoma models, to determine the dichotomy in disease causality and protection by these type I IFNs.
In vitro and in vivo disease modeling highlights the immunomodulatory and potential therapeutic role of IFN-β in various ocular conditions. Studies have shown that administration of subcutaneous IFN-β has alleviated experimental autoimmune uveitis along with a reduction in the relevant inflammatory cytokines.71,72 IFN-β levels were associated with increased cell viability and anti-inflammatory effects in herpes simplex virus type 1-infected corneal keratocytes. 73 IFN-β also resulted in inhibition of Intercellular Adhesion Molecule 1 and CXCL9 production in retinal pigment epithelium (RPE) cells 74 and improved its proliferation after laser photocoagulation in animals. 75 Though the levels of IFN-β were reported to be increased in streptozotocin-induced diabetic rats and in aqueous and vitreous humor of patients with diabetic retinopathy,34,76 its relevance in the pathogenesis of diabetic retinopathy remains to be determined. The levels of IFN-β were reported to be significantly lower in the serum and retina of laser-induced choroidal neovascularization animal model, 77 and supplementation of IFN-β was shown to reduce chronic inflammation and pathological angiogenesis in this model.77,78 However, despite its ability to reduce activated microglia, IFN-β failed to prevent light-induced retinal degeneration—a model claimed to mimic dry AMD, 79 which is in line with a study that implicated IFN-β in RPE degeneration via a noncanonical-inflammasome pathway in a geographic atrophy model. 35 Adeno-associated virus-based intravitreal injection of IFN-β exhibited a potent antitumor effect in in vivo retinoblastoma model. 80 The observations from these studies emphasize the disease-specific, route of administration-specific, and dose-specific therapeutic benefit of IFN-β in ocular conditions.
Conclusion
Intraocular endogenous IFN-b was signficantly reduced in patients with primary glaucoma. The association of intraocular endogenous IFN-β with clinical parameters suggests its neuroprotective and antifibrotic role. With IFN-β being an approved drug with a known safety record for over two decades, observations from the current study and others open avenues for IFN-β supplementation or augmentation as a new indication in the management of glaucoma. However, a more detailed preclinical study is required to determine the optimal dose and regimen to restore RGC survival and aqueous outflow for improving the clinical outcome in patients with glaucoma.
Footnotes
Authors’ Contributions
A.P.N.: Investigation, formal analysis, validation, visualization, and writing—original draft. P.M.: Investigation and formal analysis. S.T.: Resources and data curation. S.D.: Resources and data curation. S.D.A.V.: Resources and data curation. N.S.: Resources and data curation. R.S.: Resources and data curation. A.G.: Conceptualization, methodology, writing—review and editing, project administration, and funding acquisition. S.S.: Conceptualization, methodology, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
The authors have no financial disclosures or conflicts of interest to declare pertaining to the study.
Funding Information
The study was funded by Narayana Netralaya Foundation, Bangalore, India. The funding organization had no role in the design or conduct of this research.