
Abstract
Purpose:
To assess and describe young women's experiences with their first dose of quadrivalent human papillomavirus vaccine (HPV4) (Gardasil®) in a large managed care organization.
Methods:
We collected survey and electronic medical record (EMR) data for 899 young women aged 11–26 receiving their first HPV4 injection from February through September 2008. Survey items included questions about adverse events, interactions with healthcare providers, and knowledge and attitudes toward HPV disease and HPV4.
Results:
Six hundred ninety-six (78%) participants reported pain at the injection site. Other common reactions included injection site bruising or discoloration (n=155, 17%) or swelling (n=127, 14%) and presyncope or syncope (n=134, 15%). Overall, preteens and teens were more likely than adult participants to report vaccine adverse events. Most respondents, particularly in the adult age group, reported that their healthcare provider reviewed important information about HPV infection and about the risks and benefits of receiving the vaccine. Knowledge and attitudes about HPV and HPV4 also varied by age, with older women generally exhibiting more accurate knowledge about HPV and perceived susceptibility to cervical cancer.
Conclusions:
There were significant age differences in young women's experiences with their first HPV4 injection. These findings highlight the importance of age-appropriate education and provider communications about HPV disease and vaccination.
Introduction
In June 2006,
Surveys of young women conducted before and shortly after HPV4 licensure have shown that most young women have favorable attitudes toward the vaccine and would consider being vaccinated. 5 –11 Uptake of HPV4 has been less than expected in the United States, however, with reported initiation rates ranging from 9% to 44%, depending on age. 12 –16 Although most young women are generally aware of HPV disease and the availability of the vaccine, their knowledge about virus transmission, screening recommendations and practices, and treatment is less reliable. 6,11,17 –21 Knowledge about and attitudes toward HPV vaccine vary by race and ethnicity, education, and socioeconomic status (SES), 6,10,17,22 –28 with lower rates of knowledge among the less educated and among nonwhites. 21,22,24,26 Commonly reported barriers to receiving HPV4 include cost and concerns about vaccine safety. 25 –30
We currently have limited information about young women's adverse event experiences with HPV4 aside from the data collected in the prelicensure clinical trials and reports to the Vaccine Adverse Event Reporting System (VAERS). Clinical trials have demonstrated that HPV4 is highly effective in preventing infection with the HPV types included in the vaccine. 31 The primary adverse events reported during these trials included injection site pain, fever, nausea, and dizziness and syncope. 32 An analysis of case reports from VAERS also found pain, nausea, and dizziness/syncope to be the most frequently reported adverse events after HPV4. 33
Our goal was to assess and describe young women's experiences with their first HPV4 dose in a large managed care organization, using electronic medical record (EMR) and survey data. We gathered data related to reported adverse events, interactions between the young women and their healthcare providers, and knowledge and attitudes toward HPV disease and HPV4 vaccine. Such information could be used to design or focus interventions to improve HPV4 uptake and compliance with the three-dose HPV4 series and might identify opportunities for improved provider communication and education of vaccine recipients. Our study is one of a few that is based on data from vaccine recipients rather than on data from potential vaccinees or their parents. Our study is also one of the few to report data about adverse events following HPV4 injection.
Materials and Methods
Kaiser Permanente Northwest (KPNW) is a large managed care organization serving about 56,000 young women 11–26 years of age in northwest Oregon and southwest Washington. KPNW has comprehensive EMR databases that contain information about member demographics, insurance coverage, diagnoses, and vaccinations. The health plan provides vaccines, including HPV4, to members who choose to receive them at no additional out-of-pocket cost.
We identified all female KPNW members aged 11–26 years who received their first HPV4 dose in February through September 2008. Within 1 week of their vaccination, we initiated a series of recruitment mailings and follow-up telephone calls to vaccinees inviting them to complete a survey about their experiences with HPV vaccine. For minors <18 years old, we first sent an invitation letter describing the survey to their parents or guardians, giving them an opportunity to decline participation for their daughter. Participants had the option of completing the survey on paper or on a secured website. Survey respondents were entered into monthly raffle drawings to receive a $100 gift certificate.
Our 50-item survey included questions about adverse reactions to HPV4, interactions with the provider and health plan, potential barriers or challenges to vaccination, and general knowledge and attitudes about HPV vaccine and disease. Survey response options included a mixture of forced-choice, multiple choice, and Likert-scale items and included questions about vaccine knowledge, attitudes, and beliefs that were similar to questions used in other HPV vaccine studies. 5,11,13,17 –20 Copies of the survey text are available from the authors by request.
To supplement our survey data, we extracted the following EMR information: race and ethnicity, insurance coverage, geocoded Census tract of residence, and vaccination history. We also extracted information about medically attended local reactions and dizziness and syncope to compare with survey responses. A complete list of ICD-9 codes is available from the authors by request. We identified local reaction diagnosis codes that indicated events occurring within 7 days of the vaccination and syncope/dizziness diagnosis codes within 2 days of the vaccination. To improve the specificity of these coded vaccine adverse events, we excluded persons with local reaction or syncope diagnoses in the 30 days before vaccination. In addition to Medicaid enrollment history, we estimated SES using the Diez-Roux Index, which is a commonly used measure of neighborhood SES associated with health outcomes. 34 Using Census data, Diez-Roux et al. created composite summary scores representing neighborhood wealth and income, education, and occupation. We obtained Diez-Roux scores for the Census tracts in the KPNW service area and then divided the scores into quintiles (lowest SES, lower SES, middle SES, higher SES, and highest SES). We then assigned each individual participant to the SES quintile of their geocoded residential address.
We describe survey responses by age at vaccination (11–12, 13–17, or 18–26 years). If the survey was returned to us without any response, we classified the participant as nonresponsive and excluded her from analysis. Missing data for individual survey items were infrequent (generally <2%) and were excluded from chi-square comparisons of responses across age categories. To describe potential selection bias, we used data from our EMR to compare survey respondents and nonrespondents by age, race and ethnicity, SES, and frequency of EMR-recorded vaccine adverse events. We also report the percent agreement between survey-reported and EMR-coded local reactions and dizziness/syncope. We used logistic regression to compare adverse events between those who received HPV4 alone and those who received multiple concomitant vaccinations.
The KPNW Institutional Review Board reviewed and approved the study protocol and survey instrument.
Results
Between February and September 2008, 3490 young women 11–26 years of age received HPV4 at KPNW and were invited to participate in the survey (Fig. 1). Four percent of our recruitment mailings were returned as undeliverable, and 9 parents refused participation on behalf of their daughters before receiving our survey materials. Of the 3347 young women who received our materials, 899 (27%) completed the survey. Thirty-four percent completed the survey on the Internet; the rest completed paper-based surveys.
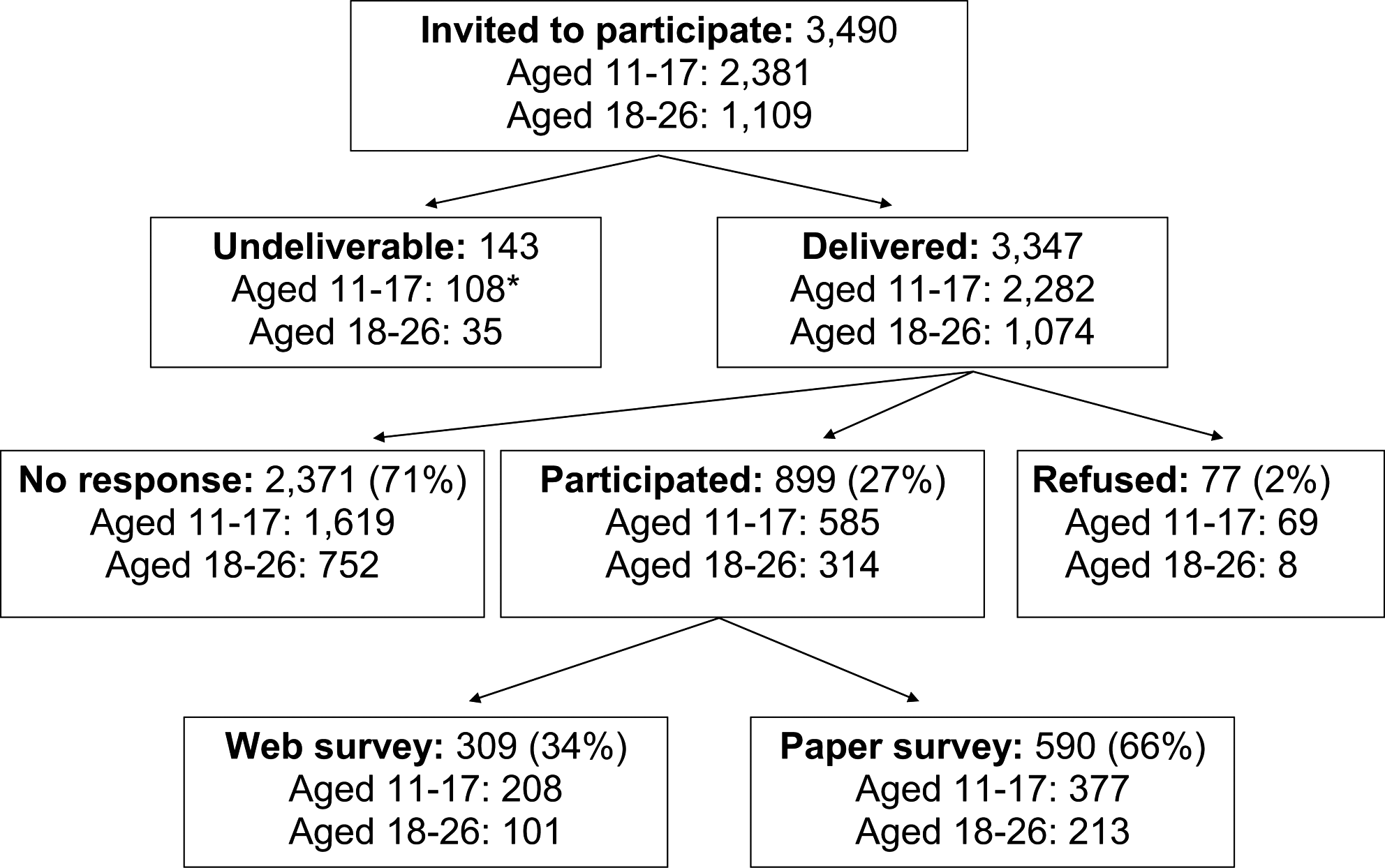
Participation rates in human papillomavirus (HPV) vaccine survey of young women 11–26 years of age. *Includes 9 parents who refused participation for their daughters before receiving survey materials.
When we compared survey respondents and nonrespondents, we observed several significant differences between the groups (Table 1). Adolescent females (13–17-year-olds) were less likely to participate in the survey than were preteens (11–12-year-olds) and adults (18–26-year-olds). Females of lower SES (measured either as SES of geocoded Census tract of residence or Medicaid status in the last year) were also less likely to participate. Race and ethnicity were unknown for more than half of the sample, but among those with available information, participation rates were higher in non-Hispanic whites compared to other ethnic and minority groups. Response rates were also higher among those who received HPV4 from an internal medicine or obstetrics/gynecology provider compared to those seen by a pediatrician or family practitioner, which likely reflects the older age distribution of our respondents. Respondents were more likely to have received HPV4 alone at the index encounter; nonrespondents were more likely to have received more than one vaccine at that encounter. We hypothesized that this relationship might have been confounded by age, but it was observed across all age strata (data not shown).
Diez-Roux Index scores represent a composite summary of neighborhood wealth and income, education, and occupation based on Census data. 34
Emergency room and missing encounters excluded from chi-square test.
EMR, electronic medical record; HPV, human papillomavirus; SES, socioeconomic status.
Seventy-eight percent of survey participants reported pain at the injection site; of those reporting pain, 11% said the pain was severe to very severe (Table 2). The proportion of respondents reporting pain and the reported intensity of pain decreased with age. One third of respondents said the vaccines they received at the index encounter hurt more than other vaccines received in the past.
Among those reporting any pain.
Seventeen percent of participants reported bruising or discoloration at the injection site, and 14% reported swelling. These reported local reactions were less common among the 18–26-year olds than among the preteens and teenagers. Forty (6%) of the 711 females who reported pain, bruising, or swelling had a related local reaction coded in the EMR. Among the 215 females who reported just swelling or bruising, 12 (6%) had a coded local reaction in the EMR.
Eight participants (1%) reported fainting (syncope) after their index vaccination, and 133 (15%) reported feeling lightheaded or dizzy (presyncope). Reported presyncope was most common in preteens and adolescents. Thirty-one percent of participants who fainted or felt lightheaded after vaccination reported that they told their provider how they were feeling. Of the 134 females who reported fainting or dizziness, only 2 (1%) had a dizziness or syncope code in the EMR. We reviewed the medical records of 13 participants with possible syncope, 7 who reported fainting in our survey, 5 who had a syncope diagnosis code in the EMR, and 1 who both reported syncope and had a syncope diagnosis code. Of the 7 females who reported syncope, 1 was confirmed through medical record review, 1 had symptoms of syncope noted but never lost consciousness, and 1 fainted 9 days after vaccination while at school. The 4 remaining reported syncope events were not confirmed by record review. All 5 of the females with a syncope diagnosis code in the EMR had chief complaints of dizziness or past syncope, and all received their HPV4 at the reference encounter with no adverse effects noted. The 1 participant who both reported syncope and had a syncope diagnosis code in the EMR fainted in the clinic waiting room, suffered a head contusion and loss of memory, and was transported to the emergency room for further evaluation and monitoring.
Adult females (60%) were more likely to receive HPV4 alone at their index encounter compared to adolescents (23%) and preteens (8%) (p<0.0001). HPV4 was most often coadministered with a tetanus booster (Td or Tdap), meningococcal conjugate vaccine, or hepatitis A vaccine. After adjusting for age, females who received HPV4 alone reported fewer adverse events than those who received HPV4 plus additional vaccine(s) at their index encounter. The age-adjusted odds ratios (OR) comparing those who received HPV4 alone to those who received multiple vaccines at the index encounter were 0.76 (95% confidence interval [CI] 0.53-1.08) for injection site pain, 0.51 (95% CI 0.33-0.80) for bruising, 0.45 (95% CI 0.27-0.75) for swelling, and 0.63 (95% CI 0.39-1.01) for dizziness.
Knowledge and beliefs about HPV and the vaccine varied across age groups, with older females generally having more accurate knowledge of HPV than younger females (Table 3). Most respondents knew that HPV can cause cervical cancer and that the HPV vaccine requires three doses. Respondents, especially those in the preteen group, were less aware of HPV symptoms and treatment and of its relationship to genital warts and abnormal Pap tests. Participant beliefs about susceptibility to cervical cancer also varied by age; 11% of preteens, 8% of teenagers, and 3% of adults strongly agreed or agreed they were too healthy to get cervical cancer. Similarly, 15% of preteens, 8% of teens, and 4% of adults strongly agreed or agreed they were too young to get cervical cancer. About 12% of participants reported a family history of cervical cancer. Participants with this family history were more likely to disagree that they were too healthy (p=0.05) or too young (p=0.02) to get cervical cancer compared to those without a family history of cervical cancer.
Percent of participants providing the correct answer to these true/false statements.
Seventy-four percent of participants reported that they had seen an advertisement for HPV vaccine, and this percentage increased with age. About half of participants said they received HPV4 as part of a routine medical checkup; 19% said the primary reason for their visit was to be vaccinated against HPV (Table 4). Two thirds of participants said their provider talked with them about HPV infection, 76% said their provider discussed the benefits of the vaccine, 61% said their provider discussed the vaccine's potential side effects, 52% talked with their provider about cervical cancer, 20% talked with their provider about genital warts, and 29% discussed Pap tests with their provider. Older participants reported their providers were more likely to discuss these topics with them during their visit. In particular, adolescents and adults were more likely to report discussing genital warts and Pap tests with their providers than were pre-teens. Eighty-seven percent of participants said their provider talked with them about the need to return for additional doses of HPV4.
Clinical setting data from the electronic medical record, not participant report; one adult participant received HPV4 in the emergency room.
The ACIP currently recommends that HPV vaccine recipients be seated and monitored for signs of presyncope/syncope for 15 minutes after vaccination. 35 Twenty-four percent of preteens, 22% of teens, and 17% of adult survey respondents said their provider asked them to sit and rest after vaccination. Among those who reported dizziness after vaccination, 37% were told to rest by the provider compared to 18% of those who did not experience dizziness (p<0.0001).
We asked several questions about potential barriers to vaccination, such as transportation or scheduling difficulties and apprehension about vaccination. Overwhelmingly, survey respondents did not report such barriers (data not shown). Ninety-two percent of the 11–17-year-old respondents said their parent or guardian drove them to the clinic for their appointment. Almost half (45%) of the vaccinees reported they were worried or scared about getting a vaccine, and this fear decreased with age (64% of preteens, 50% of teens, 24% of adults, p<0.0001).
Discussion
Our study shows that age is an important factor influencing young women's experiences with the quadrivalent HPV vaccine. Age was associated with the likelihood of an adverse event, interaction with healthcare providers (including which topics related to cervical cancer providers discussed with their patients), and patient knowledge and beliefs about the vaccine. Younger girls were more likely than older females to report local reactions and presyncope after vaccination. They were also more likely to receive other vaccinations concomitantly, especially tetanus and meningococcal conjugate vaccines.
The frequency of injection site pain following HPV4 injection in our participants was consistent with data reported from the Gardasil prelicensure trials. Seventy-three percent of females in our study reported pain at the injection site following HPV4 alone, compared to 84% of 9–26-year-old females in the clinical trials. 36 Our participants reported less swelling (7% vs. 25%) but more dizziness (10% vs. 4%) after HPV4 alone than clinical trial participants. 32 Although dizziness is not a serious side effect by itself, it can lead to syncope if not properly managed. As we observed in our study, syncope can in turn lead to serious injuries, especially to the head.
To our knowledge, no population-based studies have reported rates of self-reported local reactions and presyncope following HPV4 with or without concomitant vaccinations. Our reported adverse event rates were generally higher in females who received additional vaccines at the index encounter, especially in younger girls. Very few of the adverse events self-reported in the survey responses were coded in our EMR. Providers might note these events in the text portion of the EMR but not assign ICD-9 codes to them. With the exception of syncope, we did not manually review medical records to collect additional information about these reported adverse events.
Our survey respondents were aware of the existence of HPV but were less knowledgeable about the specifics of HPV symptoms and treatment. The preteen girls, for whom the vaccine is specifically recommended, had the least knowledge and awareness of HPV and the vaccine of any age group. Knowledge and beliefs about HPV disease and vaccine in our population were generally consistent with those in other surveys. 5,11,13,17 –20 In a systematic review including 39 studies published before HPV4 licensure between 1992 and 2006, 8%–68% of study participants were aware that HPV causes cervical cancer, and 5%–83% of participants in these studies were aware that HPV causes genital warts. 19 In our survey, 70%–94% of respondents were aware that HPV causes cervical cancer, and 32%–68% were aware that it causes genital warts, depending on the age of the participant. Older participants generally had more awareness of the negative health consequences of HPV infection than did younger participants.
HPV4 is the first vaccine to be marketed directly to consumers. Most participants reported seeing a print or television advertisement for the vaccine, and this proportion increased with age. Our findings are consistent with two recent surveys that suggest HPV vaccine advertisements have reached a large segment of the age-eligible population. 14,36 However, the issue of direct marketing for HPV4 is complex because a significant segment of the recommended population for vaccine are minors, and, therefore, parental consent is required for vaccine administration. Thus, marketing efforts have also been targeted at parents in addition to young women. Several studies suggest most women and girls are, in addition to getting information about HPV from advertisements, getting HPV information from their parents, peers, and medical providers. 14,37 A provider recommendation is frequently cited as one of the strongest predictors of HPV4 initiation. 30,38,39 We were not able to survey parents and medical providers directly as part of this study.
The majority of our survey participants reported that their providers discussed HPV vaccine benefits and possible side effects with them. All providers within the health plan provide the Gardasil Vaccine Information Sheet (VIS) to patients as part of routine care. Our finding that age is associated with the likelihood of provision of specific information by providers about HPV suggests that providers in our health plan are tailoring how they deliver this vaccine and communicate about the vaccine according to their patients' age. For example, most participants regardless of age reported talking with their providers about the risks and benefits of HPV vaccine, but younger girls were much less likely than older females to report that their providers discussed Pap tests and genital warts. Our findings are consistent with a nationally representative survey of pediatricians and family practitioners, who report they are tailoring the information they deliver about HPV and vaccine according to the age of their patient. 29
The most significant limitation of this study is our 27% response rate. It is very difficult to engage preteens and teens in survey research, and our response rate is consistent with that of other surveys in this age group. 40 –42 Although we had expected that a web-based survey might be appealing to young women, our respondents were more likely to complete the paper-based format. Additionally, parents may have refused participation for their daughters rather than the young women themselves refusing to participate. We know this occurred in nine instances before we mailed our survey materials to the participant, but we did not collect additional data about parental vs. participant refusals after our materials were mailed.
We observed some important differences between survey responders and nonresponders, especially in SES and race/ethnicity. Females with lower SES were less likely to complete the survey. Other studies have shown that SES and race/ethnicity are associated with knowledge and beliefs about HPV and vaccine, so our findings must be interpreted carefully. 22,23,25,27 We were not able to analyze race/ethnicity in depth in this study because this information was available for only 44% of our sample. We do not expect, however, that participation bias affected our reported adverse event rates. We did not observe any difference in coded adverse events between respondents and nonrespondents, and our rates of reported adverse events were consistent with those in previous clinical trials.
An important strength of our study is that we were able to use EMR data to identify females within 1–2 days of their vaccination and survey them shortly thereafter. Most survey responses were received within 2 weeks of the index vaccination; we believe this minimized the potential for poor recall and misclassification of adverse events and details about the participant's interaction with the provider and health plan. We were not able to survey providers as part of this study, so our findings about patient-provider interaction are limited to reports from the patient perspective only.
Providers have a significant role to play as one of the most important sources of vaccine information and recommendations from a patient's perspective. 30,38,39 Understanding young women's experiences with this vaccine can help providers develop better strategies for improving HPV4 initiation and completion rates. For example, concerns about possible vaccine adverse events are frequently cited as a barrier to HPV vaccine initiation and completion in young women. 6,13,29,30 The information we have provided here about adverse events following HPV4 injection can be used to help providers better inform and communicate with patients about adverse event expectations after vaccination, which may in turn lead to improved vaccine uptake and completion. Specifically, young patients and those receiving multiple vaccines may need more adverse event information than older patients and those receiving HPV4 alone. Providers may also want to consider administering HPV4 alone when possible to minimize the risk of local reactions and presyncope. Additionally, providers should follow ACIP recommendations by monitoring seated patients for 15 minutes after vaccination to reduce the risk of syncope, particularly in younger patients and in those who report dizziness.
This study was the first to survey young women in a managed care population about their experiences with their first HPV4 injection shortly after initial vaccination. We found important age differences in young women's HPV4 experience in our health plan. Many of the young girls are receiving other recommended adolescent vaccines at the time of their HPV vaccination and although they are receiving information about the risks and benefits of the vaccine, are not receiving as much information about HPV itself as are older patients. Older women have more knowledge of and are receiving more information from their providers about the association between HPV and cervical cancer and genital warts.
Footnotes
Acknowledgments
Financial support for this study was provided in full by the Centers for Disease Control and Prevention (200-2002-00732) through America's Health Insurance Plans. The manuscript was reviewed and approved through the clearance process of the Centers for Disease Control and Prevention before submission. The findings and conclusions in this report are those of the authors and do not necessarily represent the official positions of the Centers for Disease Control and Prevention or America's Health Insurance Plans. We thank Jill Mesa, Carrie Meeks, JaNice Brewster, and Eresha Bluth for assistance with data collection and Dr. Matthew Daley for assistance with survey development.
Disclosure Statements
No competing financial interests exist.