
Abstract
Background:
Our group has shown a positive dose-response in maximal cardiorespiratory exercise capacity (
Methods:
We examined 365 sedentary, overweight, hypertensive, postmenopausal women randomly assigned to sedentary control or exercise groups exercising at 50% (4 kcal/kg/week, [KKW]), 100% (8 KKW) and 150% (12 KKW) of the National Institutes of Health (NIH) Consensus Development Panel physical activity guidelines. Primary outcomes included time and frequency domain indices of HRV.
Results:
Overall, our analysis demonstrated a significant improvement in parasympathetic tone (rMSSD and high frequency power) for both age strata at 8 KKW and 12 KKW. For rMSSD, the age-stratified responses were: control, <60 years, 0.20 ms, 95% confidence interval (CI)−2.40, 2.81; ≥60 years, 0.07 ms, 95% CI −3.64, 3.79; 4 KKW, <60 years, 3.67 ms, 95% CI 1.55, 5.79; ≥60 years, 1.20 ms, 95% CI −1.82, 4.22; 8-KKW, <60 years, 3.61 ms, 95% CI 0.88, 6.34; ≥60 years, 5.75 ms, 95% CI 1.89, 9.61; and 12-KKW, <60 years, 5.07 ms, 95% CI 2.53, 7.60; ≥60 years, 4.28 ms, 95% CI 0.42, 8.14.
Conclusions:
Introduction
The risk for cardiovascular disease (CVD) increases in women after menopause.
1
As with men, maximal cardiorespiratory exercise capacity (
In a recent report detailing the primary outcomes of a large clinical trial involving exercise training in postmenopausal women, the Dose Response to Exercise in Women (DREW) trial, we demonstrated a significant dose-dependent improvement in
The answer to this question is important to the aging process in women, as in one of our ancillary reports stratified by age, we found that regardless of exercise dose, women aged >60 showed an attenuated response in
Materials and Methods
Study design
The complete design, methods, and primary outcomes of our study are presented elsewhere.
9,24
Briefly, the DREW study was a randomized, dose-response exercise training trial complying with the Declaration of Helsinki comparing a nonexercise control group with three groups exercising at incremental doses (50%, 100%, and 150%) of the minimal NIH Consensus Development Panel's recommendation for energy expenditure.
10
The Cooper Institute and Pennington Biomedical Research Center's institutional review boards reviewed DREW annually. The primary outcomes for the DREW study included
Participants
After an initial evaluation and run-in period, we randomized 464 postmenopausal women (45–75 years) to one of three exercise groups or a nonexercise control group for a 6-month intervention period. The exercise intensity for this study was fixed at 50% of measured
Study participants were sedentary (exercising <20 minutes, <3 days/weeks, <8000 steps/day assessed over the course of 1 week), overweight or obese (body mass index [BMI] 25.0–43.0 kg/m2), and had a systolic blood pressure of 120–160 mm Hg. We excluded women who had a history of stroke, heart attack, or any serious medical condition that prevented them from adhering to the protocol or exercising safely. Our current analysis is limited to 365 women who successfully completed both
Heart rate variability
Although many indices of HRV exist, the time and frequency domain indices are the most common. For the time domain, the root mean square of successive RR intervals (rMSSD) represents parasympathetic nervous system activity, and the standard deviation of normal beat-to-beat (RR) intervals (SDNN) is a global index encompassing both the sympathetic and parasympathetic nervous systems. For the frequency domain, high frequency (HF, 0.15–0.40 Hz) power has been linked to vagal activity, whereas the role of other indices is less clear. 6 Nonetheless, we also calculated additional frequency domain spectra, such as low frequency power (LF, 0.04–0.15 Hz), very low frequency power (VLF, 0.0033–0.04 Hz), and total frequency power (PT, 0.00–0.40 Hz).
We examined each participant's HRV between 6:30
Statistical analysis
We used a generalized linear model to analyze the influences of the differing doses of exercise training on HRV characteristics. We focused our primary analysis on the time domain index of rMSSD, as it is sensitive to short periods of recording time.
6
We also examined the frequency domain index HFLn as a means of examining parasympathetic activity. We adjusted all our outcomes among the randomization groups for select specified covariates, including baseline HRV, race, and use of antidepressant medication. Given that this is an ancillary analysis in a large cohort, we first reproduced the findings of our primary outcome study and other ancillary reports from which we formed our current research question. The results were consistent, so we undertook further analysis to answer the question of whether age affects HRV improvements associated with exercise training. To accomplish this, we subdivided women by age into those <60 years and ≥60 years of age, given our recent report showing that this latter age group was unresponsive to exercise training as determined by changes in
Results
We show the clinical and demographic data for our cohort in Table 1. Similar to our previous reports, we observed that
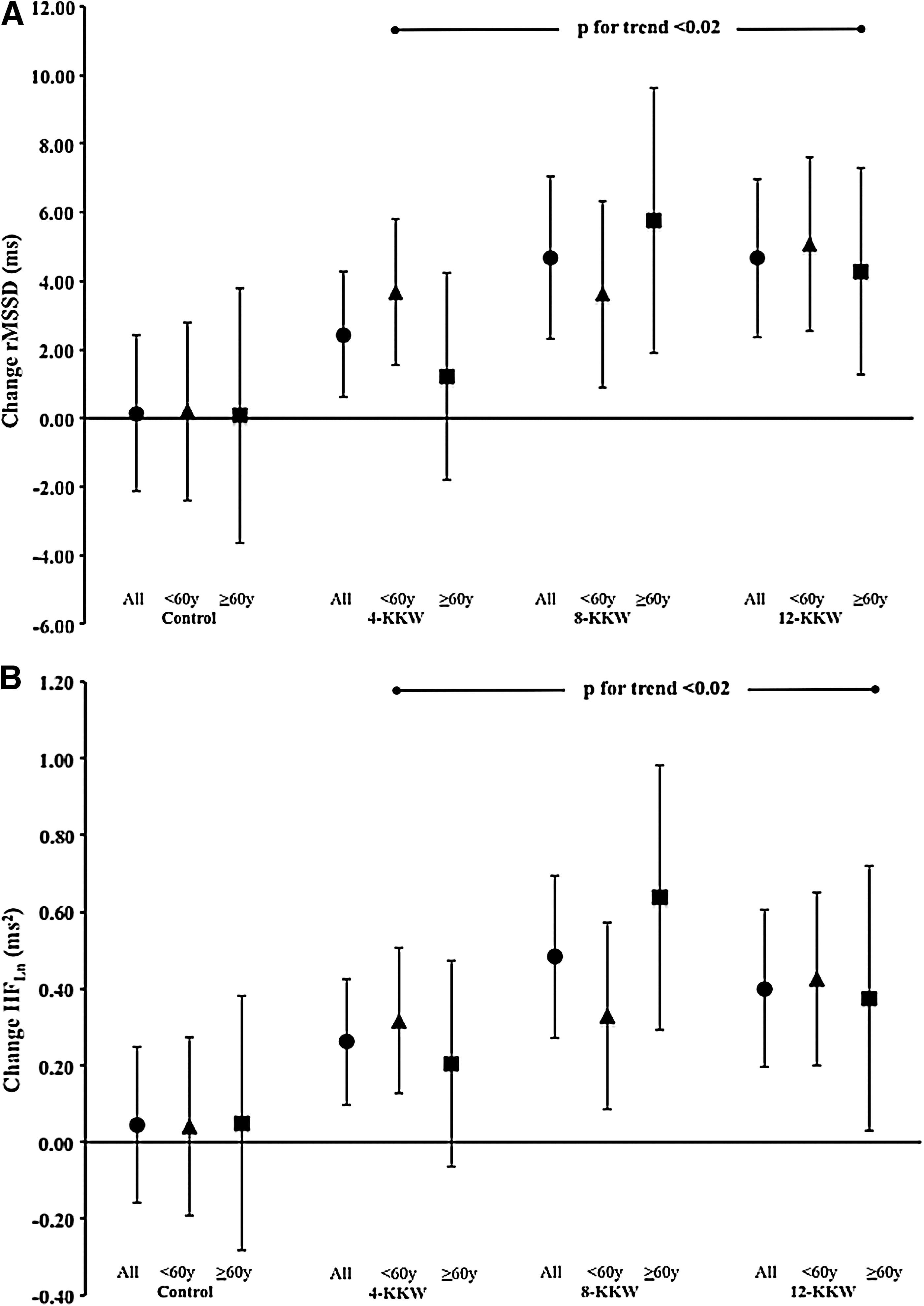
Data represent changes the root mean square of successive RR intervals (rMSSD) indicative of changes in parasympathetic nervous system activity for the entire Dose Response to Exercise in Women (DREW) cohort
Significantly different from <60 years.
BMI, body mass index; HDL, high-denisty lipoprotein; HRV, heart rate variability; hsCRP, high sensitivity c-reactive protein; LDL, low-density lipoprotein; LF, low frequency; RER, respiratory exchange ratio; rMSSD, root mean square of successive beat-to-beat intervals; SD, standard deviation; SDNN, SD of normal RR intervals;
Discussion
The primary finding from our study demonstrates that low-to-moderate intensity exercise training increases parasympathetic activity in previously sedentary, overweight or obese, postmenopausal women regardless of age. Of particular importance to our findings is the observation that women ≥60 years of age showed a significant improvement in HRV despite demonstrating no improvement in
Regarding exercise interventions, Davy et al. 23 reported in 8 postmenopausal women that HRV did not improve after 12 weeks of aerobic exercise at 70% of maximal heart rate. In contrast, Stein et al. 22 demonstrated an improvement in HRV characteristics for older women exercising for 12 months, and Albinet et al. 21 recently showed that HRV increased in older men and women after 12 weeks of exercise training. Still, these latter two studies comprised 18 and 13 women, respectively, who were further divided into two treatment groups. Although the results of these early exercise intervention trials suggest that the effects of exercise on HRV may be equivocal, we are now able to confirm the findings of the those studies showing a positive modulation in autonomic nervous system activity accompanying exercise training in a large cohort of women ≥60 years of age. The findings of our study are clinically important because the autonomic nervous system function is associated not only with CVD risk but also with a number of health-related issues, such as mood, depression, anthropometry, extreme physical exertion, cognitive and executive functioning, and vagal control of the cardiovascular system. 6,11 –17,27
Overall, parasympathetic activity is higher in women than men, yet aging reduces this difference in that parasympathetic activity shifts to a lower range after menopause.
28
–32
Heart rate variability (HRV) is a good example of how the risk for CVD may be improved with exercise during aging as a result of changes in systems physiology independent of improvements in
A primary strength of the DREW study is that it was a large, well-controlled exercise training study with excellent exercise adherence and a low dropout rate. The DREW study was also well positioned to answer the research question that we have posed given the large number of women ≥60 years in our study. The DREW study has limitations because its sample is limited to sedentary, overweight or obese, postmenopausal women at a moderately elevated risk of CVD. Therefore, we do not know if the results will apply to other women or to men. Additionally, although the results of our study show that postmenopausal women can improve their HRV with exercise without improving
The important point, however, is that our current findings strongly suggest that HRV is improved in older women partaking in a low-to-moderate intensity exercise program irrespective of changes in
Footnotes
Acknowledgments
This work was funded by grant HL66262 from the National Institutes of Health. We thank Life Fitness (Schiller Park, IL) for providing exercise equipment.
Disclosure Statement
C.P.E. has received honoraria for lectures from scientific, educational, and community groups. T.S.C. has received honoraria for lectures from scientific, educational, and community groups, served as a consultant for Trestle Tree Inc, and has a book in publication from which he will receive royalties. S.N.B. reports receiving book royalties from Human Kinetics; honoraria for service on the Medical Advisory Boards for Matria Health Care, Magellan Health Services, and Jenny Craig; and honoraria for lectures from scientific, educational, and community groups. He also reports that the University of North Texas pays him as an Executive Lecturer; he gives these fees to the University of South Carolina Educational Foundation or to other nonprofit groups. During the past 5-year period, he has received a research grant from Jenny Craig.