
Abstract
Background:
Limited data are available on hepatitis rates during pregnancy by socio-demographic characteristics. This study examined temporal trends in hepatitis B virus (HBV) and hepatitis C virus (HCV) mono-infections and HIV/HBV and HIV/HCV co-infections in subpopulations among pregnant women in Florida between 1998 and 2007.
Methods:
We analyzed all Florida live births from 1998 to 2007 using hospital discharge data linked to birth records.
Results:
The total sample size was 1,700,734 singleton live births. The prevalence of HBV in pregnancy rose from 65.4 per 100,000 births to 123.5 per 100,000 births (p<0.0001 for trend), and the prevalence of HCV in pregnancy increased from 17.0 per 100,000 births to 125.1 per 100,000 births (p<0.0001 for trend). Compared with white mothers, black mothers were more than twice as likely to have HBV in pregnancy (adjusted rate ratios [ARR]=2.24; 95% CI=1.97–2.53). Black mothers were 69% (ARR=0.31, 95% CI=0.25–0.39) and Hispanic mothers were 51% (ARR=0.49, 95% CI=0.41–0.60) less likely to have HCV compared with white mothers.
Conclusions:
Although the overall prevalence rate of HBV increased over the past decade, black women still had a noticeably higher rate of infection. Similarly, white women and those with HIV co-infection had noticeably higher rates of HCV infection over the study period. Our findings call for improved and increased HBV/HCV prevention, screening, and immunization programs among minority women of childbearing age.
Introduction
In the United States, between 800,000 to 1.4 million people are estimated to be chronically infected with hepatitis B virus (HBV), 2.7 million people are chronically infected with hepatitis C virus (HCV), and over 1.0 million people are living with HIV today. 1 –4 By sharing the same modes of transmission, co-infection with HBV or HCV in HIV-infected pregnant women may increase the risk of chronicity in the immunosuppressed host 1 and have a higher risk of vertical transmission of the hepatitis virus from mother to child. 5,6 Though the exact prevalence of HBV and HCV infection among women of childbearing age is not well established, it has been estimated that HBV affects 0.19% of women, while HCV affects 1% of women living in the United States. 7 –9 Studies have shown that HBV and HCV infection rates vary by race and ethnicity. 3,7 –10 Estimates for the prevalence of HBV and HCV infections among pregnant women who are co-infected with HIV in the United States are 1.5% and 4.9%, respectively. 11 HBV and HCV infections during pregnancy are associated with an increased risk of maternal and fetal complications, 12 –15 and HIV co-infections with HBV or HCV during pregnancy have an increased risk of vertical transmission. 5
Few studies have estimated the prevalence of HBV or HCV during pregnancy by socio-demographic characteristics. Additionally, there is a paucity of data on HBV/HCV infection among pregnant women already infected with HIV. 5,11 In particular, the United States lacks current data on the disparities in rates and trends of HBV/HIV and HCV/HIV co-infection in antenatal populations. Determining which pregnant populations have an increased risk of HBV/HCV infection and understanding trend patterns over time would be helpful in allocating resources for prevention and management purposes (e.g., curtailing neonatal infections and mother-to-child transmission) in an efficient and cost-effective manner. In this study, we examine the temporal trends in HBV and HCV mono-infections as well as HIV/HBV and HIV/HCV co-infections among pregnant women in the state of Florida over a decade (1998–2007). We also explore potential disparities by investigating changes in those trends according to important socio-demographic and behavioral characteristics.
Materials and Methods
We conducted a population-based retrospective cohort study by using a de-identified version of the Florida-linked hospital discharge linked to birth certificate data files. Florida vital statistics birth records from 1998 through 2007 were linked to the Florida Agency for Healthcare Administration's Inpatient Hospital Discharge Data for the same period. This linked file has been used previously to explain the trends and rates in HIV/AIDS among pregnant women from 1998 through 2007. 16 The linkage process was found to be 97.6% successful through internal validation and the details of the linkage process have been submitted for publication (Mbah et al., unpublished data, 2011). All maternal socio-demographic information—maternal age, maternal race/ethnicity, educational level, and marital status—was abstracted from vital records. The hospital discharge data provided diagnosis information for hepatitis B, hepatitis C, HIV/AIDS, and alcohol and drug use during pregnancy. Tobacco use during pregnancy was determined from both sources. This linked data set contains information on singleton live births (n=1,700,734) only.
Maternal age was classified into three groups: <20 years, 20–29 years, or ≥30 years old at the time of delivery. Maternal race/ethnicity was categorized as non-Hispanic (NH) white, NH black, Hispanic, and other. If “ethnic Hispanic” was listed on the birth certificate, regardless of race classification, Hispanic was assigned. Marital status was dichotomized as single or married, with all women who were divorced, widowed, or of unknown marital status classified as single. Education was categorized into “college degree” (those with at least a bachelor's degree or 16 years of education) and “no college degree” (those without at least a bachelor's degree or less than 16 years of education).
Using ICD-9-CM codes, hepatitis B (070.20; 070.21; 070.22; 070.23; 070.30; 070.31; 070.32; 070.33), hepatitis C (070.41; 070.51; 070.70; 070.71), and HIV/AIDS (V08, 042-045, 079.53) diagnoses were abstracted from the hospital discharge data. Tobacco, alcohol, and drug abuse during pregnancy were also ascertained by hospital discharge data by using ICD-9-CM codes. Tobacco abuse during pregnancy was defined by ICD-9-CM codes that indicated tobacco use disorder or excessive tobacco use that is harmful to a person's health or social functioning (305.10); complicates pregnancy, childbirth, or puerperium (649.00-04); and has toxic effects (989.84). Alcohol abuse was defined by ICD-9-CM codes that include acute alcohol intoxication (303.00-03); alcohol dependence (303.90-93); nondependent alcohol abuse, such as “binge drinking” (305.00-03); alcohol-induced mental disorders (291.0-5, 9; 291.81-82, 89); and alcohol affecting fetus or newborn via placenta or breast milk (760.71). ICD-9-CM codes that denote drug dependence complicating pregnancy, childbirth, or the puerperium or post-delivery period (648.30-34) were used to define drug abuse.
Statistical analysis
The annual hepatitis B and hepatitis C prevalence rates among pregnant women were calculated by dividing the number of hepatitis B or hepatitis C cases by the total number of singleton live births for that year and multiplying it by 100,000. The same method was applied to HIV/AIDS co-infection with hepatitis B and hepatitis C and to calculate group-specific HBV, HCV, and HBV/HCV-HIV prevalence rates. Chi-square for trend tests were used to examine trends in HBV, HCV, and HIV co-infection with HBV/HCV across the 10-year study period.
17
Additionally, the 10-year rate ratios for HBV, HCV, and HIV/AIDS co-infection with HBV/HCV during pregnancy were compared among different subgroups, using one of the groups as a referent, from the period 1998 through 2007. A Poisson distribution was assumed for our data since the prevalence of infection among pregnant women in our study population was rare. We assumed that the probability of HBV or HCV among women at birth (y) per 100,000 live births is equal to some number r and is given by:
where λ is the expected value (mean) of y and r!=r(r − 1)(r − 2)…(2)(1). 18 Using the equation, we were able to derive the variance to estimate the standard errors and confidence intervals (CIs) around the prevalence rates. We corrected for intracluster correlation using the Generalized Estimating Equation (GEE) since some women had more than one live birth during the study period. 19 The GEE models adjusted for maternal age, maternal race/ethnicity, educational level, marital status, tobacco, alcohol and drug abuse, and year of delivery based on a review of the literature. Aggregates of residuals were used to examine regression models and goodness-of-fit. 20 All statistical analyses were performed using SAS (version 9.2, SAS Institute, Inc.). Tests of hypothesis were two-tailed and a p-value of <0.05 was considered statistically significant.
Results
During the 10-year period from 1998 to 2007, there were 1611 pregnant women with HBV infection and 1023 with HCV infection in Florida, as documented in hospital discharge records. There was an average of 161 prevalent cases of hepatitis B per year and 102 prevalent cases of hepatitis C per year. The rate of HBV in pregnancy in 2002 reached 114 per 100,000 births and slowly increased by 9% over 5 years to reach its highest level of 124 per 100,000 live births in 2007. The rate of hepatitis C in pregnancy steadily increased over the entire decade to reach its peak in 2007 at 125.12 per 100,000 births. Over the decade of study, the prevalence rate for hepatitis B during pregnancy in Florida increased by 89% (p<0.0001 for trend), while the prevalence rate of hepatitis C during pregnancy increased by about 635% (p<0.0001 for trend).
The frequencies and rates of HBV and HCV infection during pregnancy by maternal socio-demographic and behavioral characteristics are presented in Table 1. The study population was ethnically diverse, with NH black and Hispanic mothers representing 21.4% and 22.2% of all births, respectively. Though white mothers represented over half of all births during the study period, they only accounted for 19.6% of all cases of HBV in pregnancy. By contrast, 70.1% of all cases of HCV in pregnancy were detected in white mothers. Overall, married women represented 60.6% of all births and only accounted for 50.8% and 39.2% of all cases of HBV and HCV in pregnancy, respectively, whereas single women delivered 39.5% of all births in the total study population, yet comprised 49.2% and 60.8% of all cases of HBV and HCV, respectively.
Rate per 100,000 live singleton births.
Model adjusted for all variables listed in the table and year of delivery. Significant ARR values in bold font. ARR, adjusted rate ratios.
Analysis stratified by race/ethnicity revealed that NH black mothers had the highest prevalence rate of HBV in pregnancy at 176.1 cases per 100,000 births, while the prevalence rates for NH white and Hispanic mothers were 34.9 and 70.9 cases per 100,000 live births, respectively. Compared with white mothers, NH black mothers were more than twice as likely to have HBV in pregnancy (adjusted rate ratios [ARR]=2.24; 95% CI=1.97–2.53) (Table 1). The adjusted risk for HBV among Hispanic mothers was similar to that of white mothers.
For HCV, NH white mothers had the highest prevalence rate in pregnancy at 79.2 cases per 100,000 births, whereas the prevalence rate of NH black and Hispanic mothers with HCV were significantly lower, at 34.6 and 39.2 cases per 100,000 births, respectively. Even after adjusting for potential confounders, NH black mothers were 69% (ARR=0.31, 95% CI=0.25–0.39) and Hispanic mothers 51% (ARR=0.49, 95% CI=0.41–0.60) less likely to have HCV, compared with NH white mothers (Table 1).
The results of trend analysis overall and by race/ethnicity for HBV and HCV are shown in Figs. 1 and 2, respectively. From 1998 to 2007, the prevalence rate of HBV during pregnancy increased by 73% among NH black women (p<0.0001 for trend) and increased by 425% among Hispanic women (p<0.0001 for trend). There was not a significant change in prevalence rates of HBV among NH white women during the study period. The prevalence rate of HCV in pregnancy increased by 741% among NH white women (p<0.0001 for trend), increased by 299% among NH-black women (p=0.0002 for trend), and increased by 1855% among Hispanic women (p<0.0001 for trend).
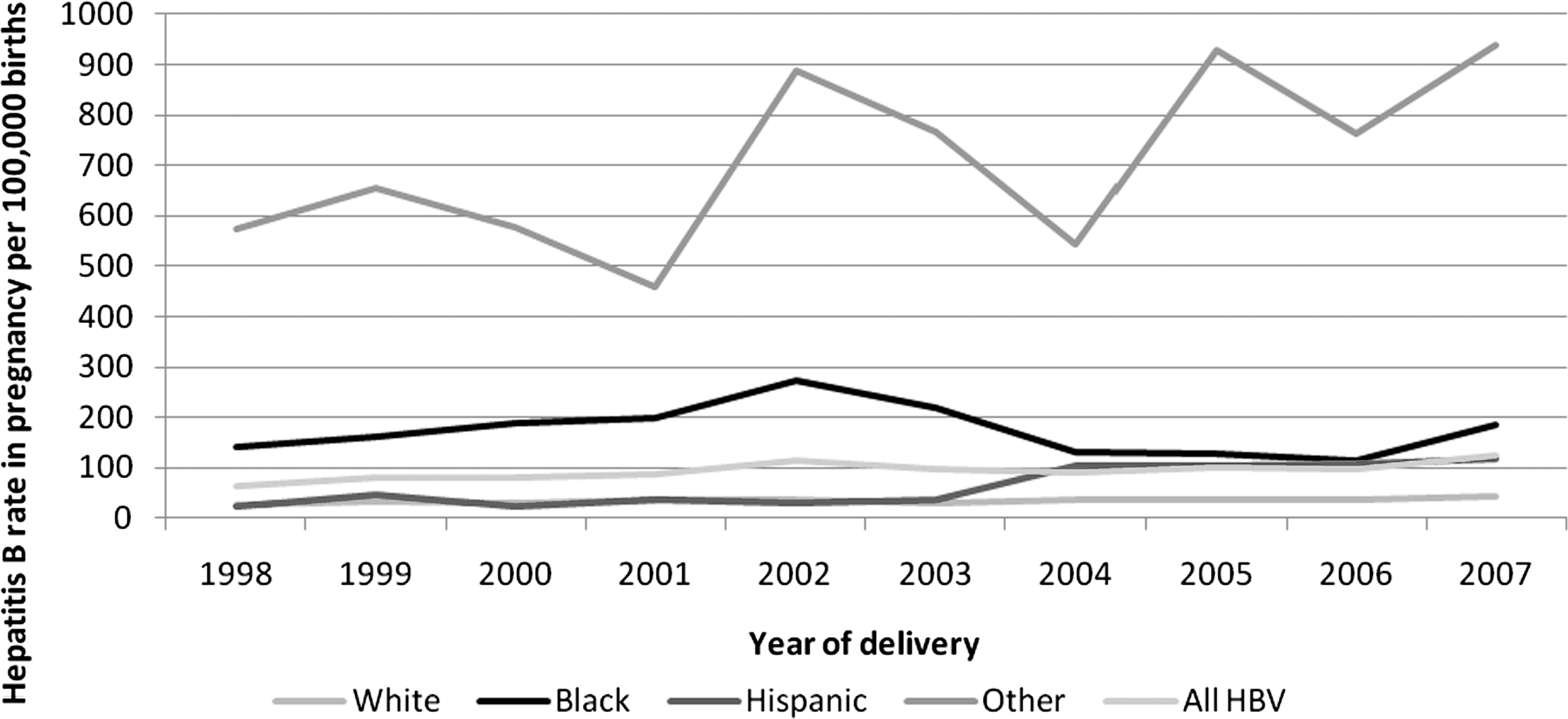
Hepatitis B rates in pregnancy in Florida from 1998 to 2007 per 100,000 singleton live births by race/ethnicity.
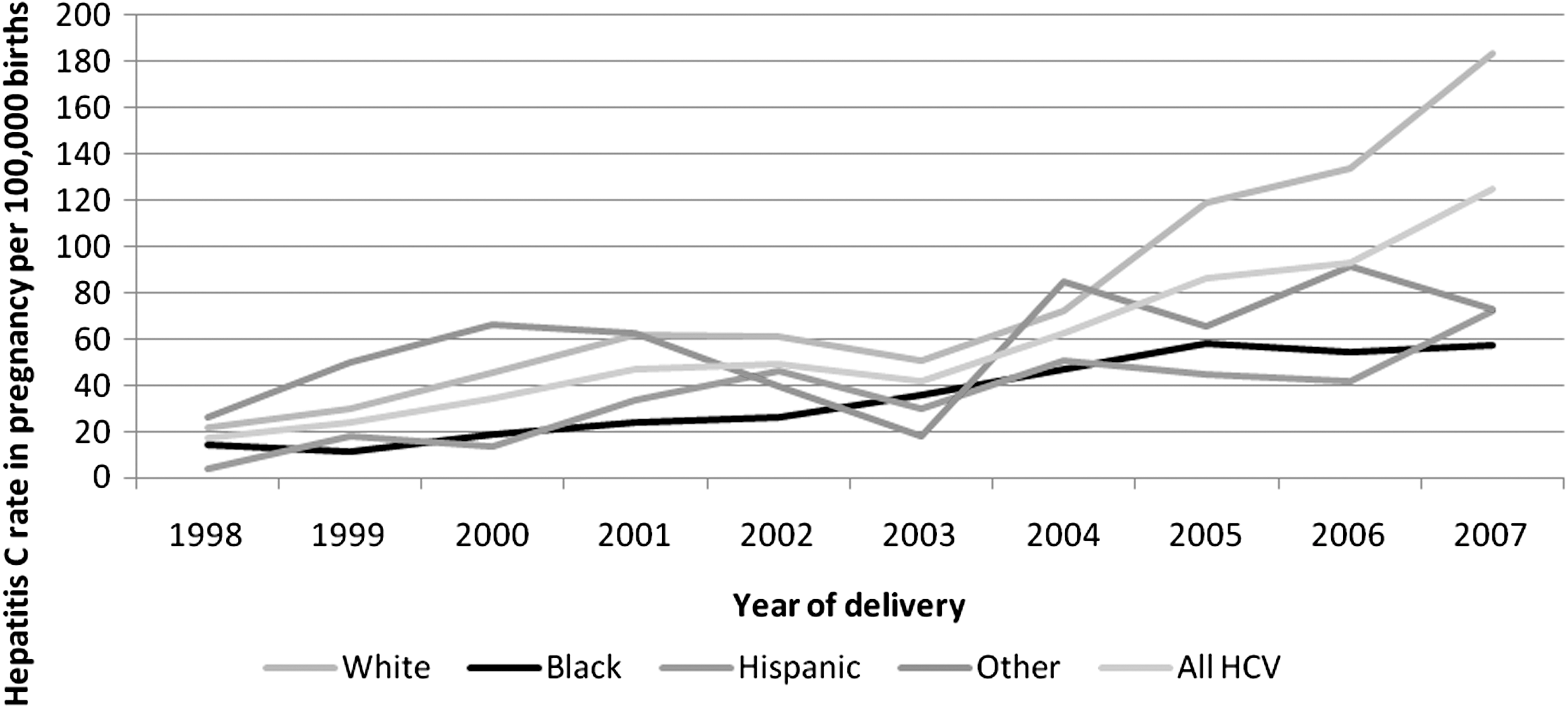
Hepatitis C rates in pregnancy in Florida from 1998 to 2007 per 100,000 singleton live births by race/ethnicity.
Trend analysis results for maternal age are depicted in Fig. 3 for HBV and Fig. 4 for HCV. Mothers aged 30 years or older had the highest prevalence rate of HBV and HCV (HBV=97.7 per 100,000 live births, p<0.0001 for trend; HCV=76.1 cases per 100,000 births, p<0.0001 for trend). The prevalence rate of HCV among women aged less than 20 years increased by 284% (p=0.002 for trend) and rose by 2547% among women aged 20 to 29 years (p<0.0001 for trend) from 1998 to 2007. Mothers aged 20 to 29 years and those 30 years or older were nearly 1.5 to 2 times as likely to have HBV in pregnancy compared with mothers aged less than 20 years (ARR=1.49, 95% CI=1.25–1.78; ARR=1.94, 95% CI=1.59–2.36, respectively) (Table 1). Mothers aged 30 years or older were more than seven times as likely as mothers under 20 to have HCV during pregnancy (ARR=7.31, 95% CI=5.25–10.20). Mothers aged 20 to 29 years were about four times as likely to have HCV infection in pregnancy compared with women aged less than 20 years (ARR=3.63, 95% CI=2.63–5.00).
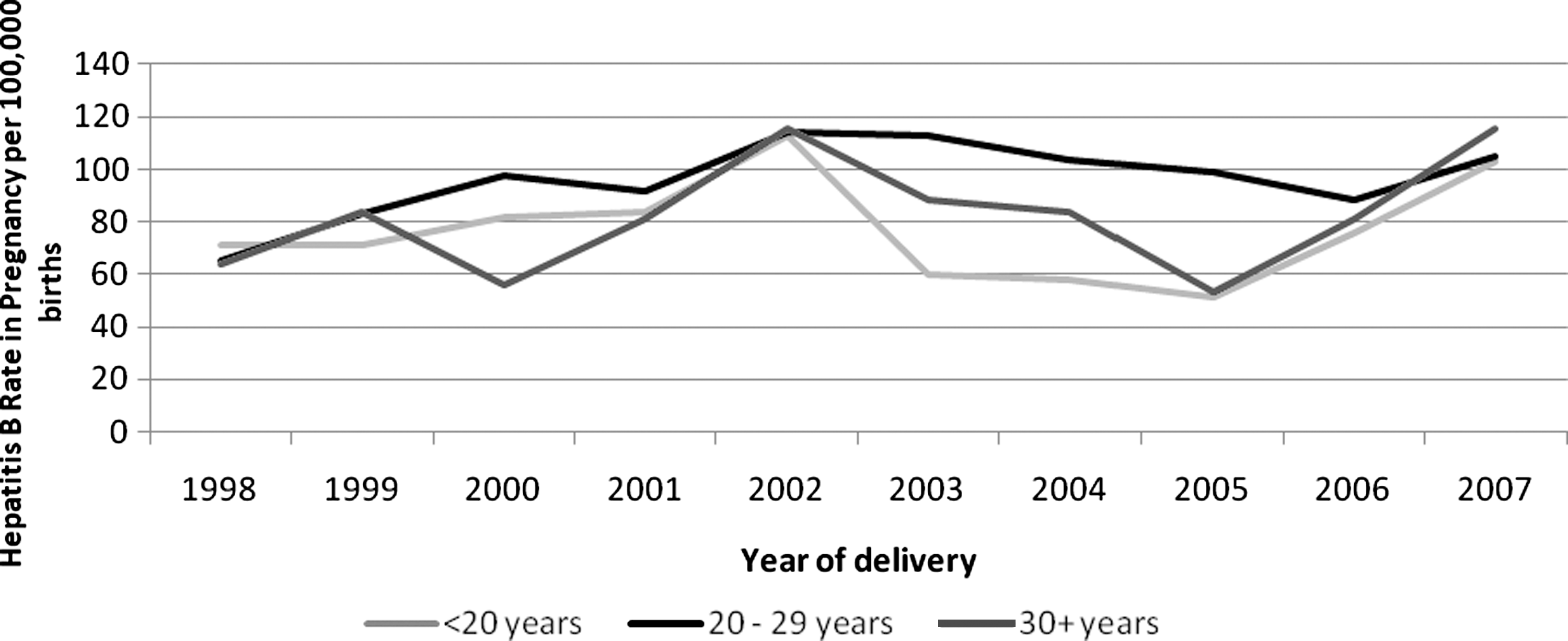
Hepatitis B rates in pregnancy in Florida from 1998 to 2007 per 100,000 singleton live births by maternal age at delivery.
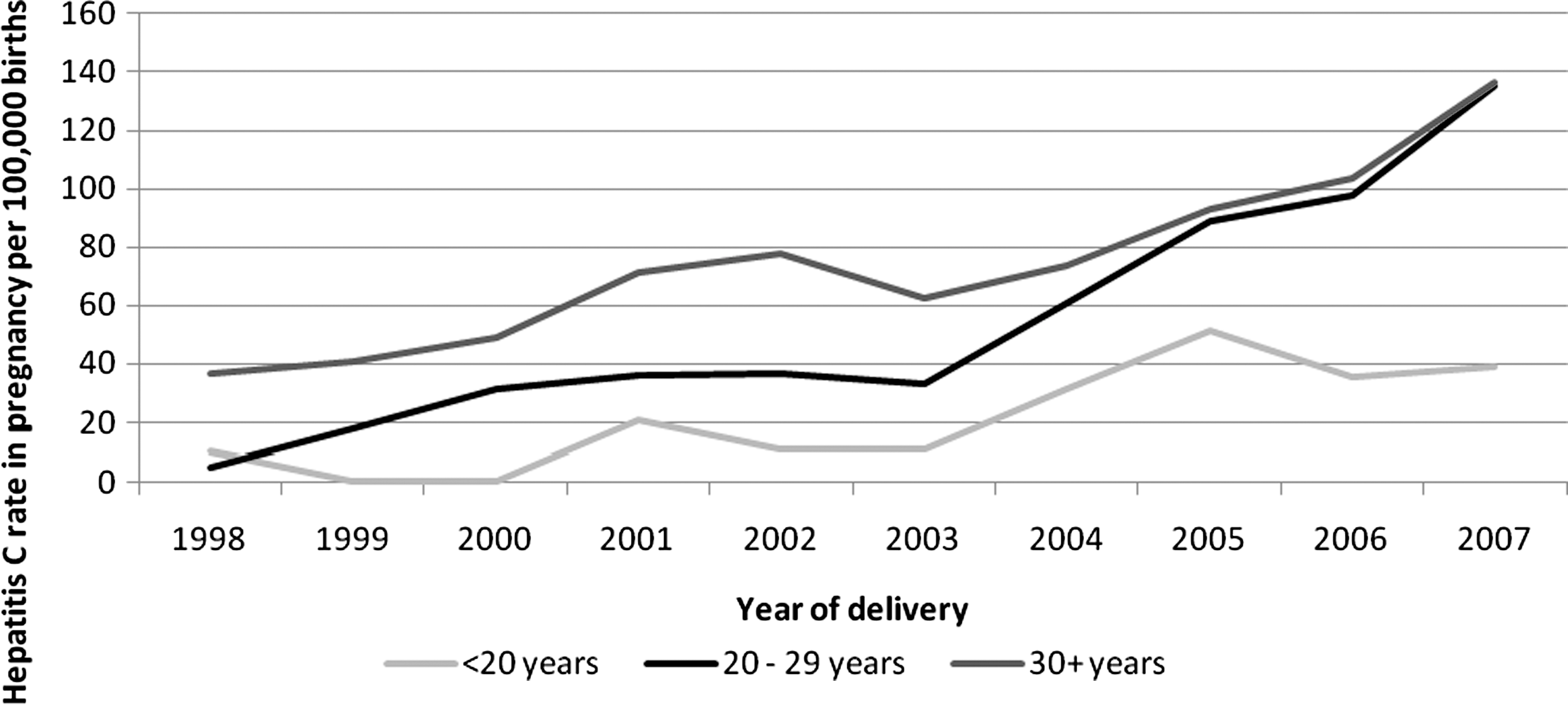
Hepatitis C rates in pregnancy in Florida from 1998 to 2007 per 100,000 singleton live births by maternal age at delivery.
Married women were less likely to have HBV and HCV in pregnancy as compared with single women (HBV: 79.4 vs. 118.2 cases per 100,000; HCV: 38.9 vs. 92.7 cases per 100,000); however, after adjustment for potential confounders, the reduced risk for HBV infection in married women was not significant (ARR=1.11, 95% CI=0.98–1.25). Lower education and tobacco and drug abuse were risk factors associated with both HBV and HCV during pregnancy. The relationship between drug abuse and HCV was particularly remarkable, with drug abusers showing a more than 10-fold elevated risk for HCV (ARR=10.2, 95% CI=6.72–15.57). Mothers with HIV/AIDS were more than seven times as likely to have HBV in pregnancy (ARR=7.25, 95% CI=5.49–9.57) and bore a more than 10-fold increased risk of HCV in pregnancy (ARR=10.25, 95% CI=6.60–15.93), as compared with HIV-negative mothers. The prevalence rate of HBV increased by 3% among women who were HIV/AIDS positive (p<0.0001 for trend), while the prevalence rate of HCV increased by 683% among women who were HIV/AIDS positive (p<0.0001 for trend) (Fig. 5).

HBV-HIV and HCV-HIV co-infection rates in pregnancy in Florida from 1998 to 2007 per 100,000 singleton live births.
Discussion
This study demonstrated a trend of increasing prevalence in hepatitis B among pregnant women within the past decade. In pregnant populations, a paucity of data exists regarding the prevalence rates and trends of hepatitis B and hepatitis C infection over time, especially in racial/ethnic subpopulations, which makes it difficult to compare prevalence rates associated with infections. Although the prevalence of hepatitis B among pregnant women is understudied, a cross-sectional study using data from the National Health and Nutrition Examination Survey (NHANES) estimated the prevalence of hepatitis B infection in the general U.S. population to be 0.27%, after age adjustment, which is three times more than that among pregnant women (0.09%). 7 Although these national data show lower hepatitis prevalence rates for pregnant women, the increasing trend in the HBV prevalence rate among Floridian women during pregnancy in our study is disconcerting, especially since hepatitis B infection in pregnancy is known to cause adverse perinatal outcomes. 12 –14
For hepatitis C infection, we found an increasing trend in the prevalence rates among pregnant women from 1998 through 2007; however, hepatitis C infection rates in the general population have plateaued since 2003 in the United States. 21 In Florida, there has been an increase in the number of incident cases reported to the health department since 2000, which may be attributable to new reporting requirements established by the state, making hepatitis C a notifiable disease in July 1999. 22 In addition, a cross-sectional study using data from NHANES to examine the prevalence of hepatitis C infection found the prevalence in the general U.S. population to be 1.6%, which was 26 times higher than the prevalence rate found among pregnant women (0.06%). 8 The lower prevalence of HBV and HCV infection among pregnant women compared with the general U.S. population may be explained by the young age of our study population. Since the implementation of universal HBV vaccination in 1991 for children and expectant mothers and their infants, the prevalence of hepatitis B has decreased among those aged 20–49 years of age. 7,21,23 The decline in HCV prevalence has occurred primarily among those aged 25 to 39 years, which may also be attributed to the decline in HCV incidence among injection drug users. 21
We observed a fivefold increase in the prevalence rate of hepatitis B among black mothers, as compared with white mothers. Similarly, Wasley and colleagues 7 conducted a large, population-based seroprevalence study from 1999 to 2006 and found that the prevalence of HBV is more than four times higher among blacks than among whites (12.2% vs. 2.8%). Currently, there are insufficient data to fully explain the racial and ethnic disparities of hepatitis B infection, but these disparities have been attributed to higher rates of exposure to HBV infection and lower rates of vaccination among blacks. 24 In 2003, the Viral Hepatitis Consensus Panel identified high-risk sexual behavior, illicit drug use, foreign birth, and low education among African Americans to be factors associated with disparities in HBV infection prevalence rates. 25
Interestingly, we found that the prevalence rate of hepatitis C among white mothers was more than twice that of both Hispanic and black mothers. In contrast, previous research in the general population has found that blacks generally have higher rates of hepatitis when compared with whites. 26 –28 However, when stratified by age and race, it was found that the difference in HCV prevalence rates among blacks and whites under the age of 40 was insignificant. 26 Studies of injection drug users and/or incarcerated populations have shown higher rates of HCV among whites when compared to blacks 29,30 ; however, this is the first study, to the authors' knowledge, to examine hepatitis C prevalence among pregnant women by race/ethnicity. As the predominant mode of HCV transmission in the United States is injection drug use, 22,26 which is a practice that is more frequent among whites, 31 substance use among white mothers may be a critical factor in the elevated rates of HCV. This explanation for the observed increase is, at best, speculative and warrants further investigation.
Our study showed that women with HIV/AIDS, compared with HIV-negative mothers, were more than seven times as likely to be co-infected with HBV during pregnancy (ARR=7.25, 95% CI=5.49–9.57) and were more than 10 times as likely to have HCV during pregnancy (ARR=10.25, 95% CI=6.60–15.93). Since HIV/AIDS is associated with an increased risk of vertical transmission of hepatitis from mother to infant, 5,32 the high prevalence rate of HIV/AIDS co-infection with HBV/HCV is a cause for concern.
A limitation of our study is that the level of hepatitis B or hepatitis C viremia was unknown, with our study population consisting of a combination of those with and without viremia; therefore, we were unable to determine whether women had a past or present infection or their vaccination history for hepatitis. Additionally, the reported independent association in this study between tobacco and alcohol abuse and hepatitis B, as well as drug and tobacco abuse and hepatitis C, might have been underestimated since drug, alcohol, or smoking abuse during pregnancy had to be noticeably pronounced to be diagnosed as a case of abuse.
In summary, the overall prevalence rate of HBV and HCV infection during pregnancy increased over the decade, which is a source of concern. Furthermore, the alarming rate of HIV/AIDS co-infection with HBV/HCV warrants further investigation to confirm these findings and requires additional research to guide evidence-based management of HIV-HBV/HCV co-infection in pregnancy. The fact that black women had a noticeably higher rate of HBV infection is equally worrisome and calls for improved prevention, screening, and immunization programs, especially among minority women.
Footnotes
Acknowledgments
We thank the Florida Department of Health and Florida Agency for Health Care Administration for providing the data files used in this study.
Disclosure Statement
None of the authors of this manuscript have conflicts of interest with this research.