
Abstract
Purpose:
By 2006, women constituted 34% of academic medical faculty, reaching a critical mass. Theoretically, with critical mass, culture and policy supportive of gender equity should be evident. We explore whether having a critical mass of women transforms institutional culture and organizational change.
Methods:
Career development program participants were interviewed to elucidate their experiences in academic health centers (AHCs). Focus group discussions were held with institutional leaders to explore their perceptions about contemporary challenges related to gender and leadership. Content analysis of both data sources revealed points of convergence. Findings were interpreted using the theory of critical mass.
Results:
Two nested domains emerged: the individual domain included the rewards and personal satisfaction of meaningful work, personal agency, tensions between cultural expectations of family and academic roles, and women's efforts to work for gender equity. The institutional domain depicted the sociocultural environment of AHCs that shaped women's experience, both personally and professionally, lack of institutional strategies to engage women in organizational initiatives, and the influence of one leader on women's ascent to leadership.
Conclusions:
The predominant evidence from this research demonstrates that the institutional barriers and sociocultural environment continue to be formidable obstacles confronting women, stalling the transformational effects expected from achieving a critical mass of women faculty. We conclude that the promise of critical mass as a turning point for women should be abandoned in favor of “critical actor” leaders, both women and men, who individually and collectively have the commitment and power to create gender-equitable cultures in AHCs.
Introduction
T
A fundamental assumption of the seminal theory of critical mass promulgated by Kanter over 40 years ago is that “low relative numbers and the accompanying problems of tokenism affected the social environment of women in the workplace, causing isolation and impeding their ability to effectively perform their jobs.” 1 She suggested that, having a critical mass increases women's comfort level and eases some of the stress associated with being a minority. Etzkowitz et al. predicted that there would be a discrete point where the presence of a sufficient number of women in an organization would bring about a qualitative improvement in conditions and accelerate the dynamics of change. 6
Background to this study
In 2009, we received a grant from the National Institutes of Health, “Achieving a Critical Mass of Women Biomedical Faculty: Impact of 3 US Programs,” to answer the following question: Did the participation of women faculty in three career development programs (CDPs) lead to increased numbers of women biomedical faculty in AHCs who were better prepared to assume leadership roles? Our results showed that women who attended at least one of three national career CDPs, (1) endorsed acquiring a set of skills, which better prepared them for advancement and leadership 7 ; and (2) were more likely to be retained in AHCs than non-CDP peers providing a potential for gender equity in leadership. 8 For the purpose of this article, we define gender equity as “the process of allocating resources, programs, and decision-making fairly.” 9
In this article, we focus our examination on the theory of critical mass by asking, “Is having attained a critical mass of women in AHC institutions sufficient to catalyze organizational culture change in specific ways?” We conjectured that once a sufficient proportion of women were achieved, the AHC culture would become more inclusive of women on many levels, more gender equitable, and less tolerant of gender norms; and more women would assume leadership positions, including deans and department heads.
Methods
Population samples, data collection, and analysis
Our study of critical mass is seen through the lens of two groups: women who had attended at least one of three CDPs between 1988 and 2011, and institutional representatives, both men and women, holding leadership positions in AHC institutions in 2012 (AHC leaders). The CDPs are sponsored by the Association of American Medical Colleges (AAMC) (Early-Career Women in Medicine [EWIM] and Mid-Career Women in Medicine [MidWIM]) and the Drexel University College of Medicine [DUCOM] Executive Leadership in Academic Medicine program (ELAM®).
We analyzed two sources of data: qualitative interviews among women currently employed in AHC institutions who had attended at least one of the three CDPs, and focus groups with AHC institutional leaders. The objective of our qualitative analyses was to reconstruct the general perspectives of the respondents; the quotes presented are intended to be representative of the preponderance of evidence in answering our research question. 10
Qualitative interviews
Telephone interviews were conducted in 2012 by an interviewer specifically hired for this purpose, who subsequently became a member of the research team (S.L.N.), using an interview protocol that emerged from our conceptual framework depicting the individual and institutional influences on career advancement. 11 Women volunteered for these interviews after responding to an online survey, described in detail elsewhere. 7 These interviews were, on the average, 60 minutes in length. Women were purposefully selected based on following criteria: (1) PhD or MD, (2) which CDP they attended between 1988 and 2010, and (3) current academic rank. Biographical experiences before and after CDP attendance were obtained through a series of open-ended questions, such as “During your [xx] years in academic health center institutions, have you seen a change in the number of women who participate in leadership?” “Does this change you describe affect the institution, and if so, how?” “What system changes are needed to better include the contributions of women?” We used probes on skills, networking, strategic career decisions, and institutional support. Details about the methods and results of these interviews were published earlier in this journal. 12
Focus groups
To obtain the AHCs' institutional perspective on these issues, national leaders in AHCs were invited to participate in focus groups. Participants were recruited from the pool of institutional leaders attending national meetings of relevant professional groups. These groups included alumnae of the ELAM program and four groups convened under the auspices of the AAMC: the Group on Faculty Affairs (GFA) (
Participants were recruited if they had senior academic rank and substantial leadership/authority and were a current faculty member at an AHC institution. The authors sent invitations to the ELAM alumnae list, while AAMC staff sent invitations to members of GFA, GDI, GREAT, and GRAND. The letter of invitation included information about the NIH grant, its purpose, and the context in which the focus group was being held. Discussion groups were intentionally formed from those who accepted the invitations. In the aggregate, we sought diversity in terms of participants' gender, race and ethnicity, institutions, and leadership roles.
Open-ended questions, such as, “What changes do you see in the status of women at your institution?” “Thinking about leadership, are you seeing women represented in leadership roles at your institution—specifically are they ‘at the table’?’” were used to generate conversations about trends in AHCs, focusing particular attention on collaborative and translational research and faculty trends, institutional and national influences on these trends, and their impact on institutional policies and practice.
Analysis of interview and focus group data
We utilized a systematic, theory-guided approach to text analysis using a category system. This approach allowed us to be open to new interpretations of the content, by using a strictly controlled step-by-step process for analyzing interview and focus group transcripts. This coding and analytical process, called pattern matching and explanation building, is described by Yin as a methodological way to move from a lower to higher conceptual level of data interpretation. 13
The deidentified transcripts were imported into NVivo 10 and analyzed in two stages of content analysis. First, the interviewer coded the data to create coding structures (hierarchical or matrix displays) that conformed to the topics in the interview and/or focus group guides (S.L.N.). Other team members conducted independent review of transcripts (P.M., D.H., and G.C.). S.L.N. also reviewed the matrix displays with the focus group facilitators to gain consensus on the coding approach. Second, the entire research team verified and expanded the original (level 1) codes into higher levels of emergent themes and categories. The final coding display for the focus group data was a matrix organized by themes and categories, the original text and line number in which it appears in the transcript, and researcher comments. 14 For the interviews, a hierarchical display was developed and the research team used the display as a structure from which to interpret higher level data. Internal audits, frequent discussions, and member checking led to multiple edits of the initial coding structures.
We systematically compared the above datasets to determine whether they corroborated one another and discrepancies in the data through the triangulation process. Triangulation is a powerful technique that facilitates validation of data through cross verification from two or more sources. In particular, it refers to the application and combination of several research methodologies in the study of the same phenomenon. Triangulation gave us the opportunity to interrelate programs, individual and institutional spheres, and data sets. 15
Results
Forty-five former CDP participants were interviewed during 2012. Nine focus groups were held between December 2011 and September 2012; discussants were 74 AHC institutional representatives (51 women, 69%, and 23 men, 31%). Tables 1 and 2 show the pertinent demographics of the interview and focus group participants, respectively.
Total exceeds 45 since 30 attended two or more CDPs.
CDP, career development program; ELAM, Executive Leadership in Academic Medicine program.
Response rates were 19/20 for the ELAM groups (95%); 29/29 for the GFA/GDI groups (100%); 25/42 invited (57%) for the GREAT/GRAND groups.
The denominators indicate the number of individuals who responded to that item.
CTSA, Clinical and Translational Science Award; GDI, Group on Diversity and Inclusion; GFA, Group on Faculty Affairs; GRAND, Group on Research Advancement and Development; GREAT, Group on Graduate Research, Education and Training.
The analyses revealed two domains that are nested within AHCs: the Individual and Institutional Domains (Fig. 1). The data revealed key features within four spheres that influence women's experience as faculty. Even with a critical mass of women faculty (≥30%), these experiences are circumscribed by their gender, imposing normative expectations both inside and outside AHCs.

Key features within four spheres that influence women's experience as faculty in Academic Health Centers.
Individual domain: experience of being a woman within AHC culture
The experience of being a woman in AHCs was found in the following themes: rewards and personal satisfaction of meaningful work, inherent characteristics or personal agency, tensions created by the demands of cultural expectations of family and academic roles, and women's work to achieve gender equity.
Rewards and personal satisfaction of meaningful work
Many of the women had considered leaving AHC institutions, yet stayed due to the satisfaction and rewards of academia:
I love the academic environment. I learn all the time from my colleagues, residents, and students. There is no way really to impact healthcare in a broad sense outside of academia. All of that makes it an intellectually stimulating environment and the work rewarding. (Interview)
Personal agency of women in AHCs
The reasons women gave for seeking career development opportunities revealed ambition and motivation to advance in academia.
I've always been an ambitious person who wants to be the person in charge. [CDPs] are key and definitely high on the things I wanted to do. (Interview)
I asked three times to go to [CDP] and was told it wasn't necessary for me to go. So I asked again a number of times, and it took a chair change for me to actually go. (Interview)
Conflicting demands/expectations of traditional family and academic advancement
While women desired to progress in their academic careers, they also delayed or deferred opportunities to participate in career development activities and/or advance and assume leadership roles because they embraced their families as high priorities in making career choices.
[Dean] has been talking to me about doing ELAM for a while, and now that my children are out of the house, I may do it because I see it would be really great. (Interview)
I'm the primary parent…That's why now, 10 years into my career, is when I'm finally taking the time to get the proper training I need…it wasn't an option before, so it delayed my career. (Interview)
A few token women are included on some committees but the power is still with the male hierarchy in general. The men are playing golf on Sunday and making deals. I want to spend Sundays with my kids. It is discouraging, and I think the women who get to the highest levels got there by being men. (Interview)
Women working for gender equity
The CDP experiences enhanced participants' personal agency, which gave them confidence to assert themselves and create informal structures such as networks of women who had attended CDPs.
I learned to not be afraid to put my ideas out there and tell people what I want…to be more confident and assertive than I might not be otherwise. I realized that I”m not supposed to let my doubts hold me back and just finally stand up for myself. (Interview)
When I came back [from CDP] I recognized that we didn't really have a group of women together in one place.…We had a small group of women who would get together once a month. I recognized we needed to do something on a global scale so we reinstituted the women in medicine group and opened it up to everybody in the institution. (Interview)
When I see residents or medical students come through the program, I tend to be more prescriptive or proactive in terms of reaching out to them. You know, a lot of very assertive, overconfident male surgeons have no trouble going out there and getting what they want but some of the women, and even some of the men, tend to be a little more reticent to do that, so I try to coach them in that. And coach them in some of their networking and communication skills, that sort of stuff. So it's a small impact I will have but it's the sort of thing that is important for me. (Interview)
Some women established groups to support the career development of younger women; some sought leadership positions and mentored other faculty. Regardless of the obstacles presented above, some women in AHC institutions have promoted each other, with the goal of increasing the capacity of the institution to improve culture and gender equity.
I have had an important role in a departmental program for women in internal medicine, and have been in discussion with the leaders of that program to (assume) one of the associate vice chair positions. (Interview)
I do mentor a lot of the younger faculty, both men and women, probably more women than men.… what ELAM called leading from within. So, that's a pretty important role. (Interview)
I'm part of the educational programming group—the committee on gender equity. We bring in speakers and programs for all faculty to keep moving this [gender equity] forward. I look for topics on how to advance women and how do women advance themselves. (Interview)
Institutional domain: culture of AHCs
The categories emerging from the interview and focus group data were readily grouped into three themes: the sociocultural environment, the institutional influence on women's advancement, and women as leaders. Each of these three themes yielded several subthemes.
Sociocultural environment
Institutional adherence to sociocultural gender norms
The attitudes and actions of faculty demonstrate that traditional gender norms persist.
[Some of the women have] made a decision to be the trailing spouse. It's based on their own value system. It's not something that is imposed externally. They just decided that they're going to be the one that's the trailing spouse. (Focus Group)
The conflict that women have is sitting in a meeting where your partners go, “Our clinic profit is going down because [interviewee] is taking maternity leave.” Yet, earlier when one of the male partners' wife ended up in the hospital having a baby, they were, “Can we take your call? How can we help you?” I'm like, “He's not in the hospital. All you can say to me is that I'm going to affect your bottom line.” (Interview)
Lack of institutional strategies to engage women in organizational initiatives
In the normative sociocultural environment, the absence of institutional strategies to engage women in building institutional capacity was evident, even after they demonstrated intent to contribute after their CDP participation.
It's not just about “fixing the women.” It's about changing the environment so women don't need to be always the “fixed one.” (Interview)
She did the ELAM Program and she was the interim chair of internal medicine.… and they did a search for a chair and brought in a man to be the chair of the department. They didn't want her to be chair of the department—they said they wanted an outside person. Now they're looking for a chair of surgery and are looking for internal person for surgery. But yet, they wouldn't let her be the chair of internal medicine and she'd been at the ELAM Program. (Focus Group)
So you work on empowering women, you fix them, which we've talked about for years and years, then you put them back in that same place. What is the solution to the problems? Fixing the culture and how do you do that? (Focus Group)
Unconscious gender bias in behavior and policy
Our results revealed that unconscious sexism persists and is evident in communication patterns, individual behaviors, and institutional decisions to implement policies that differentially affect men and women. While well intentioned, the implementation of policies to support faculty life was not found to be gender equitable.
When I was hired in the department of pediatrics I didn't believe this, but now that I've been here 2.5 years, I feel gender discrimination all of the time. It makes me crazy and I can't figure out what to do about it since it's very, very subtle. (Interview)
Our part-time faculty is disproportionately women trying to balance children at home. They are not eligible for health benefits. There's no tenure track. They're not able to serve on key committees and not able to run for governance. (Interview)
If you are anything less than full-time, it's (permission for leave) by special exception, and it has to be something like a physical or a mental health need, not parental leave. (Focus Group)
Institutional influences on women's advancement
Positive or negative influence of individual leaders on women's career advancement
Our results revealed that individual leaders have an important influence, and often autonomy, to contribute to the building or dismantling of critical mass in their organizations.
It's because somebody in a leadership position has the resolve to do it. When [male Dean] took the position there, there were no female chairs or female associate deans. When he left the position last year, there were six female chairs and four female associate deans. Why? Because he kept sending the search committees back and saying, “You need to expand the pool. You need to go and actively find those people.” (Focus Group)
I went to him [department chair] and said, “Look at this. Do you realize what is going on?” [lack of women being recruited]. It is just not on his radar screen—the whole diversity issue is not on his radar screen. And so on the university level, when you look at leadership, it's a bunch of men. (Interview)
Individual and informal efforts to improve women's visibility and influence
Efforts to improve women's visibility and influence require commitment by individuals and institutions. We did hear about actions by women both as individuals and as a collective, for the sponsorship of women within institutions. Some leaders passively accepted women's efforts to build women's capacity or to develop informal mentoring groups because these leaders recognized the benefits of such initiatives, whether to build institutional capacity or to enhance their image of being a gender-equitable organization. While our data include statements reflecting awareness of organizational responsibility, no examples were provided of systematic strategies to meet this obligation.
I think about how to sustain this. I mean, we've had some good experiences with women in leadership positions, but are we at a new level? A new plateau? Are we continuing to go up? I really don't know. (Focus Group)
I looked at the benchmarks after [CDP] and we had only 17% female faculty. So I started putting together grassroots programs and a women in medicine program. They weren't actually unsupportive because they would never want to actively diss a women's program. They didn't give any flack about putting it together.. It also helped the departments and university look much more active in working toward gender equity. (Interview)
Women as leaders
Women in leadership roles
Our data revealed that the act of promoting women to mid- and senior-leadership roles was perceived to be evidence of gender equity. The increase in the small number of women in leadership positions appears to be commonly translated into “problem solved,” even though the data demonstrated that a critical mass of women in leadership positions has not yet been achieved.
He [Dean] says to me in defense of the system, “Our Sr. Associate Dean for Academic Affairs is a woman, as is the Associate Dean for Research Affairs. So we have women. So, how could there possibly be gender discrimination in high level positions?” (Interview)
The chairs, except for one, are all male. There were a number of females in associate dean roles, but the power resided with the chairs, who were all male, except for one. (Focus Group)
We appointed our new executive dean for research at the medical school, who is a woman and I think there are more efforts along those lines…having women in positions like that sends a signal that you can imagine having chairs of clinical departments who are women. (Focus Group)
Token women leader
Emerging from the data was the perception that having a woman in a leadership role, which was typically a mid-level position, solves the “problem.”
There are a few token women included on some committees and are the assistant deans, but the power is still with the male hierarchy. (Interview)
On paper it looks good—there were a number of females in associate dean roles, but under the previous dean, the power resided with the chairs—who were all male, except for one …The Student Affairs dean was female, associate dean level are 50/50 male/female. But it looked good on paper, but in reality, it was all male directors. (Focus Group)
Discussion
In this article, we present evidence of the influence of institutional culture and sociocultural norms on women's careers, gained from interviews with women and focus groups with institutional leaders. The findings highlight women's challenges and motivations to remain in AHC institutions, and the ways in which institutions enabled or welcomed their contributions in a meaningful way. The data from focus groups provide the perspectives of national leaders about the involvement of the academic culture in engaging women, in setting policies to support gender equity, and in strategically promoting women to leadership.
Although we never specifically asked a question about critical mass in the interviews or focus groups, the theory of critical mass became a conceptual framework for the analyses presented in this article. Our analysis identified features of critical mass formation that contribute to its effectiveness or ineffectiveness at changing organizational culture. First, the experience of being a woman in AHC institutions includes the rewards and personal satisfaction of meaningful work, inherent characteristics, or personal agency, as well as the tensions created by the demands of cultural expectations of family and academic roles that are changing and may be less acceptable to women and men today.
We found that the interface between the individual and the influence and engagement of the institution created a tension that slowed the attainment of the “promise” of critical mass. The themes suggested that the interaction between individuals and institutions had an important impact, both positive and negative, on cultural transformation. Also, the influence of one leader's (male or female) action or perspective could catalyze women's career development. On the other hand, the participants and institutional representatives reported myriad examples of organizational subtle, but pervasive adherence to outdated sociocultural gender norms and ineffectual efforts to improve women' experience. These include absence of institutional strategies for engaging women in organizational work, institutional gender bias limiting women's opportunities for leadership, negative impact of gender-equitable policies on women's advancement, and the perception that having women in mid-level leadership roles “solves” the problem. All these findings led us to conclude that the answer to our research question (“Is having attained a critical mass of women AHC institutions sufficient to catalyze organizational culture change in specific ways?”) is unfortunately, NO!
Critical mass theory posits that having 30% of faculty who are women should be sufficient for women to have made an observable impact on gender diversity and the sociocultural environment of AHCs. The percentage of women in AHCs increased from a few “token” faculty (<10%) in 1975 to 33% in 2006. 5 Since 2006, the overall proportion of these women faculty has grown only slightly, from 32% in 2005 to 38% in 2014. 16 In addition, proportions of women in executive positions have shown limited change since 2006; the current proportion does not approach a critical mass of women leaders, which some researchers have suggested is necessary for sustained organizational culture change. 17,18 Women department chairs have increased from about 10% to 15%, and deans to 16%. 5 Even in a discipline where the majority of faculty members are women (54%), very recent evidence documents that the proportion of permanent women chairs in OB-GYN departments rose from 0% in 1981 to only 22% by 2014. 5,19 –21 The evidence for an influential role of women as catalysts for change in AHCs has yet to materialize.
Most of the women participants in this study have advanced to be mid-level and/or senior leaders of AHC institutions; they have been retained and contribute to the critical mass. The interviews and focus group data reveal, however, that the cultures of AHC institutions do not actively/vigorously support the advancement of women faculty to leadership. Despite being underrepresented in the upper echelons, women stay within stagnant hierarchical cultures because of the personal rewards and satisfaction of what they describe as meaningful work. However, their impact as change agents often is foiled by the intransigence of that organization's culture. Jude Browne proposed that “situations where a disproportionate number of women exist at the level beneath (senior leaders) and the natural progression of these women toward higher levels in the institution does not materialize (sic)—there is, in other words, a ‘thwarted critical mass’.” 22 Therefore, the potential for a critical mass of women to act as a catalyst for a supportive work environment for women at all career stages remains unrealized. 23 –26
Outside of AHC institutions, there is a consensus that attaining a critical mass of women is not sufficient for creating a successful working environment. For example, Dalrup noted that women politicians have conflicting challenges: they must prove they are just as able as men but avoid being seen as to represent only “women's interests.” 1 Grey suggests that the theory of critical mass about women in politics is further complicated by the fact that women are by no means a coherent group. 3 Generally, the evidence is mixed; some political studies support the theory and others do not. 27 Recent reports about the field of technology document the failure of critical mass to be a catalyst for change. 28 Given these inconsistent findings, many researchers have been reconsidering whether to abandon the notion of critical mass altogether in favor of “critical actors.” 2,29 –31
Childs and Krook argued for a shift from focus on a critical mass to what specific men and women (“critical actors”) do to achieve cultural transformation—those who initiate cultural transformation and sponsor others to advance gender equity, even when women form a small minority. 3,32 –36 Unger et al., found evidence that the achievements of women leaders are more influential than those of a critical mass of individual women throughout an organization. 37
Applying the concept of critical actors to AHCs, we revisualize the depiction of the nested spheres of influence to hypothesize how critical actors might transform these institutions (Fig. 2). In this culture, the extrainstitutional critical actors are national leaders of foundations, funders and professional organizations. Intrainstitutionial critical actors include chancellors, deans, department chairs, and others who drive organizational change. The societal expectations of men and women are becoming more gender equitable, creating more flexibility for women. Within AHC institutions, the culture becomes more conducive to choices for women leading to greater recruitment, satisfaction, promotion, and retention. This will lead to a greater proportion of faculty who are women.
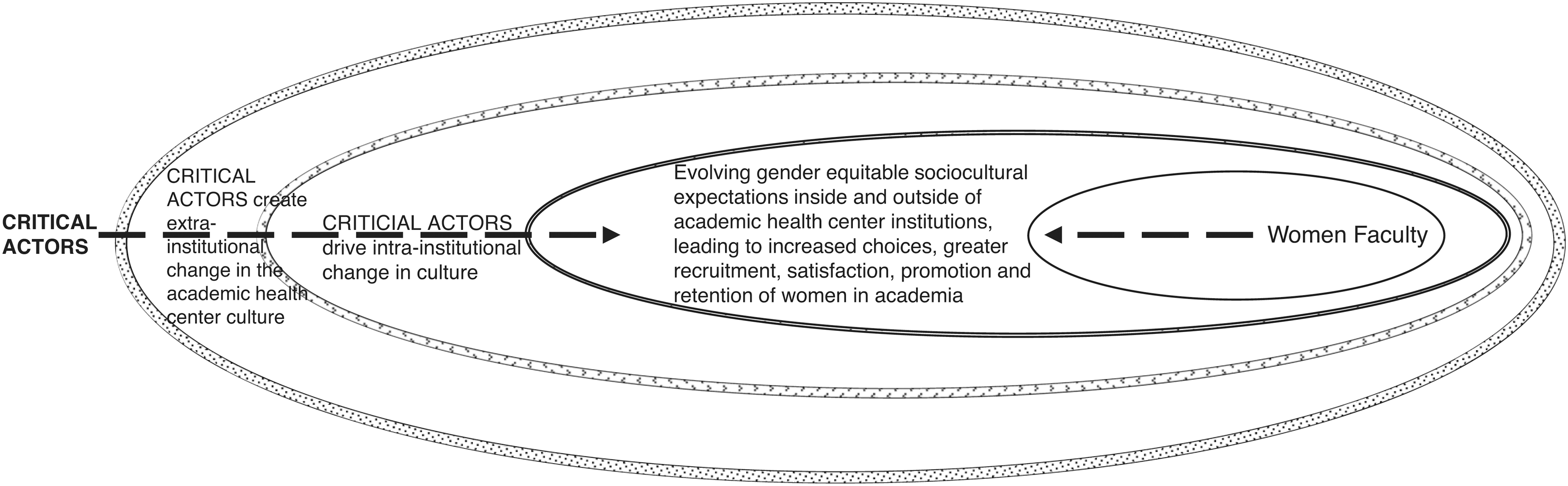
The influence of critical actors on the reform of the domains that influence women's experience in Academic Health Centers.
As with all studies, our research has limitations. Nearly two-thirds of the interviewees had attended more than one of the CDPs, providing a longitudinal perspective of change (or the lack thereof) in the organizational environment. However, the experiences of non-CDP women may be different. Our research found that non-CDP women were less likely to be retained in AHC institutions than their CDP peers. 8 Focus groups of self-selected academic leaders across U.S. AHCs offered their perceptions of gender equity and organizational culture at their own institutions, but these views may not be representative of all AHC leaders or all AHC institutions. Participants may have felt uncomfortable or unwilling to share personal experiences or professional beliefs fully in the focus group setting or in individual interviews. The AHC community is relatively small and individuals are often well known to each other. We were conscientious about redacting any identifying information, but some participants were reluctant to share stories that would make them vulnerable to discovery. Because of our efforts to deidentify transcripts and the nature of focus groups as discussions rather than comments from individual participants, we were unable to disaggregate comments based on seniority, race/ethnicity, gender, or institutional representation.
Conclusions
Our study shows that despite achieving a critical mass of women throughout AHC institutions, we have yet to see its promise. One question yet to be answered is whether 35% of women coming through the system is sufficient to exert changes on the environment of AHC institutions in particular. Perceptions about and realities of academia influence career trajectories and sustain unequal outcomes. Our study suggests that two features make a difference: an institutional culture that is highly receptive to changing existing cultural practices and changes in the perception that leadership roles are appropriate for women. 38 –40 Historically, the industrialized countries have followed a segregated pattern in the division of labor by gender, with work that is defined as being either masculine or feminine. 41 –43 Research has shown that leaders are more likely to be men than women, or, more specifically, androgynous and masculine persons are most likely to emerge as leaders. 43,44 Society sanctions men's aggressive and competitive behavior, which translates into social and economic power and authority over women. 45 The “role congruity” theory 46 has been tested; findings demonstrate that beliefs about leadership style and gender result in prejudice and discrimination toward women leaders, especially those with an autocratic style. 47 –52 Recent studies show that the United States ranked 28th overall among 156 nations in economic equality and 72nd in political empowerment of women. AHCs are nested systems in which individual institutions mirror the sociodynamics of the larger culture. 53 To date, the proportions of women chairs and deans of medical schools have not changed considerably, despite the fact that the number of Legislative Council on Medical Education-accredited medical schools has grown (from 125 in 20001,17 to 144 in 2015), 54 ostensibly providing more opportunities for leadership roles for women. To achieve momentum in these areas, leadership must be passionate about and committed to gender equity. 36
To erode the incongruities of being a leader and a woman in an organization, organizations must engage women in the development and implementation of institutional strategies to engage women in organizational initiatives and encourage critical leaders to foster women's ascent to leadership. 55 –57 Rather than focus on the development of a critical mass of women in AHC institutions, we argue that more women and men must become committed champions and leaders who are “critical actors” to catalyze cultural transformation. With more informed leaders and a bolder few 3,31,58 who are held accountable to “walk, talk, run, and shout” 59 gender equity, institutions may become more nimble and responsive to culture change.
Footnotes
Acknowledgments
The authors would like to acknowledge their appreciation for the collaboration of AAMC staff with survey item development and implementation. The authors also wish to thank the following members of the Advancing Women National Advisory Board who gave valuable feedback: Drs. Jasjit Ahluwalia, Carol Aschenbrener, Lorris Betz, Carmen Green, Sharon McDade, Sally Shumaker, and Diane Wara. This project was supported by the NIH Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), grant award number 1R01 HD064655-01, and the National Center for Research Resources and the National Center for Advancing Translational Sciences of the National Institutes of Health through grant number UL1 TR000041.
Ethical Approval
The authors obtained human subject institutional approvals from the University of New Mexico, MD Anderson Cancer Center (DR09-0396), and DUCOM (HRRC 09-556).
Author Disclosure Statement
Dr. Helitzer has taught as a faculty member in EWIM and MidWIM, and was a participant at MidWIM and ELAM. Dr. Morahan has taught as a faculty member in all three programs. She founded the ELAM program and directed it from 1995 to 2008; she now is Research Director for ELAM. Dr. Magrane has attended all three programs; from 2003 to 2008, she was Associate Vice President of Faculty Development and Leadership and program director and faculty for the WIM programs; she is now program director and teaches in ELAM. Dr. Chang has taught as a faculty member in EWIM and was a participant in MidWIM.