
Abstract
Background:
The association between menopausal vasomotor symptoms (VMS) and depressive symptoms remains controversial. We aimed to examine the associations between moderate–severe VMS and moderate–severe depressive symptoms.
Methods:
Nationally representative cross-sectional survey of 2,020 noninstitutionalized Australian women aged 40–65 randomly recruited between October 2013 and March 2014. Symptoms were assessed by the Menopause-Specific Quality of Life Questionnaire, the Beck Depression Inventory-II, with score ≥20 defined as moderate–severe depressive symptoms. Cigarette, alcohol, and psychotropic medication use was also assessed. Binge drinking was defined as four standard drinks on one occasion.
Results:
VMS were classified as moderate–severe for 267 of the 2,020 women (13.3%). After adjusting for multiple factors, including age, partnership status, paid employment, housing insecurity, and body mass index, when compared to women with no or mild VMS, women with moderate–severe VMS were more likely to have moderate–severe depressive symptoms (odds ratio [OR] 2.80, confidence interval [95% CI], 2.01–3.88, p < 0.001). Having moderate–severe depressive symptoms was associated with a greater likelihood of use of psychotropic medications (48.9%, 95% CI, 43.1–54.8 vs. 20.1%, 95% CI, 18.2–22.1, p < 0.001), smoking (25.9%, 95% CI, 20.8–30.9 vs. 12.2%, 95% CI, 10.6–13.7, p < 0.001), and binge drinking at least weekly (15.1%, 95% CI, 11.0–19.2 vs. 10.3% 95% CI, 8.8–11.7, p = 0.015).
Conclusion:
Moderate–severe VMS are independently and significantly associated with moderate–severe depressive symptoms.
Introduction
S
The present study was therefore undertaken to determine the association between moderate–severe VMS and moderate–severe depressive symptoms, using validated questionnaires in a randomly recruited, appropriately sized community sample. The rationale for assessing the association between depressive symptoms and VMS, rather than menopausal status, is twofold. First, in clinical practice, it can be difficult to classify menopausal status, especially for the nonspecialist, whereas VMS are a distinct clinical manifestation of menopause. Second, while research has linked the early postmenopause with depressive symptoms, many women will continue to experience bothersome VMS for many years after the final menstrual period. 7,17
Methods
Study participants
The study has been reported according to Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 18 Women were recruited from the Roy Morgan Single Source (RMSS) database, which contains over 300,000 respondents with 50,000 new participants each year. Recruitment to RMSS is based on the Australian electoral roll. Voting is compulsory in Australia, with all eligible adults' names and addresses registered on the roll. Australia's 150 electorates, each with ∼150,000 people, are divided into four roughly equal sections, creating 600 sampling areas. A starting address from each sampling area is randomly selected each month from a list of all known addresses. Face to face interviews are conducted to recruit people from these sampling points.
For the current study, community dwelling women aged 40–65, listed on the RMSS, were randomly recruited by telephone to a study of “the health of women at midlife,” as previously described. 19 Recruitment to the current study was deliberately designed so that the sample represented the age distribution of women within the target age group according to the 2011 Australian census. 20 The only exclusion criterion was being unable to complete a written questionnaire in English. Women interested in the study were sent the study questionnaire with a reply paid envelope, with return of a completed questionnaire accepted as informed consent. A total of 17,226 phone numbers on the RMSS database were dialed, resulting in 5,850 contacts (Fig. 1). Of 5,079 eligible women, 2,911 women were recruited with 2,051 questionnaires returned. The final sample included 2,020 completed questionnaires. Ethical approval was granted by the Monash University Human Research Ethics Committee (CF13/1281: 2013000648).
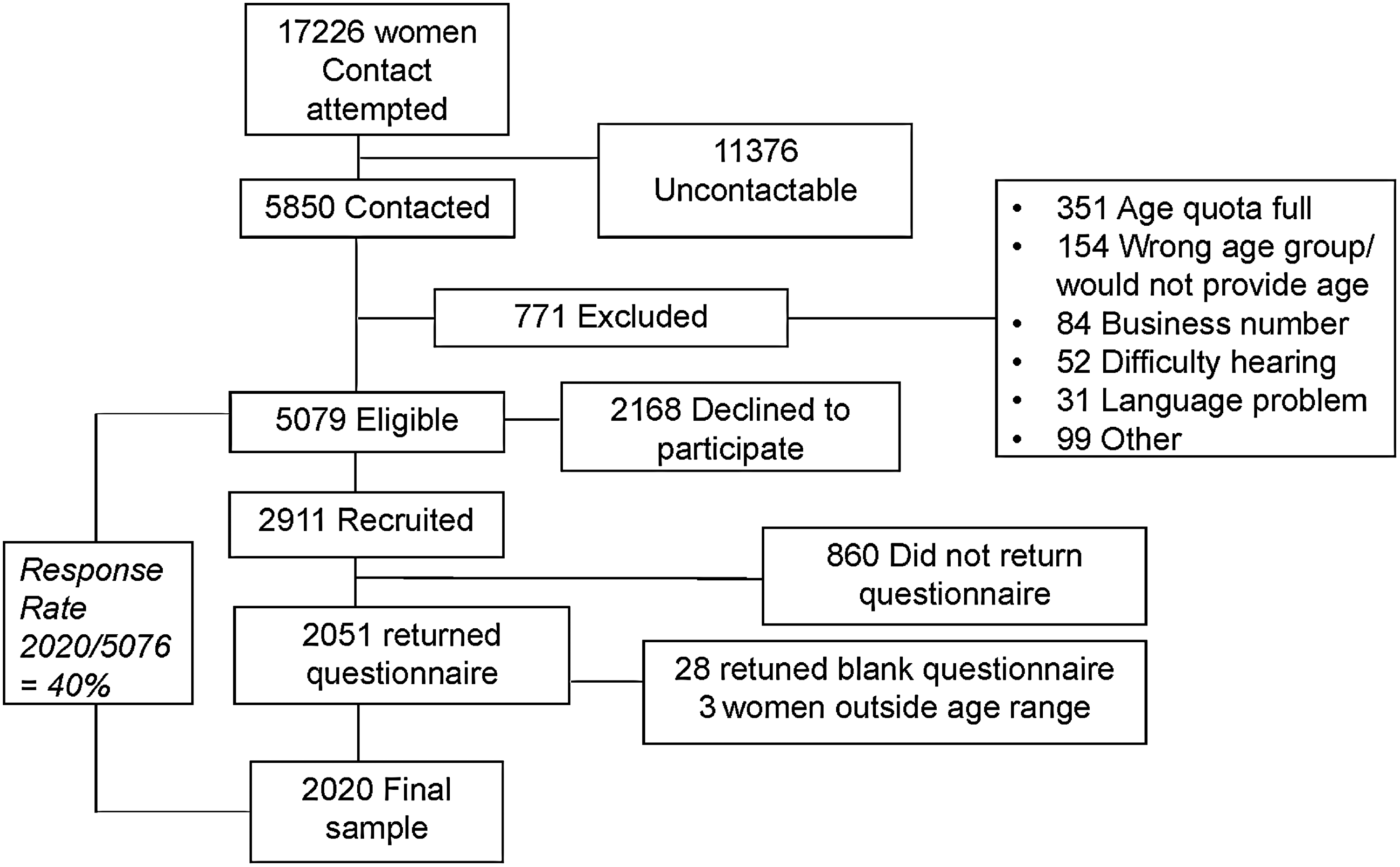
Participant flow.
Study variables
Participants completed a comprehensive health and behavior questionnaire that included a number of validated self-report instruments.
Current depressive symptoms were assessed using the Beck Depression Inventory-II (BDI), a 21-item self-report instrument, validated in clinical and community samples. 21 The BDI has a total score of 63. Based on validated cut-points, women were classified as having as minimal–mild (<20) or moderate–severe (≥20) depressive symptoms. 21
The participants were classified as being premenopausal, perimenopausal, or postmenopausal on the basis of published algorithms that take into account age, menstrual bleeding pattern, gynecological history, and the use of systemic hormone therapy. 22,23
The degree of bother caused by menopausal symptoms was determined by the Menopause-Specific Quality of Life Questionnaire (MENQOL), a validated self-report instrument. 24 The VMS domain of the MENQOL comprises three questions about the degree of bother caused by night sweats, hot flashes, and sweating. Participants rated each symptom from 1 (no symptom) to 8 (extremely bothersome). The VMS domain score was calculated as the mean score of these three questions. 24 We further divided the domain score into two levels: no or mildly bothersome symptoms (score 1–≤5) and moderate to severely bothersome symptoms (hereafter referred to as moderate-severe) if VMS were rated more than the midpoint of the scale (score >5–8). 19 We have successfully used this approach in multiple other publications. 7,19,25
Participants were asked if they were current smokers (yes/no), whether they drank alcohol (yes/no), and the frequency and quantity of alcohol consumption. Binge drinking was defined as consuming ≥4 standard alcoholic drinks on one occasion. 26
The study questionnaire also provided women with a comprehensive list of psychotropic medications. Participants were asked to identify any medication they had used in the last 4 weeks. The medications were classified as follows: antidepressants (paroxetine, mirtazapine, citalopram, venlafaxine, amitriptyline, escitalopram, fluvoxamine, desvenlafaxine, duloxetine, fluoxetine, agomelatine, and sertraline); anxiolytics (lorazepam, temazepam, oxazepam, diazepam, and alprazolam); antipsychotics (chlorpromazine, risperidone, quetiapine, and olanzapine); and mood stabilizers (lithium, sodium valproate, lamotrigine, and carbamazepine). Mood stabilizers (other than lithium) were excluded if the woman had a current neurological disorder due to the possibility that the medication was being used to treat another condition, such as epilepsy.
Systemic menopausal hormone therapy (MHT) was defined as use in the last 4 weeks of oral, transdermal, or implanted estrogen-only therapy, estrogen–progestin therapy, tibolone, the combined oral contraceptive pill, compounded estrogen, and compounded progesterone.
Women were asked if they felt their housing was financially secure, with those reporting “no” or “uncertain” classified as having insecure housing. They were also asked if they were a carer for a family member with special needs.
Statistical analysis and sample size
The statistical power of the study was based on an estimate of prevalence of moderate–severe VMS of 30%, 27 with a 95% confidence interval (CI) of ±2%. From this it was calculated that 2,000 participants with completed questionnaires were required. 20 Descriptive analysis was performed using numbers and percentages for categorical data and mean and standard deviation (SD) for continuous data.
A logistic regression model was constructed to test whether moderate–severe VMS were associated with moderate–severe depressive symptoms, after taking into account demographic and other factors known to be associated with depressive symptoms (age, body mass index [BMI], education level, partnership status, employment status, housing insecurity (as a measure of financial distress), and being a carer for a family member with special needs). All factors significant at p < 0.1 in univariate analysis were included in the final model. Menopausal stage was not included in the regression model. As menopause is the cause of VMS, including both in the model would create redundancy. MHT use was not included in the model as it was not significant at the univariate level (p = 0.52). All analyses were performed using STATA version 12.0 (StataCorp). All tests were two sided and the alpha level was set at 0.05 for all statistical tests.
Results
Sample description
A total of 5,850 women were contacted, and of these, 771 were ineligible (Fig. 1). Two thousand nine hundred eleven of the 5,079 eligible women agreed to participate, and 2,023 completed questionnaires were returned. Of these, 3 were from women outside the targeted age range, leaving a final study sample of 2,020 women. The response rate was calculated as 40% (2,020/5,076) using the American Society of Public Opinion Research response rate calculator version 3.1. 28
The study sample was representative of Australian women aged 40–65 years, based on several demographic characteristics. 19,29 Most women were white (93.9%), partnered (67.2%), in paid employment (63.1%), and had tertiary or vocational education (58.7%) (Table 1). Five hundred twenty-nine (26.2%) of the 2,020 women were premenopausal, 382 (18.9%) perimenopausal, and 1,109 (54.9%) postmenopausal. VMS were classified as moderate–severe VMS for 267 women (13.3%).
Excludes women with a neurological disorder who are taking an antiepileptic (sodium valproate, lamotrigine, carbamazepine).
BDI, Beck Depression Inventory; SD, standard deviation.
Current systemic MHT use was reported by 120 (5.9%) of all women. Compared to nonusers, women who used MHT were more likely to be postmenopausal (84.8% vs. 54.2%, respectively, p < 0.001) and to be aged 50–59 years (65.2% vs. 40.4%, respectively, p = 0.001).
The prevalence of moderate–severe depressive symptoms
The prevalence of moderate–severe depressive symptoms was 14.7% (95% CI: 13.2–16.3) among the whole group.
Women with moderate–severe VMS, compared to those with no/mild VMS, had a higher prevalence of moderate–severe depressive symptoms (29.6%, 95% CI, 24.0–35.1 vs. 12.4%, 95% CI, 10.8–14.0, p < 0.001).
Factors associated with moderate–severe depressive symptoms
In univariate analysis, compared to women with no/mild VMS, the odds of experiencing moderate–severe depressive symptoms were higher in women with moderate–severe VMS (odds ratio [OR] 2.96, 95% CI, 2.19–4.00, p < 0.001) (Table 2). Other factors that significantly increased the odds of moderate–severe depressive symptoms at the univariate level were higher BMI, being unpartnered, being a carer for a family member with special needs, having insecure housing, and not being in paid employment. Being more educated and older reduced the odds of moderate–severe depressive symptoms.
Moderate
P < 0.001.
P < 0.01.
p < 0.05.
CI, confidence interval; SD, standard deviation.
When adjusted for all the above factors, compared to women with no/mild VMS, moderate–severe VMS (adjusted OR 2.80, 95% CI, 2.01–3.88, p < 0.001) remained significantly associated with moderate–severe depressive symptoms. Other factors that remained significantly associated with an increased risk of moderate–severe depressive symptoms in the adjusted analyses were housing insecurity (adjusted OR 3.04, 95% CI, 2.17–4.25, p < 0.001), not being in paid employment (adjusted OR 1.83, 95% CI, 1.37–2.45, p < 0.001), BMI of 40 kg/m2 or more (adjusted OR 2.18, 95% CI, 1.36–3.49, p = 0.001), and being unpartnered (adjusted OR 2.06, 95% CI, 1.57–2.71, p < 0.001). Being 60 years or older remained associated with a significantly decreased risk of moderate–severe depressive symptoms (adjusted OR 0.40, 95% CI, 0.26–0.63, p < 0.001). Although MHT use was not significant in the univariate analysis, given that MHT has the capacity to affect VMS and depressive symptoms, for completeness we ran a version of the model that also included MHT, however, the results were unchanged (results not shown).
Psychotropic medications, smoking, and alcohol consumption
Four hundred ninety-one women (24.3%) reported use of at least one psychotropic medication in the prior 4 weeks. Antidepressants were the most commonly used psychotropic (19.0%) followed by anxiolytics (4.1%), antipsychotics (1.6%), and mood stabilizers (0.9%, when antiepileptic medications taken by women with a neurological condition were excluded). Thirteen women (0.6%) reported using an antidepressant to treat VMS. Current smoking was reported by 282 women (14.0%) and 1,482 women (73.4%) reported consuming alcohol. Five hundred four women (25.0%) reported binge drinking, at least once per month, and 223 (11.0%) reported binge drinking at least once per week.
Women with moderate–severe depressive symptoms, compared to those with minimal–mild depressive symptoms, were more likely to use psychotropic medications (48.9%, 95% CI, 43.1–54.8 vs. 20.1%, 95% CI, 18.2–22.1, p < 0.001), smoke (25.9%, 95% CI, 20.8–30.9 vs. 12.2%, 95% CI, 10.6–13.7, p < 0.001), and binge drinking at least weekly (15.1%, 95% CI, 11.0–19.2 vs. 10.3% 95% CI, 8.8–11.7, p = 0.015).
Discussion
This large study of randomly recruited, community-based women aged 40–65, clearly demonstrates that moderate–severely bothersome VMS are independently associated with moderate–severe depressive symptoms. The observed association was retained after controlling for age, BMI, partnership status, education, employment status, carer status, housing insecurity, and use of MHT.
Previous investigators have assessed the presence or frequency of VMS. 2,5,9 –11,30,31 However, the prevalence of any VMS in midlife women is very high, ranging between 42.1% and 74.2% of peri- and postmenopausal women in our cohort. 7 Such ubiquity of VMS renders it difficult to interpret associations in a meaningful way. Focusing on moderate–severe VMS is more clinically relevant, as these are the women more likely to present to their doctors.
This study also used a far higher threshold for depressive symptoms than prior studies. The cutoff used in the current study of BDI ≥20 selects women with moderate–severe symptoms. A study comparing the BDI to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV Axis I Disorders-Clinician Version, found a cutoff of ≥15 to have 65% sensitivity and 97% specificity for a current episode of major depression. 32 Many past studies have relied on the Center of Epidemiological Studies Depression Scale (CES-D) and have classified women with a CES-D score of ≥16 as having depressive symptoms, 3,9,33 although such a score incorporates many women with mild symptoms or distress as opposed to depression. 34 A BDI score ≥20 is approximate to a CES-D score of ≥25. 35 The Harvard Study of Mood and Cycles found that a CES-D score >24 had a high sensitivity and specificity for major depressive disorder. 2 A study of community dwelling adults found a CES-D score ≥25 to have a high sensitivity and specificity for “clinically relevant depression” defined as major depressive disorder, dysthymia, or subthreshold depression compared to a clinical interview. 13
Thus, this study by using a higher threshold for depressive symptoms provides insights into women with clinically relevant symptomatology. By demonstrating an association between moderate–severe VMS and moderate–severe depressive symptoms, this study adds further weight to the notion of a shared etiology between VMS and depression. In addition to improving VMS, estrogen therapy may improve mood in early menopause. 36
The use of antidepressants by 20% of women in the study is consistent with results of a recent study of 111,705 Australians aged 45 years and older, in which 23% of women had been dispensed an antidepressant within the previous 19 months. 37 In a global context, antidepressant use in Australia is high, being second only to Iceland in the Organisation for Economic Cooperation and Development. 38
The other factors found to be independently associated with an increased likelihood of depressive symptoms, namely morbid obesity and insecure housing, and older age being associated with a decreased likelihood, are noteworthy.
The major strength of this study is the representativeness of the community-based sample. Characteristics of Australian women aged 40–65 in the 2011 national census that are very similar to our sample include ethnicity (white, 92% vs. 93.9% in our sample), being partnered (70% vs. 67.2%), education beyond high school (56.8% vs. 58.7%), and being in paid employment (62.5% vs. 63.1%). 28
A potential study limitation is the reliance on self-report measures. However, the BDI is validated for epidemiological research. Other potential limitations were the inability to compare demographics of respondents and nonrespondents due to privacy guidelines and the reliance on women able to complete the questionnaire in English. This was unlikely to have a meaningful effect on outcomes as the rate of English literacy in Australian women exceeds 96%. 39
In conclusion, moderate–severe VMS are independently and significantly associated with moderate–severe depressive symptoms. Among Australian women aged 40–65, both these symptoms are common, as is the use of antidepressant medication.
Footnotes
Acknowledgments
We thank the women who participated in our study. This study was funded by a grant from the BUPA Health Foundation and a contribution in kind from Roy Morgan Research. S.R.D is an NHMRC Research Fellow (grant number 1041853). R.W. has an NHMRC postgraduate scholarship. P.G. was supported by an Australian Postgraduate Association scholarship. The funding organizations played no role in the design or conduct of the study, data collection, analyses, or preparation of the manuscript.
Author Disclosure Statement
S.R.D. and R.J.B. have research grant support from Lawley Pharmaceuticals. S.R.D. has received honoraria from Abbott Australia and Pfizer Pharmaceuticals. All other authors declare no conflict of interest.