
Abstract
Background:
Vasomotor symptoms are the most commonly reported menopausal symptoms. Hormone therapy has been widely used to relieve postmenopausal symptoms. With studies suggesting an increased risk of cardiovascular events and breast cancer with oral hormone therapy use, there has been reluctance to use it. The transdermal estrogen patch provides relief from menopausal symptoms. However, there are limited data on mortality and cardiovascular outcomes, while on the transdermal estrogen patch.
Methods:
An extensive search in Cochrane and PubMed databases was conducted up to February 2016. The selection criteria included healthy, peri-, and postmenopausal women between the ages of 50 and 79 and should have received transdermal estrogen therapy. The relationship between estrogen patch use and cardiovascular outcomes was analyzed. Six articles met the criteria and were included.
Results:
We found some evidence suggestive of protective cardiovascular effects with transdermal estrogen therapy with a decrease in the risk of stroke and no increase in the risk of coronary heart disease, death, or myocardial infarction.
Discussion:
This is one of the first systematic reviews addressing the association of transdermal estrogen patch use on cardiovascular outcomes. We found some evidence suggestive of a possible protective cardiovascular effect with transdermal estrogen therapy. Further randomized controlled studies are needed with a longer duration of follow-up, to study the cardiovascular effects of transdermal estrogen patches.
Introduction
V
Hormone therapy (HT) has been widely used to relieve postmenopausal symptoms. It involves administering synthetic hormones, estrogen, and/or progesterone, to alleviate postmenopausal symptoms. HT can be administered locally (creams or rings) and systemically (oral, transdermal patch or gels, and implants). In addition, it can contain estrogen only or a combination of estrogen and progesterone. However, with studies suggesting an increased risk of cardiovascular events and breast cancer with oral HT use, there has been an increased reluctance to use it. The Women's Health Initiative (WHI) study, in 2002, was stopped early because HT was linked to a slightly increased risk of stroke and heart disease. 4 A comprehensive report on the WHI published in 2013 concluded that for all-cause mortality and myocardial infarction (MI), conjugated equine estrogen (CEE) had more favorable results in women aged 50–59 years compared to older women. 5 In the CEE trials the hazards ratio (HR) for all-cause mortality in women aged 50–59 years was 0.70 (0.46–1.09) compared to HR 1.1 (1.01–1.21) in women aged 60–79 years. 5 The Revised Global Consensus Statement on Menopausal Hormone Therapy states that standard-dose estrogen only menopausal HT may decrease the risk of MI and all-cause mortality when started in postmenopausal women before 60 years of age or within 10 years after menopause. 6 In addition, the U.K. National Institute for Health and Care Excellence (NICE) states that HT does not increase cardiovascular risk when started in women under 60 years of age. 7,8 The transdermal estrogen patch provides relief from menopausal symptom. There are limited data on mortality and cardiovascular outcomes, while using the transdermal estrogen patch.
Transdermal estradiol administers a more physiologic dose of estrogen. Its benefit over oral estrogen is that it bypasses the first pass metabolism in the liver and hence may have a safer profile. It does not raise C-reactive protein (CRP) levels (a marker of inflammation that has been found to be a risk factor for cardiovascular disease [CVD]) while oral estradiol does. 9 In addition, compared to oral conjugated estrogen, transdermal estrogen does not reduce IGF-1 levels (an anti-inflammatory group factor), reduces serum triglyceride levels, and does not promote hepatic protein synthesis. 10 Our aim was to conduct a systematic review to study the effect of the estrogen patch on mortality and cardiovascular outcomes.
Objectives
To assess the effects of transdermal estrogen patch use on mortality and cardiovascular outcomes in postmenopausal women.
Methods
An extensive search in Cochrane and PubMed databases was conducted up to February 2016, independently by two investigators (P.B and D.M). Search terms used are delineated in Table 1. In addition to index terms, such as MeSH, keywords were searched as well. The entire search strategy is shown in Table 1.
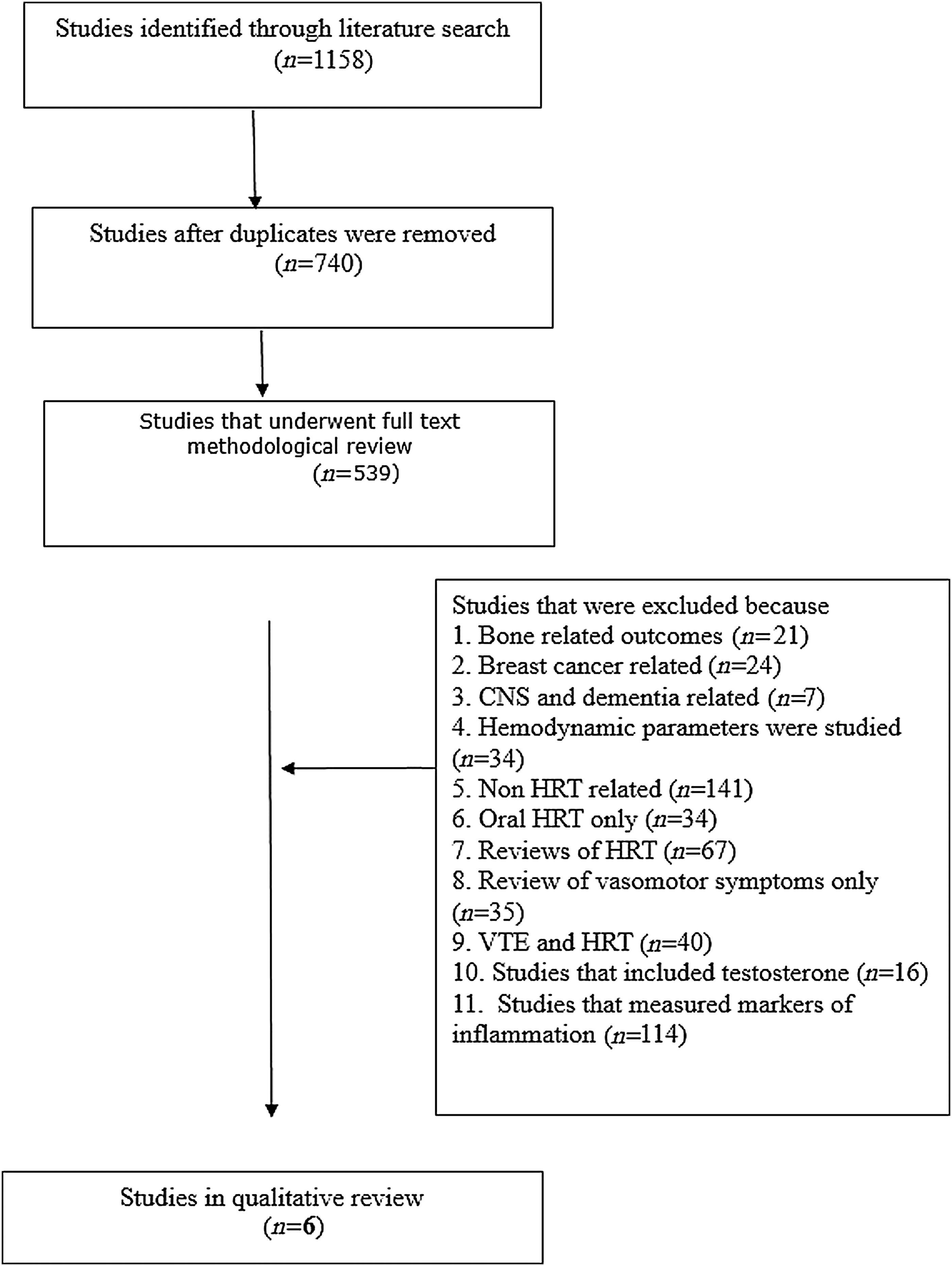
We included studies that were available as full text articles and reviewed the references of previously published articles. Results were limited to clinical trials and observational studies. No language limits were applied. We identified 1,158 articles (full text articles, abstracts, and reviews). Summary of the methods is presented in Figure 1. The selection criteria included healthy peri to postmenopausal women between the ages 50–79 and should have received transdermal estrogen HT. The relationship between estrogen patch use and cardiovascular outcomes was analyzed. Six articles met the selection criteria and were included. A meta-analysis was not possible due to the heterogenecity of the studies in terms of design and measured outcomes.
Search methods.
Results
The six articles that were included in the systematic review were published between 2000 and 2014 in four countries: United Kingdom (UK), United States (US), Denmark, and Italy. Three were cohort studies, while the remaining was case–control. All the studies were designed to assess cardiovascular outcomes related to the use of HT. The studies focused on perimenopausal to postmenopausal women. Information related to study design, year of publication, study population, inclusion and exclusion criteria, length of follow-up, statistical values, and measured cardiovascular outcomes was collected. The summary of the six articles is presented in Table 2.
CKD, chronic kidney disease; CVD, cardiovascular disease; HT, hormone therapy; IHD, ischemic heart disease; MI, myocardial infarction; NA, not applicable; VTE, venous thromboembolism.
Effect on MI
In a Danish cohort of 698,098 healthy women, aged 51–69, followed for a period of 6 years, it was found that there was no increase in the risk of MI with hormonal therapy use compared with never users. 11 There was a significantly lower risk with dermal estrogen use compared to oral unopposed estrogen use (p = 0.04). 11 There were 24 cases of MI reported with dermal estrogen use; relative risk (RR) 0.62 (confidence interval [95% CI] 0.42–0.93), while there were 264 cases associated with oral estrogen use; RR 0.98 (0.67–1.12). 11
Varas-Lorenzo et al. performed a nested case–control study of 164,769 healthy postmenopausal women, aged 50–74, followed for 5 years. The aim was to study the incidence of acute MI. They found a 28% decrease in the risk of acute MI in current/recent users of HT compared to nonusers. The ratio of cases to controls was 1:6 and there were 22 cases of MI in transdermal estrogen users and 63 in oral estrogen users. 12 Odds ratio for transdermal estrogen was 0.75 (0.47–1.21), while that of oral estrogen users was 0.85 (0.53–1.34). 12 The results for transdermal estrogen was nonsignificant because there were only a few users. The authors concluded that there was no significant difference in MI between oral and transdermal estrogen therapy, at medium to high doses of both. 12 For oral estrogens, low dose was <0.625 mg, medium dose was 0.625 mg, and high dose was >1.25 mg. For transdermal estradiol, low dose was 25 μg, medium dose was 50 μg, and high dose was 100 μg. 12
A nested case–control study was conducted in the United Kingdom, by de Vries et al., on a cohort of women aged 52–74 years, with no history of heart disease. They studied the risk of MI in HT users and the differences in that risk based on the HT product used. The duration of follow-up was 7 years. The authors concluded that MIs were less fatal and there was a reduced risk estimate for MI in women who used HT compared to nonusers. For transdermal estrogen the odds ratio was 0.66 (95% CI 0.49–0.88) and for oral estrogen the odds ratio was 0.77 (95% CI 0.66–0.90). 13 Oral and transdermal estrogen were associated with a significant decrease in MI, but there was no difference in protection between the two. 13
Effect on stroke
The WHI-Observational Study (WHI-OS), a cohort of 93,676 postmenopausal women, aged 50–79, was conducted in the United States of America. The follow-up was for 10.4 years. In the cohort, there were 2,187 women who used the transdermal estrogen patch. The authors found a lower risk of stroke with transdermal estrogen compared with conventional oral estrogen; HR 0.87 (95% CI 0.55–1.38). 14 There were 17 cases of stroke in the transdermal group, 36 in the low dose CEE group, and 297 cases in the conventional dose CEE group. The study population was large and diverse, but had limited statistical power, because of the low number of transdermal users. The study concluded that transdermal estrogen was associated with a lower risk of stroke compared to oral conventional dose estrogen therapy, 14 but was not statistically significant.
In a population based nested case–control study, conducted by Renoux et al. in the United Kingdom, it was determined that the use of low dose transdermal estrogen did not increase the risk of stroke. The cohort was 870,286 women aged 50 to 79 years. The duration of follow-up was 6.7 years, and 15,710 cases of stroke were detected. The rate ratio was 0.81 (0.62–1.05) in low dose transdermal estrogen users. 15 Only new users of HT were included. 15 Age at menopause, socioeconomic status, and education were potential confounders that were not adjusted for. However the outcome of stroke was not adjudicated as the investigators did not have access to the patients' charts. 15
Effect on major coronary heart disease and CVD mortality
A cohort study was conducted in Italy on 78,875 women aged 45 to 65. The duration of the study was 5 years. The outcomes measured were hospitalizations from ischemic heart disease (IHD) and CVD. For IHD the HR was 0.59 (95% CI 0.34–0.82) and for coronary heart disease (CHD) the HR was 0.39 (95% CI 0.18–0.82). 15 There was a decreased risk of hospitalization if HT (as a whole, both transdermal and oral) was taken for >3 years compared to 6 months or less. In conclusion, there was a decreased risk of CHD and CVD among long-term transdermal estrogen users. 16 There is a risk of bias because of errors in identification, coding, and compliance. Data on confounders as smoking, alcohol use, and physical exercise were not available. 16
The WHI-OS study concluded that there was a lower risk of major CHD in transdermal estrogen users, compared with conventional dose oral estrogen users; HR 0.63 (95% CI 0.37–1.06), but was not statistically significant. 14 There were 18 cases of CHD in the transdermal group, 22 cases in the low dose CEE, and 324 cases in the oral conventional CEE group. 14 For CVD mortality, there was a beneficial effect of hormonal therapy, but no difference between transdermal and conventional oral therapy; HR 0.94 (95% CI 0.50–1.74). 13
Discussion
CVD is the leading cause of mortality and morbidity in women. According to the SWAN study, frequent vasomotor symptoms (>6 days in 2 weeks) lasted an average of 7.4 years during the menopausal transition. 17 The protective effect of estrogen is one contributing factor to the later onset of CVD in women, as evidenced by equal rates of CVD in men and women postmenopause. 18 It was believed for a long time that hormonal treatment could prevent cardiovascular risk, but the WHI 14 and heart and estrogen/progestin replacement study (HERS) 19 studies refuted this concept. However, post hoc analysis of the above studies has shown evidence of a vascular benefit if HT is taken early in menopause. 17
There are a number of studies on the role of transdermal hormonal therapy on inflammatory biomarkers. A study by Shifren et al. concluded that transdermal estrogen had a minimal effect on inflammatory markers like CRP, E-selectin, and P-selectin, compared with oral CEE. 10 A study by Sumino et al. has shown that the patch reduces carotid artery wall thickness. 20 Literature on the association of the transdermal hormonal patch with cardiovascular outcomes is limited. In view of the burden of menopausal vasomotor symptoms and the limited role for oral HT, it is important to determine the long-term effects of transdermal HT to guide therapy for relief of symptoms.
As discussed above, transdermal estrogen therapy seems to have a beneficial effect on cardiovascular outcomes. It has a cardioprotective effect, significantly reducing the incidence of MI compared with nonusers 21 and decreasing the incidence of stroke compared to oral estrogen users. 22 In addition, there was a lower risk of major CHD in transdermal users, compared to oral estrogen users. 14 The size of the study population was large in all studies included in this review.
However there are limitations of this review. First, literature was limited by lack of data on postmenopausal status. 11 Studies that focus on cardiovascular risk with transdermal estrogen use only are not existent. Of note, only two studies studied the relationship of the patch to the incidence of stroke. 14,15 In most studies, the number of transdermal estrogen users was small and hence had a wide confidence interval. We know that smoking, alcohol consumption, physical activity, obesity, and body weight have an effect on cardiovascular outcomes. Some studies that were included in this review did not have information on these risk factors, and hence, there was confounding. 11,12,16 Some studies did not have information about postmenopausal status. 11 None of the studies are randomized controlled trials and we need studies with longer duration of follow-up. We focused on studies with clinical end points which are relevant for clinical practice. There is a need for prospective randomized studies on peri- and postmenopausal women focusing on cardiovascular outcomes with transdermal HT.
Conclusions and Implications
This is the first systematic review studying the association of transdermal estrogen patch use on cardiovascular outcomes. We found some evidence suggestive of a protective cardiovascular effect with transdermal estrogen therapy with a decrease in the risk of stroke and no increase in the risk of CHD death or MI. The effects are found to be dependent on the duration of use and the time frame; use early in menopause versus later. We need more studies in the future, especially randomized controlled trials, to study the cardiovascular effects of transdermal estrogen patches, in a diverse population so as to decrease the burden of limiting vasomotor symptoms.
Authors' Contributions
Conception and design: P.B. and D.M.; Drafting of the article: P.B., A.S., and D.M.; Critical revision of the article for important intellectual content: A.S. and D.M.; and Final approval of the article: D.M.
Footnotes
Author Disclosure Statement
No competing financial interests exist.