
Abstract
Background:
In the United States, between one-third and two thirds of postmenopausal women do not begin treatment with a prescription osteoporosis medication after a diagnosis of osteoporosis. The objective of this study was to understand the reasons for this lack of treatment.
Materials and Methods:
Online physician and patient surveys were administered in 2013. The physician survey included a chart review of untreated postmenopausal women recently diagnosed with osteoporosis and gathered data on physicians' practices regarding the management of osteoporosis in postmenopausal women. The patient survey was given to untreated postmenopausal women with a recent osteoporosis diagnosis.
Results:
The physician survey was completed by 224 physicians, who also reviewed 811 patient charts. A total of 165 patients completed the patient survey. In the chart review, physicians reported that 19% of the postmenopausal women they diagnosed with osteoporosis were not prescribed an osteoporosis medication. The patient declined a physician's recommendation for pharmacological treatment in 81% and 52% of cases in the physician and patient surveys, respectively. The most frequent reasons for physicians not recommending treatment were: low calcium and/or vitamin D levels, patients potentially at risk of medication side effects, pre-existing gastrointestinal problems, and polypharmacy. The most frequent reasons for patients deciding against treatment were: concerns about side effects, considering nonprescription options and behavioral modifications, and questioning the potential benefit of taking the medication.
Conclusions:
Patients decided against pharmacological treatment of newly diagnosed osteoporosis in at least half of the cases of nontreatment. The principal reasons for not being treated with a prescription medication, given by both physicians and patients, were that there were alternatives and concern about the risks of prescription medications.
Introduction
O
Recent estimates for the percentage of U.S. postmenopausal women not initiating treatment with an osteoporosis medication after a diagnosis of osteoporosis range from 35% to 64%. 6 –9 The reasons for patient and physician nontreatment are not well understood. The aim of this study was to understand the reasons for not initiating osteoporosis treatment among postmenopausal women in the United States who have been newly diagnosed.
Materials and Methods
Study design
The Study of Osteoporosis UNder-treatment post-Diagnosis (SOUND) is a cross-sectional study consisting of two separate online surveys completed by physicians and patients to obtain perspectives on the reasons for nontreatment of postmenopausal women who were newly diagnosed with osteoporosis (see Appendix 1 for survey questions). In addition to responding to questions about their management of patients with osteoporosis, physicians reported information they extracted from the medical charts of three to five patients who were postmenopausal women, recently diagnosed with osteoporosis in the past 3–12 months, and who had not received a prescription for an osteoporosis medication. Respondents to the patient survey were self-reported as postmenopausal women, with a recent diagnosis of osteoporosis, without a prescription for an osteoporosis medication. The surveys were conducted from August 16, 2013 to September 4, 2013.
Study participants
Physicians and patients were recruited from national panels, maintained by M3 Global Research. The panels consist of individuals who have opted in to the panel to participate in online surveys. These participants are recruited from multiple sources, including coregistration from partner websites, trade shows, conferences, targeted e-mails, and telephone recruitment.
Study participants: physician survey
Invitations to participate in an online survey were sent by e-mail on August 16, 2013 to 5,289 physicians practicing in Primary Care, General Practice, Family Practice, Internal Medicine, Gynecology, Rheumatology, or Endocrinology. The time window for receiving responses was held open until the number of completed questionnaires reached the predetermined target sample size of 220 (the sample size was determined to be sufficient to provide a confidence level of 95% with a 10% margin of error for both primary care providers and specialists). The e-mails described the study as a 45-minute survey to determine how osteoporosis is managed in postmenopausal women diagnosed with osteoporosis. An honorarium of $90 was offered to physicians who completed the survey.
Respondents were required to answer several screening questions to determine their eligibility to participate in the survey. Participating physicians were required to be practicing in one of the following specialties: Primary Care, General Practice, Family Practice, Internal Medicine, Gynecology, Rheumatology, or Endocrinology; to have been in practice for 2–30 years; to spend at least 65% of their professional time in clinical practice; to have seen or treated at least five postmenopausal women in the previous 12 months; to have at least three current patients who were postmenopausal women with a diagnosis of osteoporosis, who were not receiving an osteoporosis medication; to have prescribed osteoporosis medications in the past 12 months; to have no current consulting or commercial ties with a pharmaceutical company; and to have not participated in a market research study of osteoporosis in the previous 3 months.
Study participants: patient survey
Invitations were sent by e-mail on August 19, 2013 to 11,533 women over the age of 55 years in the patient panel. The target sample size was 160 completed surveys to allow for adequate sample sizes within patient subgroups (such as patients with a prior fracture). The survey was closed when the number of completed questionnaires reached the predetermined target sample size. The patient survey was expected to take ∼30 minutes to complete.
Patients had to answer several preliminary screening questions to determine their eligibility to participate. Patients were required to be a postmenopausal woman; at least 55 years of age; to have been diagnosed with osteoporosis in the previous 3–12 months; to not have a current prescription for an osteoporosis medication; and to have not been diagnosed in the past 12 months with a condition that might affect cognition, that is, Alzheimer's disease, mild cognitive impairment, dementia, Parkinson's disease, or Huntington's disease. No attempt was made to recruit patients whose charts were reviewed in the physician survey.
Participant screening
Both physicians and patients were screened online before initiating the surveys. All information was self-reported. The screening questions were reviewed by multiple reviewers to ensure that it did not lead participants to give biased or socially desirable answers. Those who did not meet all the screening criteria were not allowed to participate. Additionally, physicians had to answer a set of screening questions for each patient chart to ensure the accurate selection of patient for chart reviews.
Physician and patient surveys
Two surveys were developed and administered online, a physician survey and a patient survey. The surveys were developed through a targeted literature review and initial qualitative interviews with eight physicians and four patients. The surveys were pilot tested through one-on-one telephone interviews with four physicians and two patients to ensure the comprehensiveness, clarity, and relevance of the survey. Feedback from the initial physician and patient qualitative interviews and pilot tests were used to ensure that respondents understood and were comfortable with the questions regarding reasons for nontreatment.
Questions in the physician survey consisted of two sections, the first contained questions about the physician's perceptions on screening, diagnosis, management, and treatment of osteoporosis (see Appendix 1 for survey questions reported here) and the second included a patient chart review. For the chart review, physicians were asked to select at least three charts for patients who were postmenopausal women, diagnosed with osteoporosis 3–12 months before the date of the survey, and not yet prescribed an osteoporosis medication. Each patient's clinical characteristics, method of diagnosis, osteoporosis risk factors, and comorbidities were recorded. After reviewing each chart, physicians were asked to provide their reasons for not prescribing an osteoporosis medication.
The patient survey contained questions about the patient's demographics, clinical characteristics, management of osteoporosis, and the reasons why she was not treated with a prescription medication for osteoporosis (see Appendix 1 for survey questions).
Study definitions
The definition of pharmacological treatment for osteoporosis in the physician survey was restricted to U.S. Food and Drug Administration-approved prescription medications indicated for the treatment of postmenopausal osteoporosis: alendronate, ibandronate, risedronate, zoledronic acid, raloxifene, teriparatide, denosumab, and strontium ranelate. Physicians were asked to exclude nonprescription calcium or vitamin D supplements, calcitonin, and estrogen therapy/hormone therapy from their definitions of osteoporosis medications for this study.
The primary care physician category included primary care physicians, general practitioners, family physicians, internal medicine specialists, and geriatricians. A woman was considered to be postmenopausal when she had not had her menstrual cycle for 12 months. Premature menopause was defined as menopause before age 40. Pre-existing gastrointestinal (GI) problems were defined as gastroesophageal reflux disease, dyspepsia, dysphagia, esophagitis, and GI bleeding. Limited mobility was defined as a patient who was dependent on ambulation, could not sit up for 30 minutes, or could not walk or bear weights. Renal insufficiency was defined as a creatinine clearance <35 mL/minute. Ovarian failure was defined as loss of function of the ovaries before age 40.
Ethics
The study was approved by a central Institutional Review Board (Schulman Associates IRB). All data were anonymous, and the authors were blinded to the names and contact information of respondents to the physician and patient surveys.
Data analyses
Descriptive analyses were conducted to evaluate the survey responses using SPSS version 19.0. A chi-square test was used to determine the statistical significance of differences in categorical variables. Student's t-test was used for continuous variables. A p value of <0.05 was considered statistically significant.
Results
Physician characteristics
The physician survey and chart review was conducted between August 16 and September 4, 2013. The physician survey and chart review was completed by 224 physicians, of whom 103 (46.0%) were primary care providers, general practitioners, family physicians, internal medicine specialist, or geriatricians, 41 (18.3%) were gynecologists, 40 (17.9%) were rheumatologists, and 40 (17.9%) were endocrinologists (data not shown). The physicians included in the study practiced in 39 states; 16.5% of the physicians practiced in the West; 6.7% in the Southwest; 21.4% in the Midwest; 26.3% in the Southeast; and 29.0% in the Northeast (data not shown). Seventy percent of physicians responding to the survey were male and had, on average, 16 years of experience in clinical practice (data not shown).
Patient characteristics
Physicians provided data from 811 charts of postmenopausal women not prescribed an osteoporosis medication following a diagnosis of osteoporosis. The patient survey was conducted between August 19 and September 19, 2013, during which time 165 patients completed questionnaires were received from women not prescribed an osteoporosis medication (this number is greater than the predetermined target sample size because five patients were in the process of completing the survey when the target sample size was reached).
The characteristics of both sets of patients are presented in Table 1. These patient populations differed in several demographic and other characteristics. Patients included in the physician chart review were younger (modal age category 56–60 years in the physician chart review vs. 61–65 in the patient survey) less predominately Caucasian (67% vs. 86%), were more frequently diagnosed with a bone mineral density (BMD)/dual-energy X-ray absorptiometry (DXA) scan (90% vs. 75%), had less time since the osteoporosis diagnosis (6.3 months vs. 8.7 months), and lower frequencies of most comorbidities, and had lower rates of various risk factors, including limited dairy/calcium intake (30% vs. 53%), height loss (16% vs. 58%), previous fracture (7% vs. 47%) than patients in the patient survey (Table 1).
Values are presented as N (%) unless indicated otherwise.
Source: physician and patient survey questions D4 and A2, respectively.
Source: physician and patient survey questions D5 and E1, respectively.
Source: physician and patient survey questions D10a and B8, respectively.
Responses sum to greater than 100% as patients could have had more than one test to diagnose osteoporosis.
Source: physician and patient survey questions D2 and A5, respectively.
Source: physician and patient survey questions D6 and A4, respectively.
Responses sum to greater than 100% as patients could have more than one risk factor/comorbidity.
Source: physician and patient survey questions D7 and B2/B3, respectively.
Previous fractures included fractures of extremities (foot, toes, fingers), hip, wrist, vertebral, femoral, and other fractures.
BMD, bone mineral density; BMI, body mass index; DXA, dual-energy X-ray absorptiometry; FRAX, Fracture Risk Assessment Tool; N/A, not applicable; NS, not significant.
Reasons for physicians not recommending and patients declining an osteoporosis medication prescription
Physicians reported that, of the 811 patients whose charts they reviewed, 81% had declined the physician's recommendation for an osteoporosis medication prescription, whereas 19% had not been given a recommendation for a prescription (Fig. 1). These percentages did not differ significantly by physician specialty. In contrast, 52% of respondents to the patient survey reported they had declined their physician's recommendation for an osteoporosis medication prescription, whereas 48% reported they had not been given a recommendation for a prescription (Fig. 1).
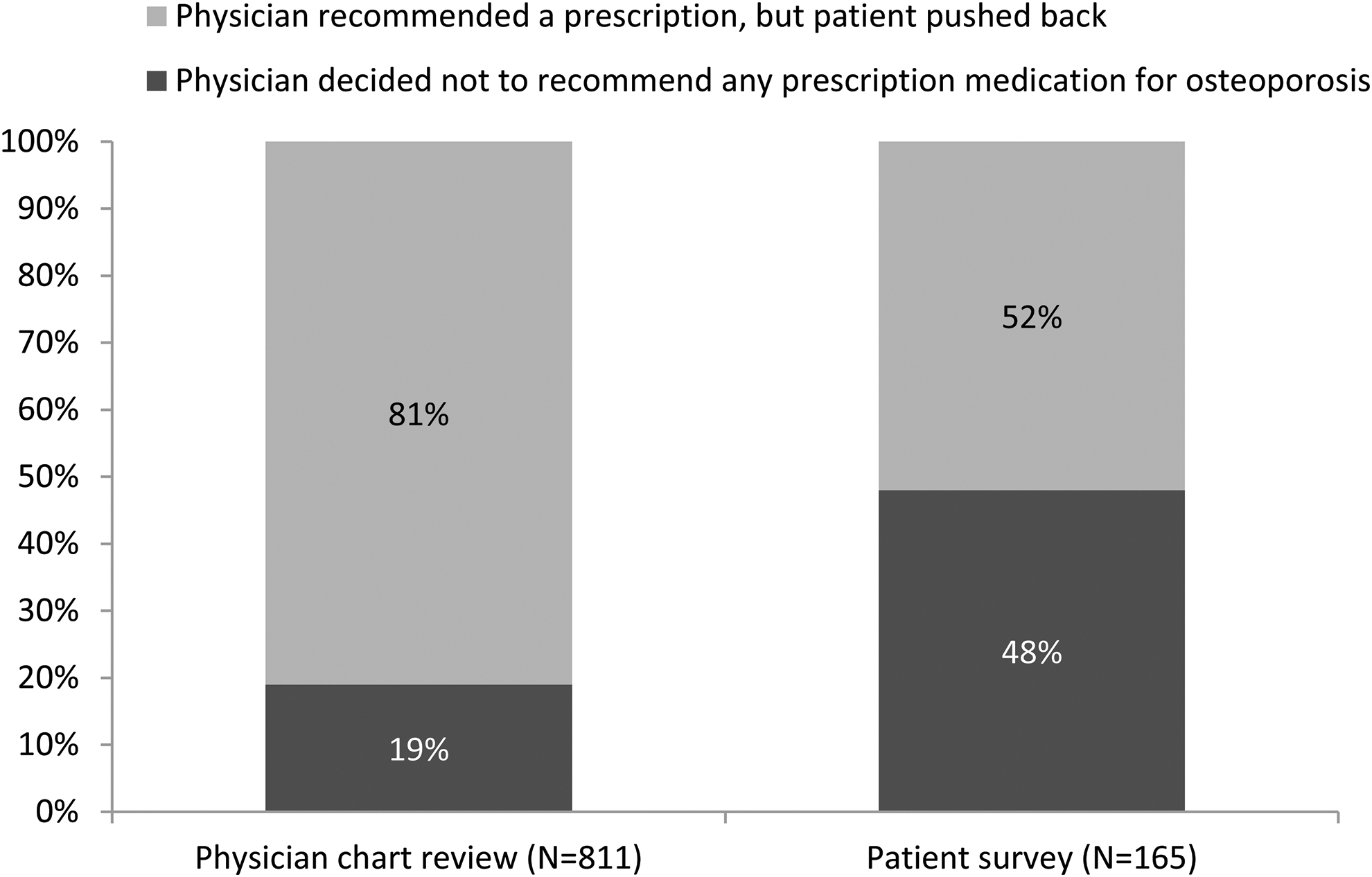
Decision not to recommend (physician) or accept (patient) treatment with prescription medication. Source: physician and patient survey questions D21 and C4, respectively.
The reasons why physicians did not recommend an osteoporosis medication prescription, as recorded in patient charts in the physician chart review and in the patient survey, are shown in Figure 2. The four most frequent reasons in both surveys were, in descending order, low calcium/vitamin D (32% in the physician chart review and 23% in the patient survey), risk of bisphosphonate side effects (20% in the physician chart review and 21% in the patient survey), GI problems (27% in the physician chart review and 20% in the patient survey), and polypharmacy (15% in the physician chart review and 19% in the patient survey). The frequencies of most reasons were similar in both the physician chart review and patient survey.
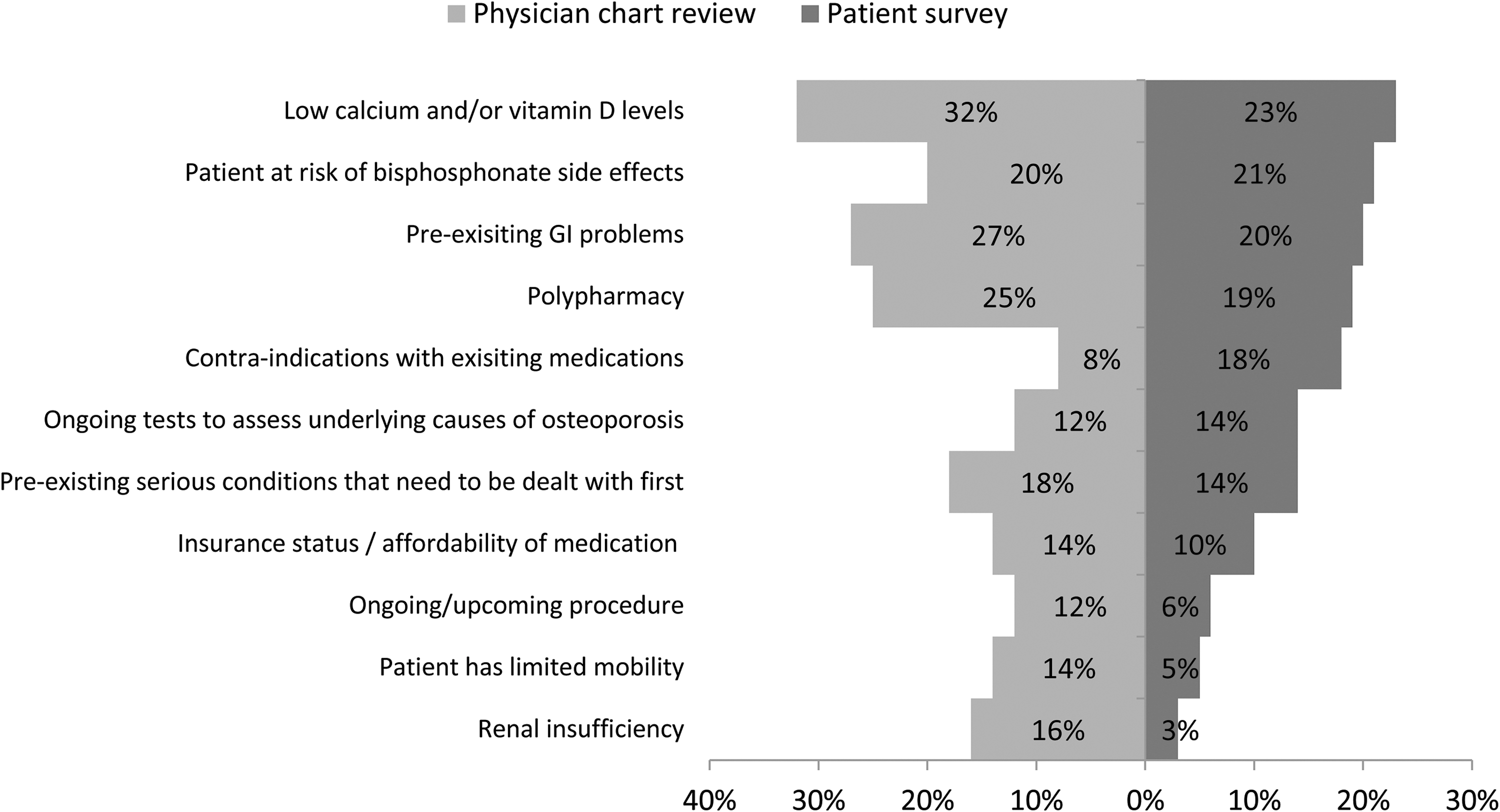
Reasons why physicians did not recommend medication as recorded in the physician survey (in patient charts) and in the patient survey. GI, gastrointestinal. Source: physician and patient survey questions D22 and C5, respectively. Responses are shown in descending order of item response frequency (as a percentage of patients) in the patient survey. Responses selected in the physician survey that are not shown are: dementia (15%), functional status (14%; dementia and functional status had no equivalent in the patient questionnaire), noncompliance (9%), and other (12%). Sample sizes: patient charts (where physicians did not recommend prescription medication), N = 153; patients who mentioned physician decided not to prescribe treatment, N = 90.
Patient reasons for declining a physician's recommendation for an osteoporosis medication prescription, as recorded in patient charts in the physician chart review, and in the patient survey, are shown in Figure 3. The five most frequent reasons in both surveys were, in descending order, concern about side effects (63% in the physician chart review and 65% in the patient survey), considering other options (42% and 52%), questioning the potential benefit of medications (32% and 33%), polypharmacy (26% and 22%), and unwillingness to take medications for any condition (21% among both populations). The frequencies of these reasons were similar in both the physician chart review and patient survey.

Reason why patient did not accept prescription medication as recorded in the physician survey (in patient charts) and in the patient survey. N/A, not applicable (the physician survey did not provide a response corresponding to “Patient has not experienced negative health issues related to osteoporosis” in the patient survey). Source: physician and patient survey questions D23 and C7, respectively. Responses are shown in descending order of item response frequency (as a percentage of patients) in the patient survey. Sample sizes for patients who declined an osteoporosis medication prescription: physician survey (from patient charts), N = 658; patients survey, N = 75.
Physicians' management of postmenopausal osteoporosis
Two hundred twenty-four physicians completed the physician survey. In the previous 12 months, these physicians had seen an average of 554 postmenopausal female patients, of whom 126 (23%) were newly diagnosed with osteoporosis (Table 2). Physicians screened 72% of postmenopausal women for osteoporosis, including 86% of postmenopausal women with a recent fracture. Osteoporosis screening was conducted primarily through a BMD or a DXA scan (89% of patients screened) or through Fracture Risk Assessment Tool (FRAX) or “other” questionnaire (31% of patients screened).
Values are Ns or percentages.
Source: physician survey questions A5 and A7.
N = 212.
Source: physician survey questions B1 and B2.
Source: physician survey question B3.
Responses can sum to greater than 100%.
Physicians' recommendations for postmenopausal women with a new osteoporosis diagnosis are shown in Figure 4. Most newly diagnosed patients were given a recommendation for behavioral modification (80%), calcium/vitamin D supplements (85%), and/or a prescription medication (72%). Fewer primary care physicians had made any of these recommendations than did physicians in other specialties, and in some instances these differences were statistically significant (Fig. 4). Twenty-eight percent of postmenopausal women that physicians newly diagnosed with osteoporosis did not receive a prescription for an osteoporosis medication. This percentage did not differ significantly between physician specialties.
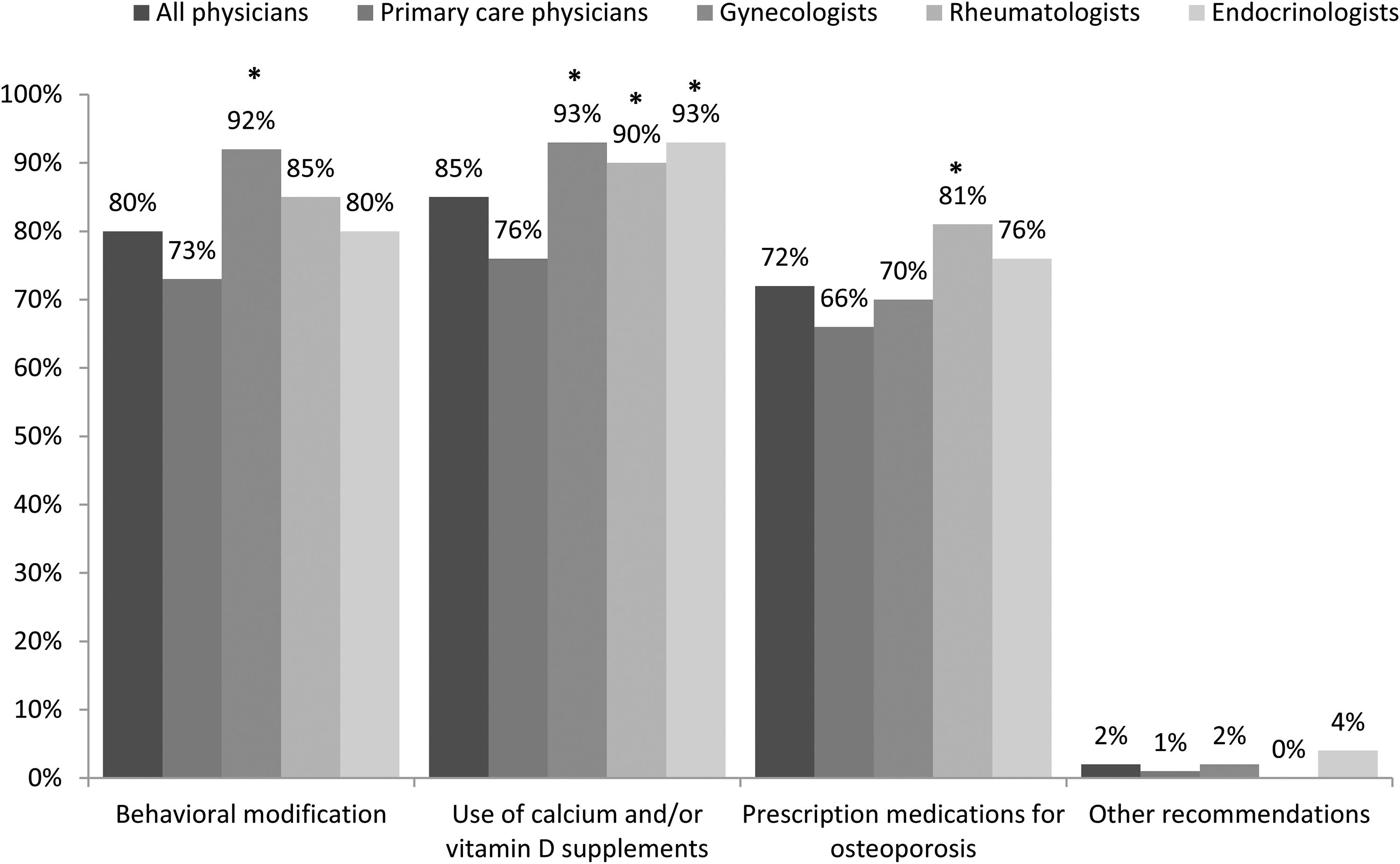
Percentage of postmenopausal women newly diagnosed with osteoporosis with physician recommendation for treatment (physician survey). Source: physician survey question C1. *Indicates a statistically significant difference versus primary care physicians (p < 0.05).
Discussion
A substantial proportion of osteoporotic women in the U.S. are not pharmacologically treated for this condition. However, the reasons for nontreatment of osteoporosis are not well understood. SOUND was a descriptive, exploratory study, which aimed to address the reasons why postmenopausal women do not receive a prescription medication to treat newly diagnosed osteoporosis.
The study provides information on nontreatment of osteoporosis from the physician's perspective based on a review of patient charts, patients' reasons for nontreatment, and physicians' management of osteoporosis. The principal reasons for not being treated with a prescription medication, given by both physicians and patients, were that there were alternatives and concern about the risks of prescription medications.
In the physician survey, physicians estimated that 28% of their postmenopausal osteoporosis patients did not receive a prescription osteoporosis medication after diagnosis, compared with 35%–64% in published U.S. studies (results from the first section of the physician survey). 6 –9 In most published reports of patients not prescribed an osteoporosis medication, it is unclear whether the decision against treatment was the patient's or the physician's. 6 –9 In a recent survey of women with a new diagnosis of postmenopausal osteoporosis, the decision against treatment was the patient's in 35% of cases. 10 The results of the current study show that it was the patient's decision in at least half of the cases of nontreatment. There was, however, a disparity in reports by physicians and patients in their perceptions regarding who decided against an osteoporosis prescription medication. While physicians reported in the physician chart review that the patient decided against an osteoporosis prescription medication in 81% of untreated patients, only 52% of respondents to the patient survey reported that this was their decision.
It is unknown whether this disparity reflects a sample selection bias—distinct groups of patients in the physicians' chart reviews and the responding patient survey members—or whether physicians' and patients' perceptions of their encounter simply differed. It is possible that the physicians might have perceived that they were effectively communicating the value of taking medications and that patients pushed back on the recommended medications, while patients in fact may not have adequately grasped the medication benefits and risks. This could be further substantiated by the results of the patient survey, where 37% of untreated patients mentioned that if more information were available from their healthcare provider, they would be highly likely to take the recommended osteoporosis medications (data not shown).
Valid response rates to the SOUND surveys cannot be calculated, because the number of panel members who were eligible to participate is unknown. The physician survey was sent to physicians in the specialties eligible for the study, but it is unknown how many met all the study eligibility criteria. Nevertheless, the characteristics of physicians in the SOUND survey are consistent with those of physician populations in other surveys. 11 –13 In the SOUND study, 70% of responding physicians were male and physicians had been in practice for an average of 16 years. In other recent surveys, males typically represented the majority of responding physicians (48%–88%) and physicians had an average of 13–26 years of experience. 11 –13
In the case of the patient survey, 11,533 invitations were mailed to female panel members over the age of 55. If we assume, based on population estimates that ∼15% of these women had osteoporosis, 1 –3 and that 50% of those women were not treated with an osteoporosis medication, 6 –9 then the approximate number of panel members eligible to participate in the patient survey was 865, and the 165 members who completed the questionnaire during the survey time window represent an estimated valid response rate of 19%.
The two sets of patients, those in the medical charts reported by physicians and patient panel respondents, differed in several characteristics. Patients included in the physician chart review were younger, less predominantly Caucasian, and had lower rates of various risk factors (e.g., limited dairy/calcium intake, height loss, and a previous fracture) than patients included in the patient survey.
These patient groups are similar to patients enrolled in previously reported studies. 7,14,15 The majority of patients enrolled in these studies were aged 55 and older and Caucasian. The National Osteoporosis Risk Assessment (NORA) study is a longitudinal observational study of postmenopausal women aged ≥50 with a new osteoporosis diagnosis and included 200,160 women. 14 The mean age of NORA patients was 64.5 years and the majority of patients in the NORA study were Caucasian (89.7%), similar to patient survey respondents. 14 At baseline, 11.0% of women in NORA reported experiencing a fracture after the age of 45 years. 14 This is similar to the patients included in the physician chart review in which 7% reported experiencing a previous fracture, but is different than the patients included in the patient survey in which 47% reported experiencing a previous fracture. Prior fracture rates reported in the patient survey included any previous fractures. Among the 47% of patients that reported experiencing a previous fracture, 37% of these fractures were fractures of extremities (foot, toes, or fingers), 31% were hip fractures, 17% wrist fractures, 13% vertebral fractures, 4% femoral, and less than 10% were other fractures.
There is striking agreement between the physician and patient surveys in the reasons given for nontreatment with a prescription medication. The four most frequent reasons why physicians did not recommend an osteoporosis medication prescription, as recorded both in the physician chart review and in the patient survey, were low calcium/vitamin D, risk of bisphosphonate side effects, GI problems, and polypharmacy.
The five most frequent reasons why patients declined a physician's recommendation for an osteoporosis medication prescription, as recorded in the physician chart review and the patient survey were, in descending order, concern about side effects, considering other options, questioning the potential benefit, polypharmacy, and unwillingness to take medications for any condition. The most frequent reasons behind physicians' decision not to prescribe an osteoporosis medication in the SOUND study differ somewhat from those in an analysis of medical records of U.S. patients with osteoporosis not currently receiving an oral bisphosphonate, reported by Kamneva et al. 16 In that study, the most frequent reasons cited by providers for not prescribing a bisphosphonate were, a GI diagnosis (56%), low functional status (51%), poor renal function (25%), advanced dementia (26%), history of bisphosphonate side effects (15%), and patient preference (8%). 16 The patient population in the Kamneva study differed from that in SOUND, in that patients in the former study were not limited to those with a new, initial diagnosis of osteoporosis, and most were Caucasian women older than 65 years of age.
The reasons for patients' decision not to accept a physician's recommendation for an osteoporosis medication prescription were similar in SOUND to those in a survey of postmenopausal women with a new osteoporosis diagnosis reported by Yu et al. 10 In Yu et al. the primary reasons that patients gave for not accepting a physician's recommendation to initiate osteoporosis medications were concern over side effects (77%), medication costs (34%), and pre-existing GI concerns (25.0%). The relatively greater importance of medication costs in that study (in SOUND 10% of patient respondents could not afford the medication) may reflect a difference in socioeconomic status.
Other studies have queried patients' attitudes toward osteoporosis and osteoporosis prescription medications. Yood et al. reported a survey of women with a DXA test and an osteoporosis diagnosis, who either did or did not fill a prescription for an osteoporotic drug in the first 3 months after the DXA exam. 7 Women who initiated pharmacotherapy believed more strongly in the benefits and effectiveness of medications than those who did not, whereas the latter reported more distrust of medications. 7 This is similar to results of the SOUND patient survey, where questioning the potential benefit of taking medication and unwillingness to take any medications ranked third and fifth among reasons not to accept a physician's recommendation for an osteoporosis medication. In addition, the 2008 survey found that both osteoporosis knowledge and the belief that osteoporosis is a serious disease increased the likelihood of initiating osteoporosis treatment. 7 Consistent with this, one fifth of untreated patients in the SOUND patient survey declined an osteoporosis prescription medication because they had not experienced negative health issues related to the condition. This suggests that some patients may not fully comprehend the impact of osteoporosis on their health.
This study has several limitations. The results of our internet survey may not be generalizable to the entire U.S. physician or patient population because an internet survey may systematically exclude older respondents, respondents who are not comfortable using a computer, and/or respondents who do not have access to the internet. In addition, physicians and patients were recruited from national panels of individuals who wish to participate in online surveys. These participants may not be representative of the general population. However, we compared our physician and patient populations to those enrolled in similar previously reported studies and there were many similarities between the populations enrolled. The cross-sectional design of the study is limited by the accuracy of patient and physician recall and reporting bias. Physicians may have selected the most recent/convenient charts for review thus introducing selection bias in the study. However, if this occurred, it may have allowed the physicians to more easily recall the reasons for nontreatment for that patient, thus reducing the chance of recall bias. In addition, we did not query patients on their perceptions of the physician–patient relationship, which has been previously shown to affect a patient's willingness to start osteoporosis therapy. 17
Conclusions
The SOUND surveys found that patients, rather than the physicians, decided against pharmacological treatment of newly diagnosed osteoporosis in at least half of cases of nontreatment. Both patients and physicians considered other options and expressed concerns about medication side effects, whereas patients were also skeptical about the benefits of osteoporosis medications.
Footnotes
Acknowledgments
The authors thank Juliana Lewis for her scientific contributions to this project. This article was prepared with the assistance of ScribCo Associate Medical Writer, Anna Kaufman, MPH.
Author Disclosure Statement
J.P.W., A.M., and S.S. are employees of Merck & Co., Inc. A.M. and S.S. own stock in the company. K.O. and R.S. are employees of Evidera and have received financial remuneration from Merck & Co., Inc. to perform statistical analyses.