
Abstract
Objectives:
Sexual health in survivors of gynecologic cancer has been studied; however, sexual health in these women before treatment has not been thoroughly evaluated. The objective of our study was to describe the pretreatment characteristics of sexual health of women with suspected gynecologic cancer before cancer treatment.
Materials and Methods:
We performed a cross-sectional analysis of women with a suspected gynecologic cancer, who were prospectively enrolled in a hospital-based cancer survivorship cohort from August 2012 to June 2013. Subjects completed the validated Patient-Reported Outcomes Measurement Information System Sexual Function and Satisfaction Questionnaire. Pretreatment sexual health was assessed in terms of sexual interest, desire, lubrication, discomfort, orgasm, enjoyment, and satisfaction.
Results:
Of 186 eligible women with suspected gynecologic cancer, 154 (82%) completed the questionnaire pretreatment. Mean age was 58.1 ± 13.3 years. Sexual health was poor: 68.3% reported no sexual activity, and 54.7% had no interest in sexual activity. When comparing our study population to the general U.S. population, the mean pretreatment scores for the subdomains of lubrication and vaginal discomfort were similar, while sexual interest was significantly lower and global satisfaction was higher. In a linear regression model, controlling for cancer site, age remained significantly associated with sexual function while cancer site did not.
Conclusions:
Problems with sexual health are prevalent in women with suspected gynecologic malignancies before cancer treatment. Increasing awareness of the importance of sexual health in this population will improve quality of life for these women.
Introduction
S
As women with gynecologic cancer have pathology that directly affects sexual organs, it is not surprising that a large proportion of women with gynecologic cancer report some form of sexual problem. 1 As such problems persist well into the survivorship phase, sexual health issues greatly influence women's ability to adjust and cope with the sequelae of gynecologic cancer. 4
While sexual dysfunction in gynecologic cancer survivors has been previously investigated, sexual health in women with suspected gynecologic cancer before cancer treatment has been studied on a very limited basis. 5 Gynecologic oncology providers are frequently confronted by a number of hurdles when addressing sexual health issues with their patients, such as lack of provider time, willingness, or training to appropriately address issues surrounding sexuality. 6,7 It is critical to identify the pretreatment rate of sexual health problems in this at-risk population to better understand how cancer treatments—surgery, chemotherapy, and/or radiation—affect sexuality into the survivorship phase.
Understanding the characteristics of pretreatment sexual health will help providers better address the impact of treatment on sexuality and sexual function in gynecologic cancer patients as this aspect of quality of life has been understudied. In addition, recognizing these potential changes to sexual interest and desire from before to during and after treatment can help physicians to better prepare women for postoperative survivorship. This will, in turn, allow for more comprehensive care and informed counseling to women undergoing these treatments. Thus, the primary objective of this study was to describe the prevalence of sexual health issues in women with suspected gynecologic malignancy before cancer treatment. Secondary objectives included assessing the effect of age and gynecologic cancer site on the prevalence of sexual health problems.
Materials and Methods
We conducted an institutional review board (IRB)-approved cross-sectional ancillary analysis of data collected for a large hospital-based observational cancer cohort. The Health Registry/Cancer Survivorship Cohort (HR/CSC) is an IRB approved University of North Carolina at Chapel Hill (UNC) Healthcare registry of cancer patients that integrates a comprehensive database of clinical, epidemiological, and interview data with repositories of biologic specimens and tumor tissue. Patients are identified and recruited through UNC Healthcare oncology outpatient clinics with the following eligibility criteria: age 18 years or older; North Carolina mailing address; and English or Spanish language proficiency. Patients who are unable to provide informed consent or participate in interview questionnaires are excluded. For this analysis, eligibility was further restricted to HR/CSC patients recruited through the gynecologic oncology clinics and who completed the baseline interview before any cancer treatments. The study cohort included all subjects enrolled in the UNC HR/CSC from August 2012 to June 2013 presenting for first treatment of suspected gynecologic malignancies.
For the primary study, eligibility was further restricted to HR/CSC patients who were recruited through the gynecologic oncology clinics with newly diagnosed or suspected gynecologic cancer and planned surgical management. Exclusion criteria included primary surgery completed or to be completed at an outside institution, active chemotherapy or radiation treatment, and pregnancy. Further restrictions for this study include completion of the pretreatment interview questionnaires before any cancer treatment.
Interviews were conducted within 2 weeks of enrollment by trained staff using a computer-assisted telephone interview software tool specifically developed for the HR/CSC. Interview questionnaire topics include medical and social histories and general and cancer-specific health assessments.
The structured Patient-Reported Outcomes Measurement Information System Sexual Function and Satisfaction Questionnaire (PROMIS-SFQ) was given to all participants at the baseline, preoperative interview, 8 and responses from this questionnaire were analyzed for this study. The PROMIS-SFQ is a questionnaire validated to assess symptoms related to sexual function. The questionnaire has 10 items, which evaluate female sexual function and its impact on quality of life. Within the questionnaire there are four subdomains as follows: (1) global satisfaction with sex life, (2) interest in sexual activity, (3) lubrication, and (4) vaginal discomfort. Symptom severity is graded on a 10-point Likert-type scale over the past 30 days.
PROMIS is scored using T scores, which are standardized to the U.S. general population and have a mean of 50 and a standard deviation of 10. Scores above or below 50 are above or below the population average in the United States, respectively. A clinically meaningful difference for this scale is defined as one-half standard deviation (five points) above or below population norms.
Relevant clinical data at the time of the new patient visit, such as body mass index (BMI), comorbid conditions, mental health history, insurance status, and cancer site, were abstracted from the electronic medical record. The clinical data abstracted from the medical record were merged with the HR/CSC demographic and questionnaire data using an honest broker system. The HR/CSC subsequently provided a deidentified data set for our analysis.
The primary aim of this study was to characterize the pretreatment sexual function in a population of women with suspected gynecologic malignancy. Thus, an a priori power calculation was not performed. Univariate and bivariate summary statistics were used to analyze categorical variables, while Student's t-test and analysis of variance were used to analyze continuous variables such as age and BMI in bivariate and multivariable comparisons, respectively. Age was dichotomized into a categorical variable using ≥ or ≤50 years to estimate menopausal status, as this information was not directly available, and Fisher's Exact test was used to analyze symptoms between women aged ≥ or ≤50 years.
Because each cancer site had relatively small numbers, sexual function scores across cancer sites were analyzed with nonparametric testing, specifically, the Kruskal–Wallis test. Multivariable logistic regression was also performed. A p-value <0.05 was considered statistically significant. Data were analyzed with IBM SPSS version 18.0 (IBM SPSS, Inc., Chicago, IL).
Results
Among 186 eligible women with a suspected gynecologic cancer during the study period, 152 (82%) completed pretreatment assessments and all went on to have surgery. The study cohort was largely Caucasian with private insurance (Table 1). The majority of women were diagnosed with early stage disease and approximately half underwent minimally invasive surgery. The most common site of gynecologic malignancy was uterine cancer, followed by ovarian, cervical, vulvar/vaginal, and other, which included gastrointestinal and unspecified gynecologic cancer. As final diagnoses were dependent on the surgical pathology, three subjects were found to have primary gastrointestinal cancer rather than gynecologic disease based on surgical pathology.
Analysis performed with Student's t-test.
BMI, body mass index; GI, gastrointestinal; NOS, not otherwise specified.
Patients' responses to the PROMIS-SFQ revealed poor sexual health before treatment (Table 2). Nearly two-thirds of women reported not being sexually active before treatment, with approximately half reporting no sexual interest. Among sexually active women, approximately one-third reported experiencing some type of sexual problem in the form of difficulty with lubrication, difficulty with sexual activity due to discomfort or pain, or inability to have a satisfying orgasm or to have enjoyment or satisfaction with sexual activity. Over half reported “uncomfortable” or “very uncomfortable” vaginal sensation during sexual activity.
Over the past 30 days.
When comparing our study population to the general U.S. population based on PROMIS T-scores which reflect this larger group, the mean pretreatment PROMIS-SFQ scores for the subdomains of lubrication and vaginal discomfort were similar to the U.S. population, while sexual interest was significantly lower. 9 Despite overall poor sexual health, global satisfaction was higher than the general U.S. population mean (Fig. 1).
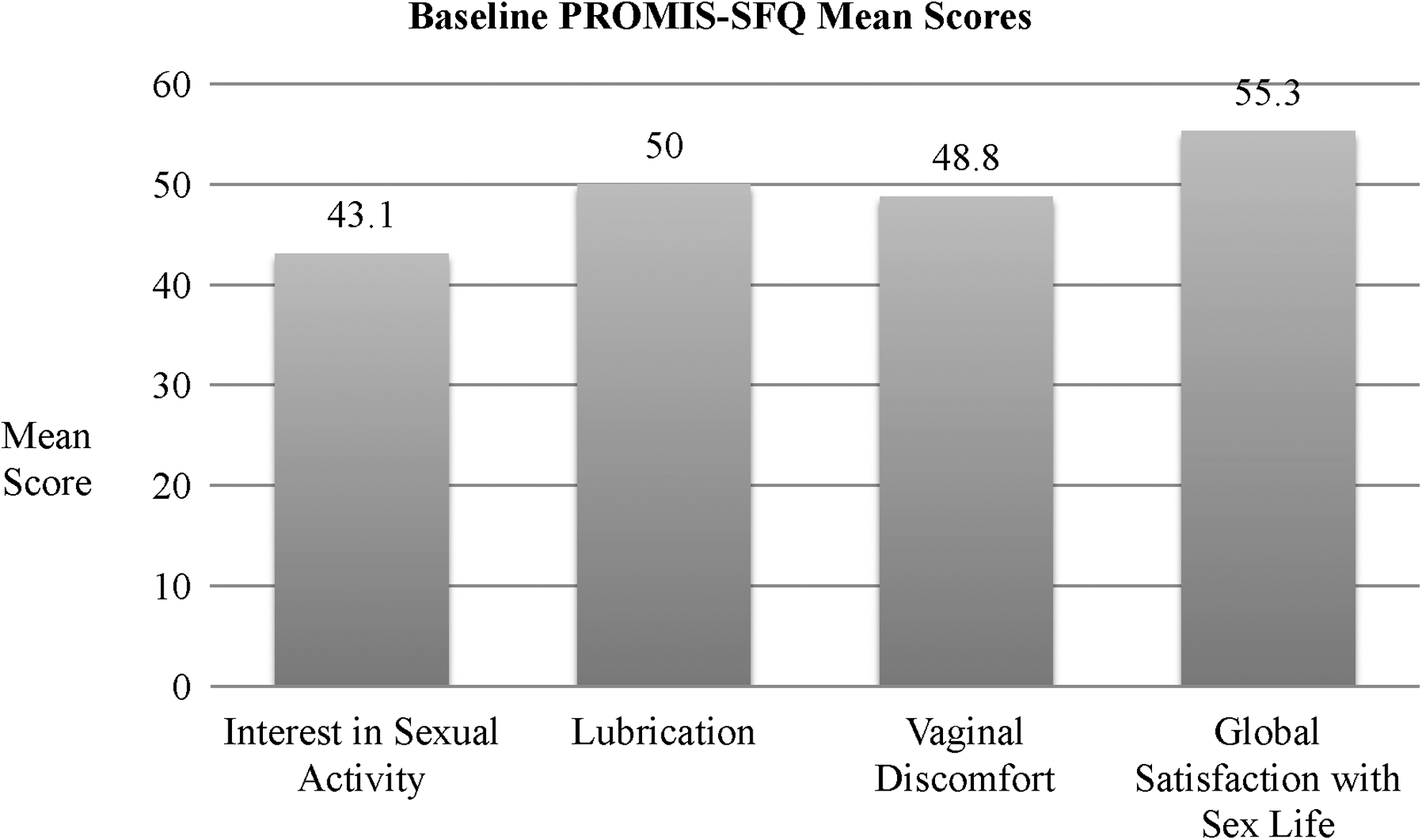
Baseline Patient-Reported Outcomes Measurement Information System Sexual Function and Satisfaction Questionnaire mean scores.
When assessing the effect of cancer site on sexual function before treatment, differences were appreciated in all domains, with the exception of difficulty with lubrication (Table 3). For uterine, ovarian, and vulvar cancer, women demonstrated low sexual interest and desire, with greater than half of women in each cancer site reporting no interest in sexual activity and no sexual desire. In contrast, a smaller percentage (29%) of women with cervical cancer reported low sexual interest or desire. In addition, the percentage of women with uterine, ovarian, and vulvar cancer who reported no sex in the last 30 days was approximately twice as high as women with cervical cancer (69% of uterine, 78% of ovarian, and 78% of vulvar vs. 35% of cervical patients).
All analyses performed by Kruskal–Wallis test.
When assessing the effect of age on sexual health, a significant difference was noted in all domains of sexual health when comparing women aged <50 and women aged ≥50 (Table 4). When assessing age based on cancer site, mean age for women with cervical cancer was significantly lower than the other cancer sites: uterine (60.6 years) versus ovarian (60.6 years) versus vulvovaginal (53.9) versus cervical (42.8 years) (p ≤ 0.001). In a linear regression model controlling for cancer site, age remained significantly associated with sexual activity but cancer site did not, with lower age indicating increased likelihood of sexual function (95% confidence interval 0.91, 0.98).
Analysis performed with Fisher's exact test.
Discussion
Gynecologic cancer is known to have an effect on sexual health. This study provides new data regarding sexual health in women with suspected gynecologic cancer before treatment. A large proportion of women reported sexual difficulties in the pretreatment phase, with nearly two-thirds reporting not being sexually active and approximately half reporting no sexual interest in the past 30 days. Furthermore, sexual health in the pretreatment phase differed significantly when comparing different cancer sites, as well as age, with age being a more powerful influence than cancer site in this cohort. The high prevalence of sexual difficulties before cancer treatment highlights the fact that sexual health is a significant quality of life issue not only during the survivorship phase but also before initiating treatment for gynecologic cancer.
Our study's findings suggest that before any treatment, interest in sexual activity of women with suspected gynecologic cancer is impaired compared to the general U.S. population. Our cohort overall also reported low rates of engaging in sexual activity. In 2006, Addis et al. published a study evaluating sexual health in middle-aged women and found that three-fourths reported being sexually active—a rate thrice higher than our study cohort. 10 In a study on female sexual health conducted by Lindau et al., of women in the 57–68 year age group, 62% were sexually active within the past year—nearly double the rate in our study cohort. 11
It is important to point out that these differences may be due to the fact that the questionnaires used in Addis' et al. 10 and Lindau et al.'s 11 studies relied on a longer recall period (1 year) than the PROMIS-SFQ (30 days). In addition, the pretreatment time period is unique in the patient experience, as the emotional stress of a possible cancer diagnosis and the anticipation of its associated treatment can be profound. 8 These emotional stressors can lead to anxiety and depression, which have been identified as causes of sexual dysfunction particularly in the realms of interest and desire. 12
In addition to lower interest in sexual activity, our cohort reported higher rates of sexual difficulties than the general population. In Lindau's 11 study, fewer women reported lack of sexual interest, difficulty with lubrication, or pain with intercourse compared to our cohort. The physical changes brought upon by gynecologic cancer and the psychological burden associated with a cancer diagnosis may be the underlying root of the sexual dysfunction experienced by women with suspected gynecologic cancer. 7
Interestingly, compared to previously reported rates of sexual function in the gynecologic cancer population at the time of first patient visit, our study reported higher levels of problems with sexual health. Kennedy et al.'s 5 study of sexual function in women presenting for initial gynecologic oncology consultation reported a similar rate of sexual activity in the past 4 weeks (39% of women in their study compared to 32%–34% in our study); however, they reported a lower rate of “problems with sexual functioning” at 9% in the sexually active portion of their cohort. This may highlight the fact that if women were sexually active, they were less likely to be experiencing problems with sexual function.
Along the same vein, women in our cohort reported higher sexual satisfaction than the U.S. population average. This may be due to the fact that while sexual function was lower overall, those that were sexually active had greater satisfaction. When comparing our outcomes to those of Kennedy et al., 5 a number of important aspects differ between our study and Kennedy et al.'s study. The questionnaire Kennedy et al. 5 used to assess sexual dysfunction relied on a “yes” or “no” response to the question, “do you have problems with sexual functioning?” As our study relied on answers from the PROMIS-SFQ, we were able to delineate the nature and degree of dysfunction in specific domains of sexual function and resultantly were able to capture more women with sexual difficulties.
In addition, Kennedy et al. 5 did not compare different cancer sites, while our study was able to highlight some differences among the gynecologic cancer population. In terms of cancer specific outcomes in our study, women with uterine, ovarian, and vulvar/vaginal cancer were found to have higher rates of sexual difficulties in the pretreatment phase compared to women with cervical cancer. This is likely, in part, related to the fact that women with cervical cancer are typically younger. Many women with gynecologic cancer present with symptoms such as bloating from ascites or vaginal bleeding from their tumor, which could exacerbate preexisting sexual dysfunction; however, it is unclear if cancer-specific symptoms are the reason for the difference in sexual functioning across these groups, especially considering the small size of the relative cancer site populations.
Age was also found to be significantly associated with sexual dysfunction. The hypoestrogenic state conferred by menopause could be contributing to higher levels of sexual dysfunction. Other factors such as partner status, for example, were not assessed, which is a limitation of our study, as older partners may have partner issues, and sexual health may represent an unmeasured barrier, independent of diagnosis.
The strength of our study is that it provides new information on sexual health in women with gynecologic cancer before treatment. Furthermore, this study was built upon a well-characterized cohort with self-reported data collected pretreatment using standardized validated questionnaires by trained interviewers conducting computer-assisted telephone interviews that include real-time quality control features (e.g., logic and range checks).
Our study may be limited in generalizability as it reflects single-institution cohort with a lower proportion of racial and ethnic minorities than the greater U.S. population. Our analysis of sexual dysfunction in regards to satisfaction, lubrication, and vaginal discomfort may have been limited as a large proportion of women were not sexually active.
In addition, small sample sizes for some cancer sites reduced our ability to detect differences between these groups. This is important because symptomatology of each cancer site differs, and thus, we cannot fully assess cancer site as a causal agent for sexual dysfunction. Furthermore, the response rate was high at 82%, but 18% of women either declined to participate or did not complete baseline surveys, and this portion of the population may represent a clinically different and thus important segment, which this study does not capture. Also, physical examination information that could be relevant to sexual function, for example, shortened vagina and pelvic organ prolapse, was not collected, making it difficult to determine whether such findings were contributing to self-reported sexual difficulties.
It is important to note that by nature of enrollment at the time of the new patient visit, we cannot account for how a potential cancer diagnosis affected these pretreatment scores. This is unavoidable given the study setting; however, we believe it accurately captures the sexual health of this population in the pretreatment phase. Other factors may also affect sexual function in this group, including anxiety related to a cancer diagnosis.
Conclusions
As sexual dysfunction greatly impacts quality of life for women with gynecologic cancer, sexual health should become a priority for gynecologic oncology providers. Our results suggest that symptoms of sexual dysfunction are prevalent in women with suspected gynecologic malignancies before cancer treatment, especially in women aged ≥50 years. Gynecologic oncology providers should consider incorporating screening for sexual dysfunction as part of a comprehensive pretreatment evaluation before initiation of cancer treatment.
During and following cancer treatment, sexual health should be regularly addressed by providers at follow-up evaluations to identify issues with sexual health and provide treatment options for those who are dissatisfied by any sexual dysfunction. It is a topic that can be embarrassing for women to bring up with their provider, and they may not think it is a relevant topic at their cancer treatment visits. Thus, it is important for providers to take the first step to introduce the topic of sexual health and let women know that it is an important part of their treatment plan and their overall health.
More research is needed in identifying which women are at greatest risk for developing sexual dysfunction and what interventions are most effective for this cohort. As prior research largely emphasized the physical aspects of sexual dysfunction, 13 more studies are needed to explore the psychological and social dimensions of sexuality. Finally, prospective studies are needed to explore the impact of gynecologic cancer treatments on sexual function over time as this subject still needs more extensive examination. The ultimate goal is to increase awareness of the importance of sexual health in this special cohort of women in order to improve perioperative care and counseling, as well as boost overall quality of life in the survivorship phase.
Footnotes
Author Disclosure Statement
No competing financial interests exist.