
Abstract
Abstract
Background:
Neurologically impaired children (NIC) have a high risk of recurrence of gastroesophageal reflux (GER) following fundoplication. A postpyloric feeding tube may be useful when gastric emptying disorders occur; however, dislocation and difficulty in feeding management often require more aggressive procedures. Total esophagogastric dissociation (Bianchi's TEGD) is an alternative to the classic fundoplication procedure, whereas laparoscopic gastric bypass is a frequently performed procedure in morbid obesity, improving gastric outlet.
Aim:
The aim of this paper is to present a preliminary experience on the laparoscopic Roux-en-Y gastrojejunal bypass, associated with Nissen fundoplication and gastrostomy, to treat and prevent GER in NIC with gastric emptying disorders.
Materials and Methods:
Eight neurologically impaired children underwent surgical treatment because of feeding problems and pulmonary complications. The procedure included: 1) hiatoplasty, 2) Nissen fundoplication, 3) 20-cm Roux-en-Y gastrojejunal anastomosis and jejuno-jejunal anastomosis, and 4) gastrostomy.
Results:
All cases were fed on postoperative day 3 without any intraoperative complications. One case developed an obstruction of the distal anastomosis due to adhesion and needed reoperation. Outcome was clinically evaluated with serial upper gastrointestinal contrast studies and endoscopies.
Conclusions:
Laparoscopic proximal Roux-en-Y gastrojejunal diversion, without gastric resection, is a safe, feasible procedure that improves gastric emptying and reduces the risk of GER recurrence. Yet, long-term results still have to be evaluated.
Introduction
Delayed gastric emptying is a commonly associated complaint, especially for those patients operated on with fundoplication, who may develop or show a persistence of postoperative retching that can increase the risk of wrap herniation, with or without disruption. 10 In such distressed patients, a postpyloric feeding should be considered: Pyloric surgery, post-pyloric tube positioning, or jejunostomy are possible options.13,15–19 Many endoscopic procedures are required to manipulate postpyloric feeding tubes. 15 Moreover, postpyloric feeding can cause dumping syndrome, whereas stricture is a frequent complication of pyloric surgery, thus leading to even worse feeding difficulties. 20
Pyloric injection of botulinum toxin significantly improves gastric emptying, yet its effect is short-lasting, often requiring repeated injections. 21 Total esophagogastric dissociation (TEGD) is a further alternative technique in order to reduce GER recurrence and supraesophageal complications and, therefore, the related need of iterative surgery.9,22–24 Basing on what was previously published by the same researchers,25–28 this study will present the unicentric provisional experience on laparoscopic proximal Roux-en-Y gastrojejunal diversion, associated with gastrostomy and fundoplication, aimed at improving gastric emptying disorders, preventing GER, and allowing adequate gastric feeding (Fig. 1).
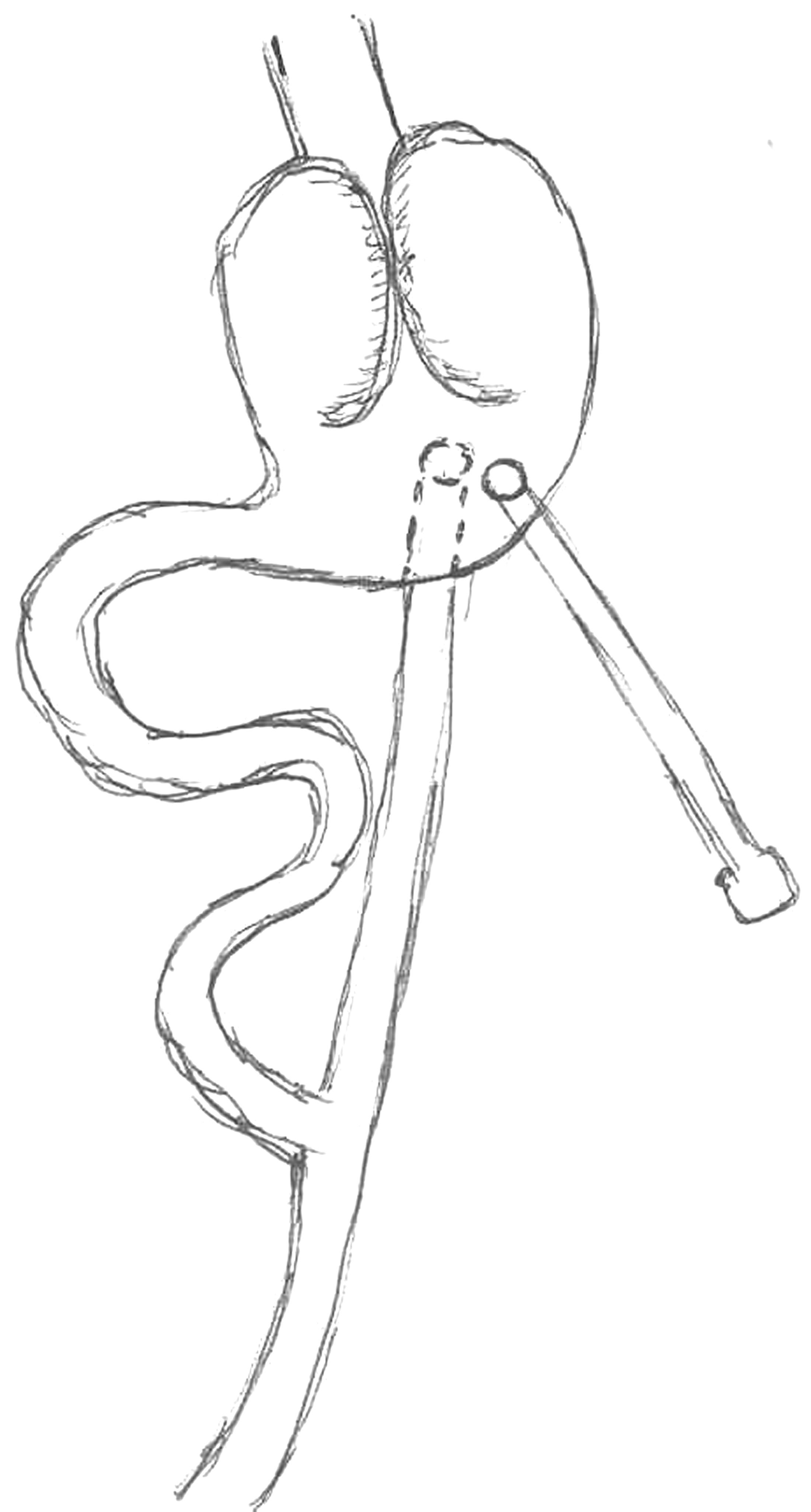
The proximal Roux-en-Y gastrojejunal diversion, associated with Nissen fundoplication and feeding gastrostomy.
Materials and Methods
All NIC scheduled for the surgical treatment of GER and delayed gastric emptying at our institution from August 2007 to August 2008 were included in this prospective, clinical trial. The preoperative diagnostic work-up included a contrast study of the upper GI tract focalized on the swallowing phase (videofluoroscopic swallowing study). GER was assessed according to previously reported methods from our institution, using 24-hour multichannel intraluminal impedance (MII) combined with pH monitoring. 29 Delayed gastric emptying was determined by clinical evidence: intolerance to prepyloric feeding (persistent vomiting) opposed to well-tolerated postpyloric enteral feeding. Delayed gastric emptying was confirmed during the upper GI contrast study showing weak gastric contraction and slow transit of the contrast medium into the duodenum. Endoscopy (esophagogastroduodenoscopy; EGD) was performed only in case a percutaneous endoscopic gastrostomy (PEG) tube insertion was planned. Surgery was, therefore, proposed once the following inclusion criteria were fulfilled: 1) evidence of impaired oral feeding with recurrent aspiration, confirmed on GI contrast study, 2) clinical evidence of delayed gastric emptying requiring postpyloric feeding, and 3) presence of GER. 29 Parents of the patients were accurately educated and informed about all therapeutic strategies, with respect to risks and benefits. A patient-specific informed consent explaining the operation was offered, including details on: 1) performing a gastrostomy (according to the Stamm procedure) with low-profile tube insertion; 2) performing GER surgery (posterior hiatoplasty and 360-degree floppy Nissen wrap) 3) performing a proximal Roux-en-Y gastrojejunal anastomosis, without gastric disconnection, and 4) approaching the field laparoscopically, when feasible.
As an alternative to this single surgical program, a step-by-step approach was offered, involving multiple general anesthesia. The laparoscopic approach is performed by using 5 ports: the umbilical site (12 mm) is used for the scope and the stapler, the left flank (5 mm), and subcostal area (left 5 and right 3 mm) for operating instruments, and the epigastrium site (3 mm) to retract the liver and stomach. Complete release of the stomach from the colon and spleen is achieved with the exposure of the posterior gastric wall and pancreas. This large window allows a good view of the posterior gastric wall. The length of intra-abdominal esophagus is increased. A posterior Farrar hiatoplasty, using three nonreabsorbable 2/0 sutures, is done. A short 360-degree floppy Nissen fundoplication is fashioned. A nasogastric tube (NGT) is used during this maneuver. Multiple 2/0 nonreabsorbable sutures are used to fix the wrap to the diaphragm and esophagus (Fig. 2).

In all the cases a hiatal repair and a standard 360-degree Nissen wrap fundoplication were performed.
The Treitz ligament is identified and a jejunal loop is divided 20 cm distally, using a 30-mm linear Endo-GIA stapler (Autosuture−) (Fig. 3). A transmesocolic window is created in an avascular plane on the lefthand side of the colonic vascular pedicle not far from the Treitz ligament (Fig. 4). The distal jejunal loop is pulled up via the transmesocolic window and anastomosed to the posterior gastric wall. Two openings are respectively created onto the stomach and jejunum in order to insert the stapler branches and a posterolateral gastrojejunal anastomosis is performed, using a 30-mm linear Endo-GIA stapler (Autosuture−). Absence of bleeding and integrity of the anastomosis are meticulously checked and ruled out. After having ruled out gross bleeding, the anastomosis is completed with interrupted 4/0 nonabsorbable sutures (Fig. 5). A terminolateral Roux-en-Y anastomosis is performed between proximal (the “duodenal” loop) and distal jejunum (the “gastric” loop) about 20 cm distal to the Treitz ligament (Fig. 6). When indicated, a standard Stamm gastrostomy can be added by pulling the stomach out from the 5-mm left port and positioning a low-profile feeding tube.

A jejunal loop is prepared and interrupted 20 cm distally to the Treitz ligament in order to create the proximal Roux-en-Y diversion.

The proximal diversion is created in the posterior wall of the stomach. A 3-cm posterolateral anastomosis is created by using the linear stapler (Endo-GIA 30; USSC) and completed nonreabsorbable sutures

The proximal Roux-en-Y gastrojejunal diversion is finally completed by creating a terminolateral jejunaljejunal anastomosis 20 cm distally to the Treitz and the stomach.
The proximal gastrojejunal Roux-en-Y diversion is performed, passing through the mesocolon or in front of the colon.
Postoperatively, the patient is kept on intravenous fluids for 3 days until a GI-tract contrast study is performed to assess anastomotic patency and integrity. If no leakage is observed, the child is progressively started on either oral or gastrostomic feeding. The NGT output is strictly monitored in order to indirectly assess gastric emptying. Recurrence of symptoms such as vomiting and/or retching associated with increase of NGT output suggest persistent delayed gastric emptying and/or anastomotic stricture.
Once full feeding is obtained and no signs of complications are demonstrated, the patient is safely discharged home. Prolonged acid-suppressive therapy with proton-pump inhibitors (PPIs) is promptly administered after surgery to reduce the risk of marginal ulceration at the gastrojejunostomy. On postoperative day 30, an EGD is routinely performed (Fig. 7). Subsequent clinical follow-up is performed every 3 months. Provided no new symptom has been experienced, no further imaging is taken.

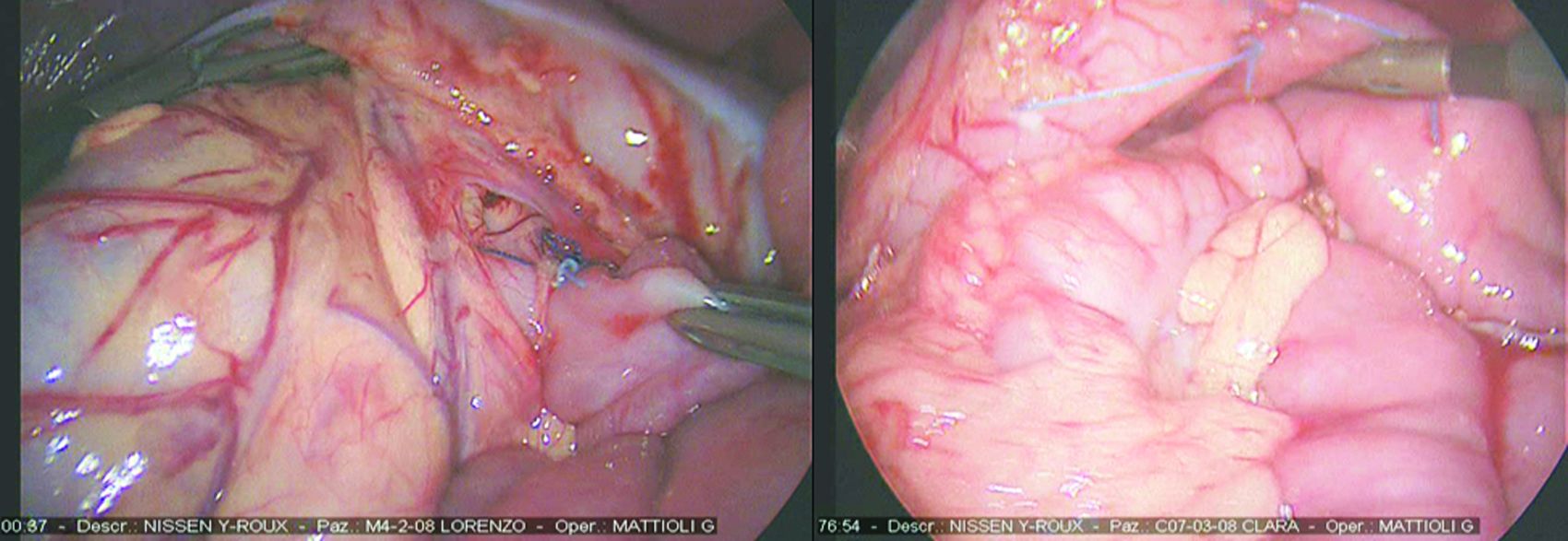
One case developed an early complication and needed a reintervention. The left picture shows a good transit through the anastomosis. The right picture shows a late complication with the colon herniated through the esophageal hiatus.
Results
Eight NIC were operated on during the study period (Table 1). CP represented an underlying disease in all patients, presenting with major feeding difficulties (severe dysphagia) and GER-related complications, such as failure to thrive and/or aspiration pneumonia. According to our previous experience, 29 24-hour MII/pH monitoring was performed in all patients and showed abnormal acid or nonacid liquid and mixed reflux either due to primary GER or related to impaired gastric emptying. Though without statistical significance, overall esophageal clearing time (bolus and acid) proved to be impaired (mean acid clearing time [MACT] and median bolus clearing time [MBCT] was longer, if compared to primary GER). Moreover, all patients presented with clinical evidence of symptom improvement once on postpyloric feeding.
CP, cerebral palsy; SB, spina bifida; MD, primary muscular disorders; WS, West syndrome; N, Nissen; G, gastrostomy; R, Roux.
The male to female ratio was 1.6 (5 males and 3 females). Median age at surgery was 3 years (range, 2–9) and median weight was 9 kg (range, 6–20). Four of 8 patients already had a gastrostomy in site. Three of them also had a Nissen fundoplication, thus requiring the gastrojejunal diversion only. In 3 cases, the jejunal loop was pulled up ventrally to the transverse colon (instead of creating a transmesocolic window). This choice was led by the abnormal gastric position due to the gastrostomy in site (Fig. 4).
Length of surgery was shorter than 4 hours in all patients: One case required a conversion to open surgery due to severe anesthesiologic issues. No intraoperative complications occurred. No leakages or strictures were demonstrated on the postoperative GI contrast study: All patients could be safely fed on postoperative day 3. One patient (MZI; Table 1) developed a small-bowel obstruction on postoperative day 10: An initial conservative approach turned out to be ineffective, thus leading to reintervention: Multiple bowel adhesions were found and released and the distal jejunal anastomosis was refashioned. The child recovered safely and was finally discharged home.
Another patient (SF; Table 1) developed signs of acute abdominal pain and bowel obstruction 6 months after the operation: A contrast study was performed, showing a colonic herniation through the diaphragmatic esophageal hiatus (Fig. 8). The patient underwent a laparotomy to reduce the hernia and to fix the hiatoplasty, with a subsequent symptoms resolution. EGD performed on day 30 could exclude gross marginal ulceration of the gastrojejunal anastomosis, which looked pretty healthy. No patients complained of retching, vomiting, gas bloating, or symptoms suggestive for dumping syndrome during the follow-up period lasting between 3 and 12 months.

One month postoperative endoscopic follow-up: details of patent gastrojejunal anastomosis and gastrostomy.
Discussion
Children with CP frequently complain of feeding problems, which, sometimes, can be managed by adapting posture, quality and quantity of feeding, and physical therapy. In case of failure to thrive, weight loss, or complications (e.g., aspiration pneumonia, vomiting, or retching), enteral feeding becomes mandatory. However, many metabolic, mechanic, or infections-related complications are frequently reported. 4 Prepyloric feeding includes an NGT or a feeding gastrostomy. In case of gastric emptying disorders, a postpyloric feeding is usually required: A nasojejunal tube, a trans-gastrostomy jejunal tube, or jejunostomy may represent temporary solutions for these patients.13,19 However, these devices are often hardly borne and may require several positioning maneuvers.
Bianchi's TEGD is a very interesting procedure. It is performed in selected cases, generally following GER recurrence or because of sialorrhea and swallowing disorders. Sialorrhea is a major problem in NIC, and many therapeutic alternatives have been described: anticholinergic drugs, physiotherapy, botulin toxin injection, and ligature of the salivary glands. Yet, all these possibilities have not been sufficiently discussed to achieve consensus. 9 Complete detachment of the stomach from the esophagus eliminates the risk of GER recurrence and the possibility of supraesophageal reflux-related complications, though the esophagojejunal anastomosis is performed in a very high position with a reported risk of anastomotic leakage with subphrenic collection. 9 Moreover, TEGD is a nonreversible procedure that implies gastrostomic feeding alone associated with a very limited amount of jejunum-compatible oral feeding. This necessarily means impossibility to taste and feel “normal” foods for any NIC undergoing such a procedure. The main goal of the proximal Roux-en-Y gastrojejunal diversion associated to antireflux surgery is to reduce GER recurrence and improve delayed gastric emptying.
The procedure differs from the Bianchi's bypass, as it maintains the normal viability through the stomach in case a good motility pattern is present. The gastrojejunal diversion represents an “escape valve” and may help the gastric emptying process in case of an impaired motility along the normal anatomic pathway. This cannot be considered as a complete standard bypass because no gastroduodenal resection is performed. Another potential advantage relies on the interruption of the posterior gastric musculature. This should reduce upward contraction waves and, subsequently, endoluminal pressures. Lower intragastric pressures should minimize the stress over the wrap and lower the risk of wrap disruption or herniation. This hypothesis has been confirmed by the good results obtained on postoperative imgaing and endoscopic study. In fact, none of the patients from our series experienced early macroscopic marginal ulceration at the gastrojejunostomy, though prolonged, full-dose PPI therapy is mandatory in order to limit acid-related damage to the jejunal mucosa. A longer, strict follow-up will be required in order to confirm these preliminary good results.
Artificial nutrition is advocated in NIC in case of clinical problems, such as recurrent pulmonary infections, when oral feeding is not possible, or when quality of life is unacceptable. Cachexia, vomiting, and aspiration pneumonia are the most frequently encountered complaints: Excluding oral feeding may be the only curative therapeutic measure. However, GER (re)occurrence and gastric emptying disorders often compromise the results of simple antireflux and/or gastrostomy procedures, leading to symptoms of persistence or complications highly affecting patient's quality of life and perspectives. We, therefore, suggest a single major procedure in order to reduce the numbers of general anesthesia and the related risk of complications. 23
Conclusions
This preliminary experience demonstrated that laparoscopic proximal Roux-en-Y gastrojejunal anastomosis, associated with Nissen fundoplication and feeding gastrostomy, is a valid alternative to the Bianchi's TEGD. A partial gastric bypass reduces gastric pressures and prevents wrap disruption or herniation due to altered gastric motility.
Footnotes
Disclosure Statement
No competing financial interests exist.