
Abstract
Abstract
Aim:
A prospective study to assess the clinical application of extracorporeal “Giant” locking sliding knot (GLSK) in pediatric and neonatal minimally invasive surgery (MIS).
Materials and Methods:
A total of 152 MIS, of various complexities were performed over a 14-month period with more than 1100 GLSKs used in 126 procedures.
Results:
There were no major complications or deaths in this cohort. Unraveling of the GLSK was observed in three instances (0.3%) secondary to excessive manipulation. Only a copolymer of glycolic acid/trimethylene carbonate material (Maxon™ suture; Covidien, Norwalk, CT) and polyproplene (Prolene™ suture; Ethicon, Sommerville, NJ) can be used for the GLSK technique due to their very smooth surface.
Conclusion:
Extracorporeal GLSKs can replace intracorporeal knots because they are safe, faster to tie, and reduce the surgeon's fatigue during complex MIS.
Introduction
The loss of depth perception and restricted space in the neonatal chest or abdomen are the most significant problems in performing IC knots for pediatric surgeons performing MIS on a regular basis, and actual procedural time in complex operations has remained longer than open surgery.1,2 This perhaps is the main reason for an increasing demand for robotics in developed countries.
IC knot-tying difficulties have reduced the desirability and acceptability of MIS for most pediatric surgeons. Another concern, but a rarely discussed problem of complex MIS, is that of mental fatigue experienced by the surgeon. 3 During knot tying, exact and quality apposition of tissues is particularly important for a successful outcome of the procedure (e.g., esophageal atresia repair) and most endoscopic surgeons perform a square (tumble) knot that is gradually tightened to achieve this (Fig. 1). Intense concentration is needed for IC knot tying and this in long, and complex procedures could cause irritability and fatigue in surgeons. Therefore, techniques that reduce the time required to tie a quality knot will result in a reduction of stress to the surgeons.
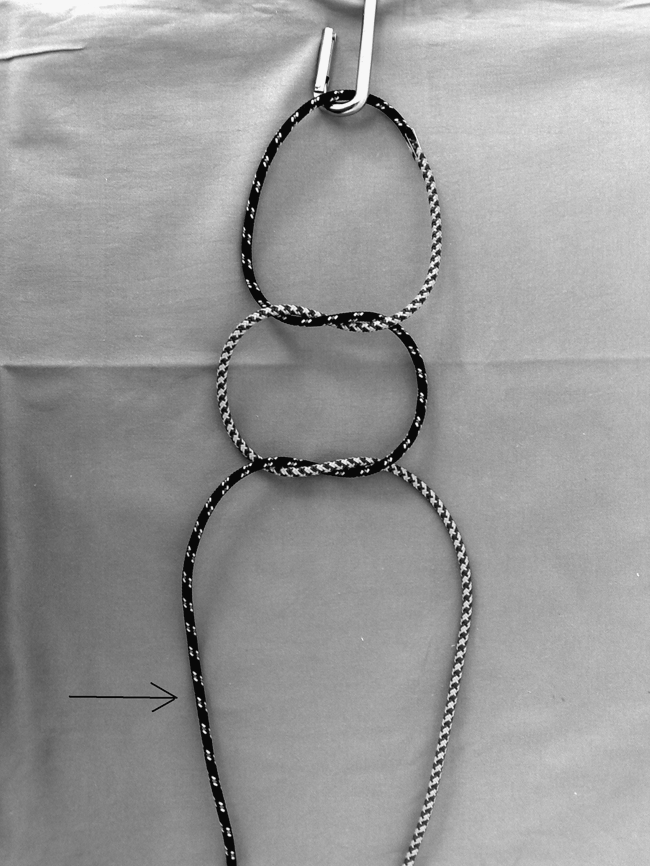
An intracorporeal (IC) square (tumble) knot: The first two alternate throws; the post strand (arrow) is pulled to tightened the knot intracorporally and a further two alternate IC throws are added to strengthen the knot.
A novel knot-tying approach has been adopted in orthopedic surgery for over two decades. Orthopedic surgeons routinely perform arthroscopic surgery in the cramped space of the knee joint by using a variety of extracorporeal sliding knots instead of intra-articular knot tying. There are as many as 26 sliding knots, including an important subset of six knots with an internal locking mechanism. 4 The easiest of these knots is termed the “Giant” locking sliding knot (GLSK) by Drs. Fleega, MD, and Sokkar, MD, for arthroscopic surgery. 5 Prior to its usage in clinical setting, strength studies for GLSK in an experimental model of esophageal atresia confirmed its overall strength at 12.90 N. This figure compared favorably to 13.1 N tolerated by standard square (tumble) IC knots. 6 In the present article, a comprehensive report on GLSK in pediatric and neonatal MIS is described.
Materials and Methods
A total of 152 pediatric and neonatal MISs were performed in a 14-month period (November 2007 to January 2009). GLSKs, instead of IC knots, were used in 126 operations (Table 1). GLSK consists of extracorporeal two overhand throws (similar to a surgeon's knot) followed by two further single overhand throws. The post strand is pulled and the knot slides through the cannula from an extracorporeal position into the body cavity. Once the desired target tissues are approximated, the loop limb is pulled to the opposite direction intracorporeally with a needle holder, which locks the knot in place (Figs. 2A–2D). A brief description of the “tricks” needed in utilizing GLSK is summarized in Table 2. To assess the time taken to achieve a conventional IC knot and a GLSK during MIS, the attending anesthesiologists were requested to time 50 GLSK and 50 IC square (tumble) knots by a digital timer.
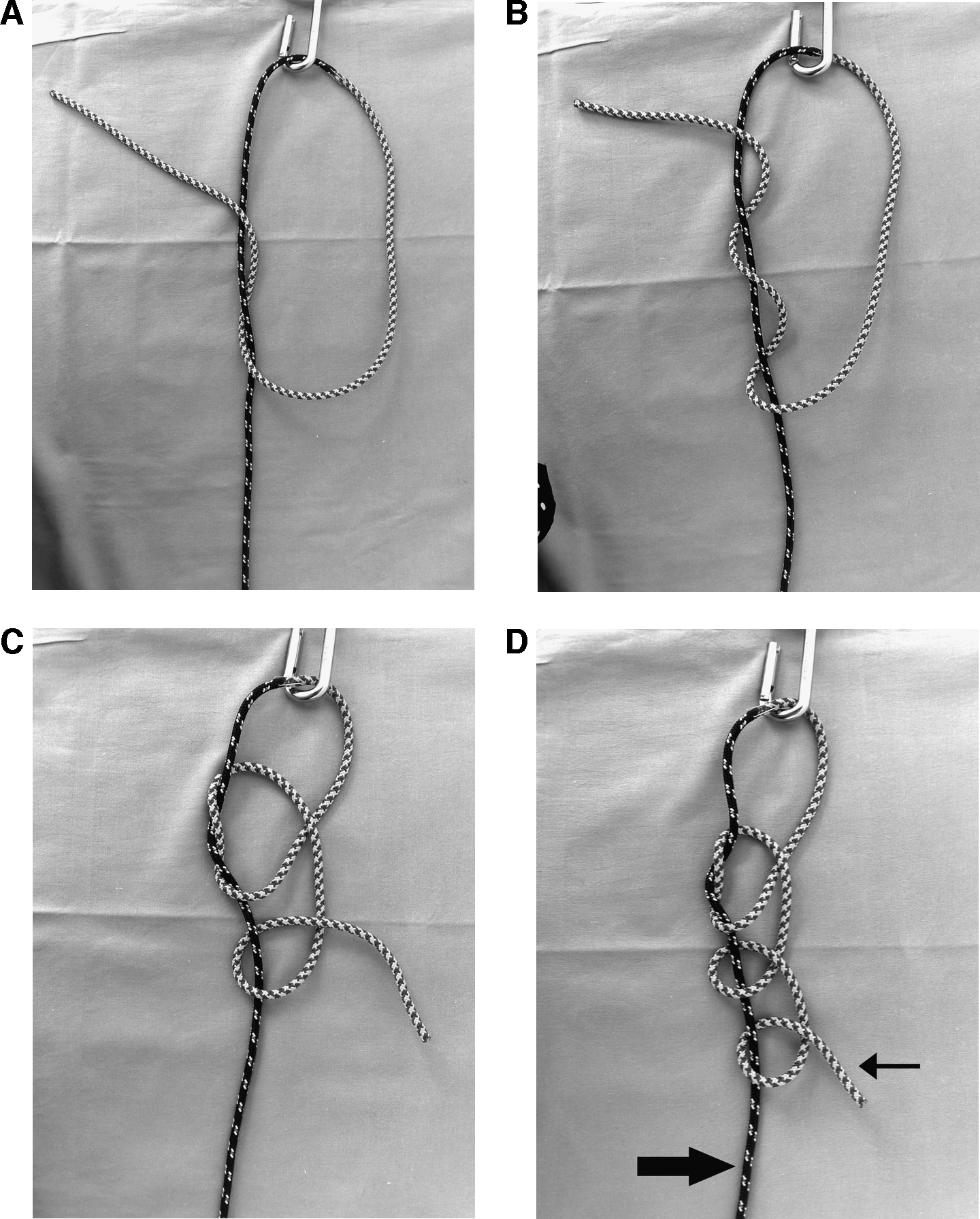
The Giant knot: (
GSLK, “Giant” locking sliding knot; CDH, congenital diaphragmatic hernia; ARM, anorectal malformation.
Congenital diaphragmatic hernia/eventration.
Anorectal malformation.
GLSK, “Giant” locking sliding knot; IC, intracorporeal; MIS, minimally invasive surgery.
Results
More than 1100 Giant knots were used in MIS for a variety of pathologies in this cohort of patients. All procedures were completed faster than anticipated due to GLSK usage. On average, it took 45 seconds (range, 25–70) to tie a GLSK, compared to 130 seconds (range, 80–220) for IC knots.
Morbidity was limited to four cases. A 3-mm cannula site became infected in a duodenal atresia repair case, a minor postoperative urine leak occurred in 1 infant after a retroperitoneal pyeloplasty procedure, and in 2 cases of extrapleural esophageal atresia repair, minor extrapleural leaks were detected on routine postoperative contrast study, which both healed within 7 days of conservative treatment (i.e., nasogastric feeding and intravenous antimicrobial therapy). There were no mortalities in this cohort.
Giant knot unraveled in three instances while being vigorously retracted upward during surgery, in one instance during repair of a congenial diaphragmatic hernia, and in another case, two knots unraveled during pneumovesicum bilateral ureteric reimplantation. Knots that require this type of manipulation are now reinforced routinely by a further two alternate stitches, using standard IC techniques. A smooth surface on the suture material in 5-0 or 6-0 suture size is necessary for the sliding of GLSK, limiting the types of suitable suture material to Maxon™ (Covidien, Norwalk, CT) and Prolene™ (Ethicon, Sommervile, NJ).
Discussion
Despite massive and explosive expansion of MIS in pediatric and neonatal conditions in the past 10 years, there is a consistent, substantial level of uneasiness by many experienced (and usually older) pediatric surgeons with this approach. One of the biggest concerns is difficulties encountered during IC knot tying in the confined and limited spaces of the neonatal thorax and abdominal cavities. A multitude of pre- or postsurgical congress IC-suturing courses are attended by many pediatric surgeons-in-training to overcome this issue. However, despite training, IC knot tying continues to be a worry in pediatric and neonatal MIS, especially in a situation when precise and quality anastomosis is crucial, such as in esophageal atresia, and may explain the reported increased rate of anastomotic leakage, compared to open thoracotomy approach.7–9
Similar concerns by orthopedic surgeons resulted in the development of many sliding knots, loosely based on various fisherman's and hangman's knots. The load or tension applied to the knot in orthopedic surgery is different to that needed in pediatric and neonatal MIS. For example, orthopedic surgeons secure only two or three knots to repair a ruptured tendon, which is expected to tolerate massive cyclical tension, which, at times, could be as much as 100 Newtons (N). 10 In comparison, in neonatal surgery, most suturing is done under minimum tension, for example, as little as 0.2 N for duodenal or esophageal atresia repair (personal readings), and a complete anastomosis is often done with 12–16 knots (Fig. 3). GLSK is more than adequate for this purpose.

Giant locking sliding knot usage during duodenoduodenostomy for duodenal atresia in a 1.6 kg premature neonate.
GLSK is easy to tie even with the finest of suture materials, but it can potentially unravel. It is, therefore, recommended that two to three additional alternate half-stitches should be used for reinforcement, as outlined earlier. Another important caveat, at least in neonatal MIS, worth reemphasizing is the suture material itself. Maxon and Prolene sutures are the only absorbable and nonabsorbable suture materials that can slide easily with this type of knot. Although other sutures did slide in experimental models, in the clinical neonatal MIS setting, popular sutures, such as 5-0 Polydiaxonone (PDS™; Ethicon, Somerville, NJ) did freeze midway during the sliding process, and therefore, its usage is not encouraged.
Like any other surgical techniques, there is a learning curve to master the GLSK technique, but this is short, in comparison to IC techniques. It is recommended that interested surgeons should practice the knot for 1 hour in a standard laparoscopic trainer “box” followed by usage in open surgery for at least a dozen cases (e.g., umbilical hernia repair or abdominal wall defect closure). Once the details of the techniques are mastered, usage of GLSK in MIS is the next step.
It is worth remembering that when using GLSK, as with many other extracorporeal sliding knots, there is no need for a ‘knot-pusher’. A gentle pull on the post strand leads to sliding of the knot toward the target tissue and a simple intra-corporeal ‘tug’ on the loop strand will then lock the knot in position. The surgeon holds the post strand suture and therefore can feel the knot as it is sliding towards the target tissue and its subsequent tightening as the tension on the suture is increased. He/she can then decide by this “feel” and visual inspection of the approximated tissue whether an adequate tension has been applied, prior to locking the knot in position. This ‘feel’ represents another advantage of GLSK compared to the IC knotting.
GLSK can potentially outshine robotic surgery, too. The main attraction of the Da Vinci® robot (Intuitive Surgical Inc., Sunnyvale, CA) is its ability in providing a three-dimensional image with the added bonus of a wrist-like action of the robotic arm to achieve IC knot tying. However, the costs of obtaining and maintaining a robot are prohibitive for most hospitals. In addition, the docking and moving of the robots are time-consuming. There is no additional cost for using the GLSK, and it can be done as quickly and securely as a robot.
Conclusion
In conclusion, this clinical evaluation of the Giant knot confirms and validates its value in the armamentarium of pediatric surgeons who wish to practice MIS on a regular basis. This report will hopefully ease some of the difficulties of MIS and should encourage pediatric surgeons around the world to undertake MIS more frequently.
Footnotes
Disclosure Statement
No competing financial interests exist.