
Abstract
Abstract
The management of long-gap pure esophageal atresia remains controversial. Treatment options include primary repair with or without circular myotomoies of the upper pouch, proximal and distal pouch dilation/stretching, colon/small intestinal replacement, and gastric transposition/pull-up. Of these options, only the gastric transposition can be performed in a completely laparoscopic approach. In this paper, we report a case of complete laparoscopic gastric transposition with cervical esophagogastric anastomosis in an infant with long-gap pure esophageal atresia.
Introduction
Case Report
An 8-month-old female with long-gap pure esophageal atresia was seen in referral for surgical management. Prior to surgical consultation at our institution, she had undergone open gastrostomy insertion for enteral feeds and her upper esophageal pouch was being controlled via a nasoesophageal tube, which was managed by her parents at home. She was gaining weight appropriately and had not suffered any complications related to aspiration events. Although she was currently healthy, her past medical history was significant for trisomy 21 and Tetrology of Fallot, for which she had undergone a primary repair at 6 months of age. A contrast study through her gastrostomy revealed a rudimentary distal esophageal stump with the proximal pouch located at the level of the esophageal inlet (Fig. 1).

A contrast study performed through the gastrostomy reveals a distal esophageal pouch of approximately 2 cm located at the level of the esophageal hiatus.
Operative approach
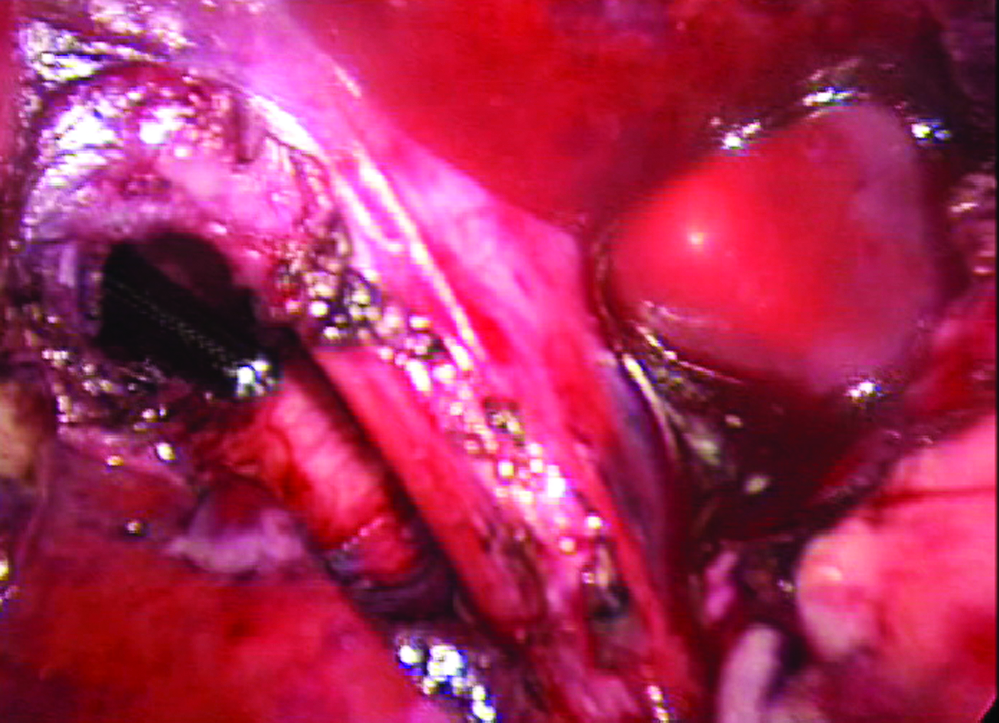
The patient was positioned at the end of the operating table in the frog leg position with her neck turned to the left. An 18-gauge nasogastric tube was inserted into the upper esophageal pouch. A metal dilator was inserted through the gastrostomy and into the distal esophageal stump. The dilator was pushed superiorly to evaluate the gap length between the proximal and distal pouches, which was greater than 6 vertebral bodies. It was decided that a primary repair would not be possible. The abdomen, chest, and neck were prepped and draped in a single surgical field. An approximately 12-mm incision was made vertically through the umbilicus and a 12-mm cannula was inserted into the abdomen. The abdomen was insufflated and one 5- and three 3-mm instruments were placed in the standard locations for laparoscopic Nissen fundoplication. Using blunt and electrocautery dissection, the gastrostomy was taken down from the anterior abdominal wall. The gastrotomy was then closed by using a GIA stapler (AutoSuture, Norwalk, CT). Attention was then focused on gastric mobilization. The greater curve was completely mobilized from the spleen by dividing the short gastric vessels, using electrocautery. The gastrohepatic ligament was opened and the lesser curve was mobilized from the pylorus to the esophageal hiatus. Great care was taken to protect the right gastric artery and the gastroepiploic arcades in order to ensure adequate blood supply to the gastric remnant. The left gastric artery was identified and ligated. The rudimentary distal esophageal stump was mobilized from the esophageal hiatus by using blunt and electrocautery dissection (Fig. 2). The gastric fundus was evaluated and the highest point identified as the site for esophagogastric anastomosis. The lesser curve of the stomach was also evaluated to determine the extent of gastric tapering that would be performed to allow an easily transposable gastric transposition through the mediastinum. Using a laparoscopic GIA stapler, the distal esophageal stump, and an appropriate portion of the lesser curve, was removed.

An intraoperative picture showing the rudimentary esophageal stump after being dissected from the esophageal hiatus.
The esophageal hiatus was enlarged to approximately 7 cm anteriorly by using electrocautery. The mediastinum was then approached. Using the 45-degree laparoscope and blunt dissection, the posterior mediastinum was dissected upward following the course of the descending aorta. In the upper mediastinum, the arch of the aorta was visualized and the dissection plane was carried upward toward the right thoracic inlet (Fig. 3).

A view of the posterior mediastinal dissection using a 45-degree 5-mm operating telescope. The aorta is located posteriorly and the dissection plane is being carried to the patients' right toward the thoracic inlet.
A right neck incision was made and carried down to the sternocleidomastoid muscle, which was retracted laterally. The nasoesophageal tube was palpated in the proximal esophageal pouch, and the esophagus was circumferentially dissected and freed from its distal attachments. Blunt digital dissection was carried out from the cervical incision toward the mediastinal dissection plane under direct laparoscopic visualization. Once the two planes had been joined, a large, curved clamp was passed through the cervical incision into the mediastinum under direct laparoscopic visualization (Fig. 4).
The large, curved clamp has been passed from the cervical incision into the abdomen through the esophageal hiatus. Note the position of the aorta immediately posterior to the clamp.
Sequential Hagar dilators were used under direct laparoscopic visualization to dilate the cervical mediastinal dissection plane to a size of 20 Hagar. This allowed for adequate room for the stomach to occupy the posterior mediastinum. The previously identified point on the gastric fundus was then grasped by using a large, curved clamp through the cervical incision and brought up into the cervical incision. After insuring appropriate gastric position across the diaphragmatic hiatus without significant tension, as well as adequate space in the posterior mediastinum, the fundus was opened and a standard two-layer esophagogastric anastomosis was created over the previously place nasoesophageal tube. Attention was turned back to the abdomen. The esophageal hiatus was inspected and the gastric transposition was found to be appropriately positioned, with no evidence for constriction due to the diaphragmatic musculature. A standard laparoscopic pyloromyotomy was performed (Fig. 5). Hemostasis was assured and the abdominal incisions were closed in the standard fashion.
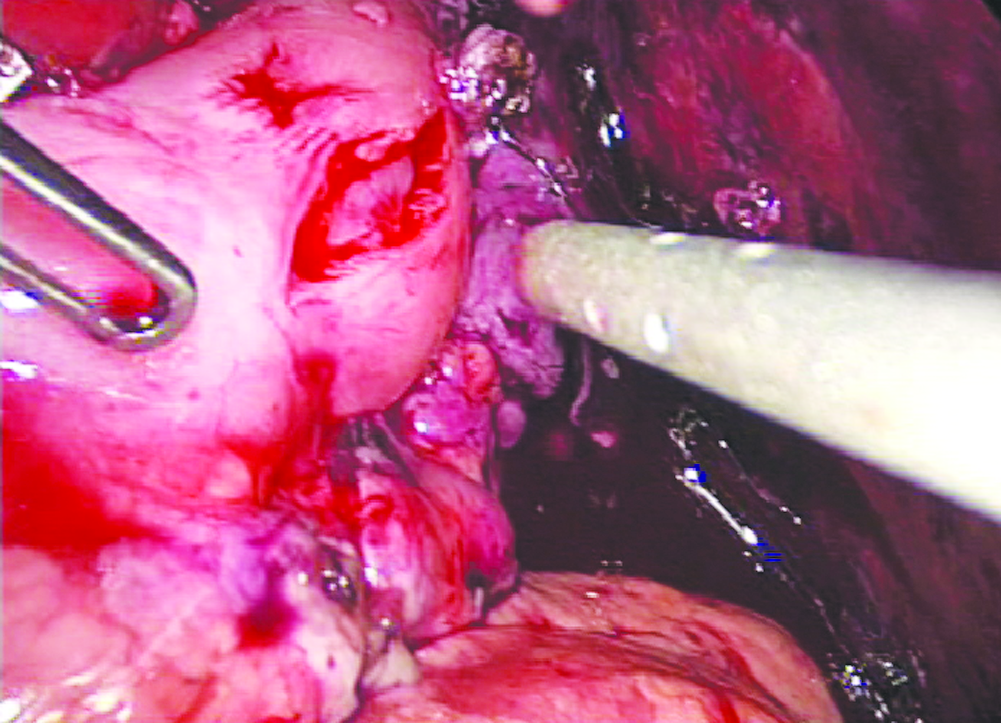
The completed laparoscopic pyloromyotomy showing complete separation of the muscle layers and bulging of the pyloric mucosa.
Postoperative course
The patient was extubated in the operating room and transferred to the intensive care unit (ICU) for monitoring. She was transferred out of the ICU on postoperative day 2. A contrast study of the esophagogastric anastomosis and intrathoracic stomach on postoperative day 7 revealed a widely patent anastomosis with no evidence of extravasation (Fig. 6). The transposed stomach emptied promptly through the pyloromyotomy. She developed a cervical wound infection with culture-positive methicillin-resistant Staphylococcus aureus on hospital 11, which responded to appropriate antibiotic therapy. Due to her oral feeding aversion, she received enteral feeds via a nasoduodenal feeding tube. The remainder of her hospital course was uneventful and she was discharged to home on postoperative day 17.
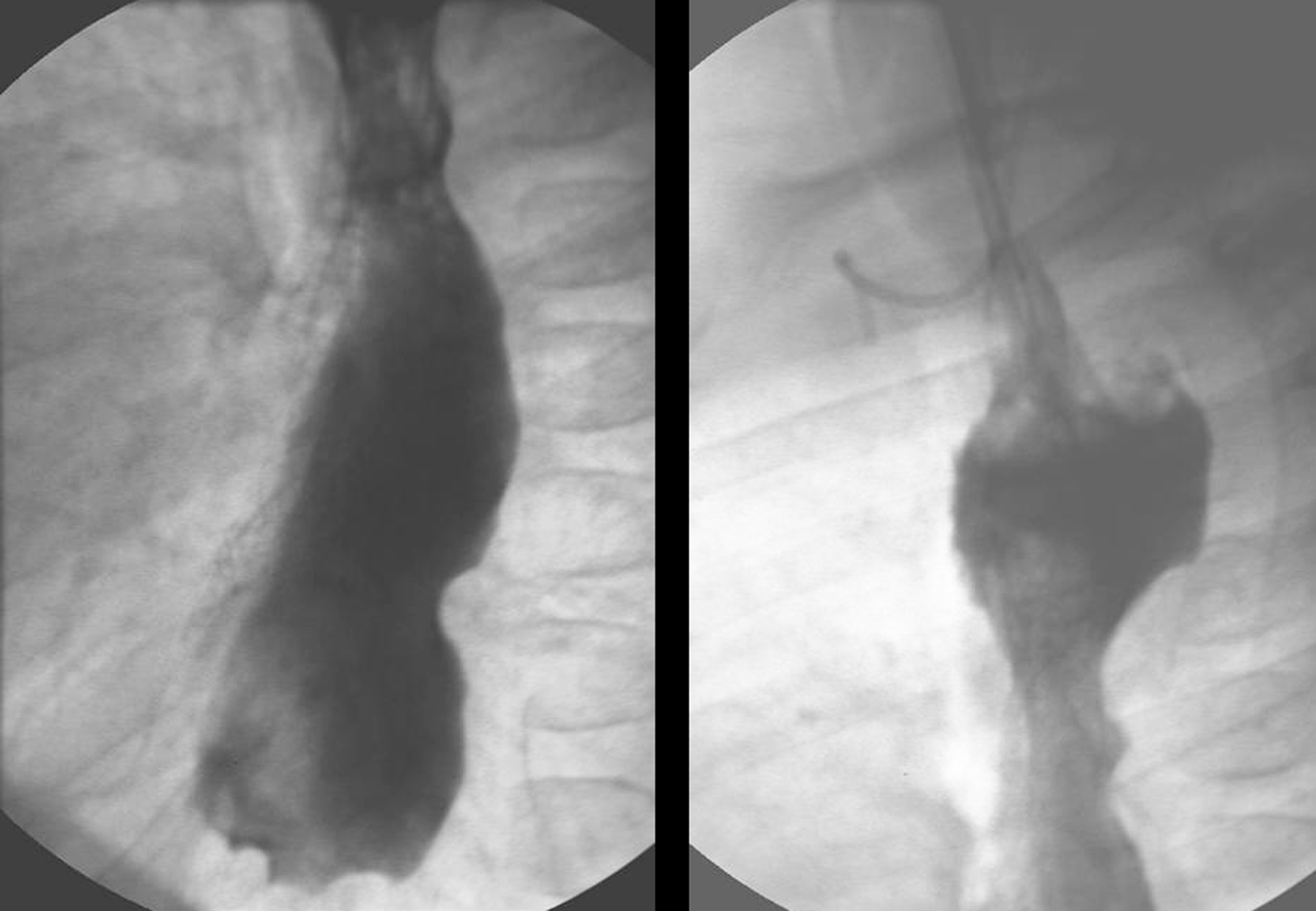
A contrast swallow revealed a widely patent esophagogastric anastomosis with prompt emptying of the gastric conduit.
Discussion
The management of long-gap pure esophageal atresia is predicated on historic techniques, using the colon or small intestine for esophageal replacement, with only recent data reporting success with using the stomach as a conduit. 1 The reported advantages of a gastric transposition include the technical aspects of a single anastomosis between the stomach and the esophagus in the neck, and the robust blood supply available to the stomach in comparison to the marginal blood supply of a colon or small intestinal interposition. The placement of a single esophagogastric anastomosis in the neck also has the advantage of having a controlled anastomotic leak, which will occur in about 12% of patients, rather than a leak into the thorax, which can be difficult to control as well as lead to significant anastomotic complications. 1 Ischemia to the colon or small intestinal anastomosis not only increases the risk for anastomotic leak (10–50%), but also predisposes to stricture formation (5–50%).2–6 Stricture formation at the site of the esophagogastric anastomosis in patients with esophageal atresia is uncommon (13%), given the size of the anatomosis as well as the robust blood supply. 1
Given the recent evidence that the gastric transposition appears to be the superior approach for esophageal replacement in infants with log-gap pure esophageal atresia, it is appropriate to consider approaching this technique via the laparoscopic approach. Technical considerations that are of utmost importance are understanding the blood supply of the stomach, especially in cases where a previous gastrostomy has been placed, complete mobilization of the stomach to allow for tension free placement in the posterior mediastinum, adequate opening of the esophageal hiatus to prevent delayed emptying of the gastric conduit, and identification of the most superior aspect of the gastric fundus that will be transposed and sewn to the esophagus. The size of the esophageal hiatus with respect to the gastric transposition should always be evaluated. The hiatus should be adequate in size to not allow for constriction of the gastric transposition to develop, while at the same time, be small enough to prevent herniation of an abdominal component into the posterior mediastinum. Although it was not necessary in this case, a consideration for suturing the stomach to the esophageal hiatus to prevent herniation should be undertaken in all cases. The posterior mediastinal dissection is performed in an expeditious, safe manner given the direct visualization afforded by the 45-degree laparoscope advanced through the esophageal hiatus. In fact, this portion of the operation is actually safer with using the laparoscope than it is when performed in the traditional fashion, which is via blunt finger dissection only.
Conclusions
Although the laparoscopic and thoracoscopic approach for esophagectomy has been reported in older children with a history of postcorrosive esophageal strictures,7,8 this is the first report of a complete laparoscopic gastric transposition in an infant with long-gap pure esophageal atresia. The complete laparoscopic approach can be performed in a safe, efficient manner, with an expected outcome similar to an open approach in this patient population. It should be considered as an alternative to the open approach for patients with long-gap pure esophageal atresia that require esophageal replacement.
Footnotes
Disclosure Statement
No competing financial interests exist.