
Abstract
Abstract
Aim:
In this article, we report our experience with diverticulectomies of symptomatic congenital bladder diverticula in children, which was performed by utilizing pneumovesicoscopy.
Materials and Methods:
Six boys, 4–8 years of age (mean, 5.6) underwent pneumovesicoscopic diverticulectomy at our institution from June 2007 to June 2008. There were 4 right-single diverticula and 2 double-left diverticula. Under cystoscopic control, after the cystopexy to the abdominal wall, a midline 5-mm trocar for a 0-degree telescope and two lateral 3-mm reusable trocars through the anterolateral wall of the bladder in the midclavicular line were introduced, insufflating the bladder with carbondioxide to 10–12 mm Hg pressure. The diverticulum/a were inverted into the bladder and the mucosa around the neck was circumcized by using scissors and a monopolar hook. The defect was sutured with interrupted sutures and the bladder was drained with a Foley catheter, which was introduced at the site of the 5-mm port, and a urethral catheter.
Results:
Mean operative time was 110 minutes. No major peri- or postoperative complications were recorded, except that the displacement of one of the lateral trocars that resulted in gas leakage in 1 case. The trocar was replaced and the procedure was completed. An ultrasound and a voiding cystourethrogram, performed from 3 to 6 months after the operation, showed the disappearance of the diverticulum/a.
Conclusions:
In our experience, pneumovesicoscopic diverticulectomy is an easy, safe procedure and can be considered a valid alternative to the open or laparoscopic procedures. It also provides no postoperative discomfort and a good cosmetic result.
Introduction
Materials and Methods
Six boys, 4–8 years of age (mean, 5.6), underwent pneumovesicoscopic diverticulectomy at our institution from June 2007 to June 2008. Three patients had a history of recurrent urinary infection (UTI), 2 of voiding disorders, and 1 of hematuria. In all patients, a bladder ultrasound (US) showed the presence of diverticula. The voiding cystourethrogram (VCUG) confirmed the diagnosis and failed to find evidence of vesicoureteral reflux (VUR) or infravesical obstruction: A single diverticulum of the right posterolateral wall of the bladder was present in 4 patients (Fig. 1) and a double-left lateral diverticula in 2 patients. The urodynamics showed overactive bladder in patients with voiding disorders.

Case 3, a 6-year-old boy: a voiding cystourethrogram, showing a posterolateral huge bladder right diverticulum.
Pneumovesicoscopic diverticulectomy was performed in all patients under general anesthesia. All patients voided their bladders before entering the operating room. The various steps of the operation were as follows. The patients were placed in the modified lithotomy position with abducted thighs, and the pelvis was tilted with the help of a cushion placed just below the buttocks. A cystoscopy with normal saline fluid distension was performed to verify the urethra, the ureteric orifices, and to determine the size, shape, and number of the diverticulum/a. A ureteral 3-Ch stent was then inserted at the site of the diverticulum.
With the bladder filled at medium capacity, the bladder wall was suspended to the anterior abdominal wall with two percutaneous transfixing sutures (no. 1 or no. 2 polyglactin stitches) placed under cystoscopic control or with a Reverdin needle in the oldest or most obese patients. The purpose of the sutures was to keep the bladder wall and the abdominal wall in close contact in order to stabilize the bladder and facilitate trocar entry. Under cistoscopic control, we introduced the first midline 5-mm trocar for a 0-degree telescope 1–2 cm below the umbilicus and two left and right 3-mm reusable trocars through the anterolateral wall of the bladder in the midclavicular line (Fig. 2). The bladder was then emptied and the cystoscope removed, insufflating, via the dome port, carbon dioxide at a pressure of 10–12 cmH2O and a volume of 2 L/min.

Case 3: view of the operative field.
The procedure required a 3-mm needle holder, a grasper, a pair of scissors, and a monopolar hook. The diverticulum/a were inverted into the bladder (Figs. 3 and 4) and the mucosa around the neck was circumcized by using scissors and a monopolar hook; the diverticular sac was then freed by sharply creating a plane between the detrusor muscle and the mucus membrane of the diverticulum and continuing the dissection along that plane (Fig. 5). When the dissection was completed, the closure of the defect was performed by a double layer with interrupted sutures of muscular and mucosal layers with 6/0 maxon or polyglactin, which could be easily passed through the 3-mm trocars or 5/0 stitches introduced in the bladder through the abdominal wall. The diverticulum/a were then removed under cystoscopic control through the 5-mm trocar, whole or divided in smaller pieces. At the end of the procedure, the ureteral stents and the cystopexy were removed. A 12-Ch Foley catheter, filled with 3–4 mL of sterile water, was introduced at the site of the 5-mm port through the cannula of the fractured trocar or with the help of a guidewire instead of suturing the port site. 8 The two sites of the 3-mm trocars did not require closure. The urethral and suprapubic catheters were removed 3 days after the procedure and the patients were discharged on day 4. All patients were kept on oral antibiotic prophylaxis for 3 months.
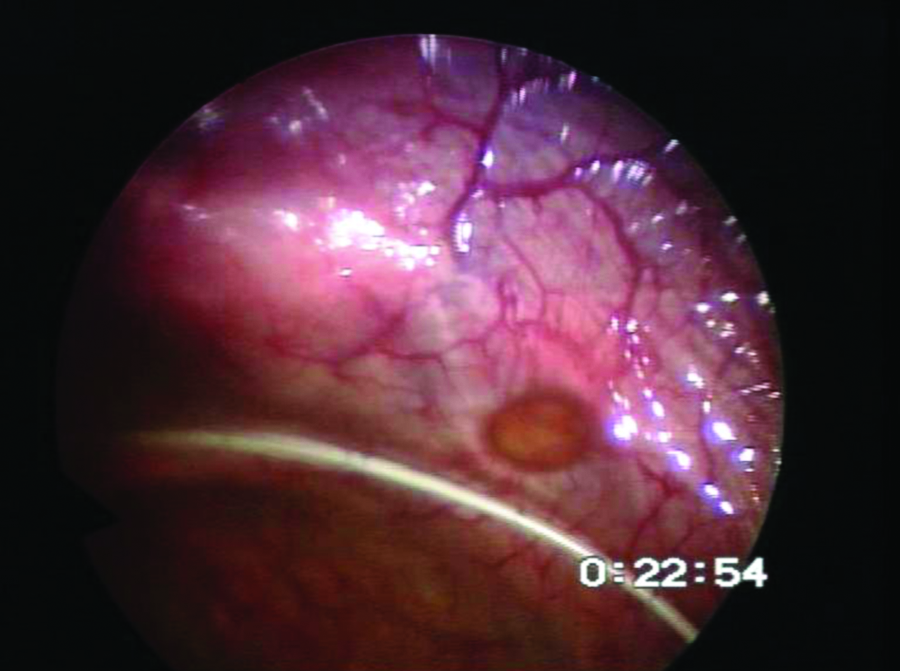
Pneumovesicoscopic view of the diverticulum.
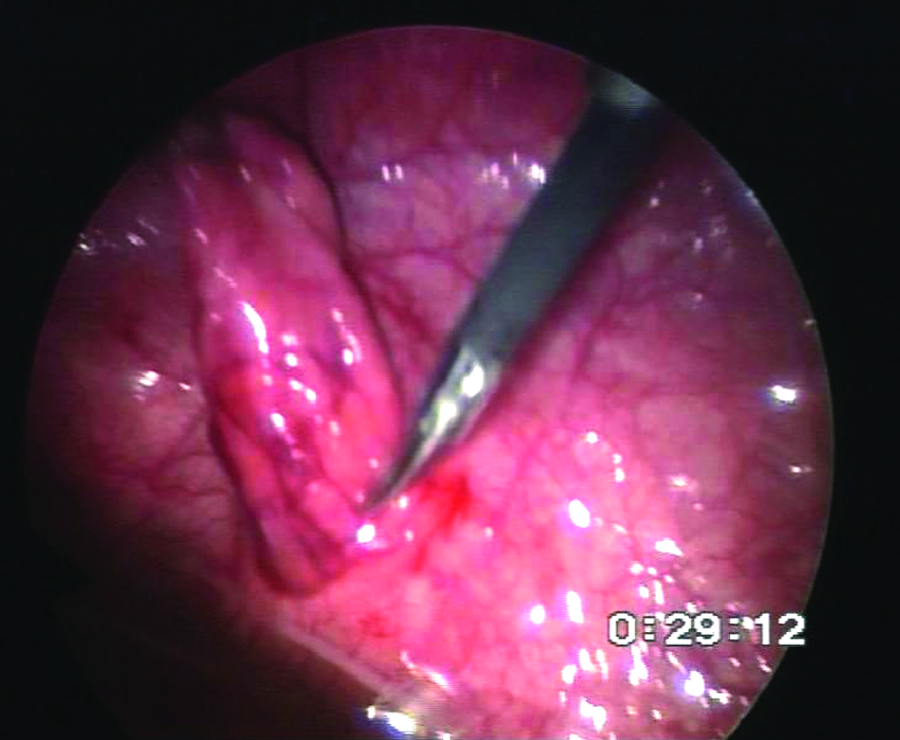
Pneumovesicoscopic view of the inverted diverticulum.

Resection of the diverticulum.
Results
Mean operative time was 110 minutes (range, 80–140). No major peri- or postoperative complications were recorded. The only intraoperative complication was the displacement of one of the lateral trocars outside the bladder, resulting in gas leakage in the extravesical space in the 8-year-old patient with double diverticula. In this case, the trocar was replaced with difficulty and, even if the gas prejudiced the intravesical space and the endoscopic vision, thus prolonging operating time, the procedure was completed. A US and VCUG (Fig. 6) were performed from 3 to 6 months after the operation, showing the disappearance of the diverticulum/a. The 2 patients with voiding disorders showed an improvement of their urgency, which was also confirmed by the urodynamic test.

Case 3: Postoperative voiding cystourethrogram showing no diverticulum or vesicoureteral reflux.
Discussion
In the last 5 years or so, pneumovesicoscopies have become part of the urologic procedures in the pediatric age group, in some institutions. The first experiences reported8,9 in children described the use of pneumovesicoscopy for the treatment of VUR and obstructive megaureter. These researchers concluded that the endoscopic intravesical ureteral mobilization and cross-trigonal ureteral reimplantation could be performed safely and effectively, with a success rate in reflux resolution as high as that with the open technique, but with minimal invasiveness and much faster recovery. 9 Nevertheless, some other researchers underline the long learning curve for this procedure and, given the limited working space, express the need for particular caution when considering its use in young patients with small bladder capacity. 10 Until now, the current treatment of symptomatic congenital bladder diverticula in children has been the open diverticulectomy either by the transvesical Kelalis technique 11 or the extravesical route. Another viable, successful technique is the standard or laparoscopic robotic-assisted diverticulectomy.6,7 The advantage of this technique is its mini-invasiveness, fast recovery, and short hospital stay. Nevertheless, the violation of the peritoneum is considered one of the major drawbacks of the transperitoneal approach. 6
More recently, Badawy et al. 12 reported their experience with pneumovesicoscopic diverticulectomy in children and adolescents. These researchers conclude that pneumovesicoscopic diverticulectomy is a feasible procedure that does not require a long learning curve; moreover, it is associated with shorter hospital stay, rapid recovery, and good cosmetic results. The results of our experience seem to confirm that the pneumovesicoscopy can be a safe, useful procedure. In our patients, this technique was adopted to treat three single and two double bladder diverticula, and in all cases, it was viable, safe, and not particularly difficult. We utilized the same procedure described by Valla 13 for the cross-trigonal pneumovesicoscopic reimplantation, using a median 5-mm trocar for the 0-degree telescope and two 3-mm operative reusable trocars inserted at both sides of the bladder wall, with the surgeon standing on the side opposite to the diverticula. The technique is different from the one described by Badawy et al., 12 who used a different position of the trocars and preferred the insertion of two 5-mm balloon trocars in the bladder along the midclavicular line opposite to the mouth of the diverticula. Regarding the use of the locking or balloon trocars,12,13 we do not have any experience with the use of these kinds of trocars to fix the bladder wall during the pneumovesicoscopy. In our patients, we routinely utilized the cystopexy with two transabdominal stitches and two reusable 3-mm trocars. This procedure is less expensive than the use of locking trocars, even if in our experience and from a revision of the literature,9,10 this can cause the dislodgment of the lateral trocars during the movements. In most cases, this does not represent a drawback because the replacement is easy, but in some cases this can result in a massive gas leakage in the extravesical space, making difficult the replacement of the trocar or requiring the conversion to open surgery. Therefore, in our opinion, the possibility of conversion to open surgery should be always considered in requiring informed consent. To our knowledge, this is the second report about bladder pneumovesicoscopic diverticulectomy in children, confirming that the procedure is safe and effective for removing single- or double-bladder diverticula. The pneumovesicoscopic access allows an easy identification of diverticula and facilitates the dissection by attracting the diverticulum into the bladder cavity. Moreover, this approach allows the correction of every other associated malformation, such as VUR, megaureter, ureterocele, and bladder neck surgery. The only drawback of the procedure is the need to suture in the small space represented by the bladder cavity, which requires sufficient skill. The pneumovesicoscopy offers the opportunity of integrating the transvesical and the laparoscopic extravesical approaches and all the advantages of a mini-invasive access. Additional advantages of this procedure are also the reduction of abdominal-wall and bladder trauma: in fact, there is no wide cystotomy and no mucosal irritation with gauze swabs. Other advantages of the technique may be the potential lack of postoperative hematuria or clot formation and bladder spasm due to the large detrusor opening. Direct diverticulectomy with mini-invasive access could also enable the surgeon to remove the diverticula and, at the same time, correct every other associated malformation, such as VUR. Pneumovesicoscopic diverticulectomy could also represent a first step for learning this technique, which can be useful for all intravesical and more complex procedures, such as the treatment of ureterocele, VUR, megaureter, and bladder neck surgery. In our opinion, the routine utilization of pneumovesicoscopy could become the gold standard for the treatment of all intravesical procedures, keeping, at the same time, the advantages of the open technique.
Conclusions
In our experience, vesicoscopic diverticulectomy is an easy, safe procedure and can be considered a valid alternative to the open or laparoscopic procedures. Pneumovesicoscopy also provides a rapid recovery, no postoperative discomfort, and a good cosmetic result. Pneumovesicoscopic diverticulectomy could also represent a first step for learning this technique, which can be useful for all intravesical procedures. Nevertheless, the number of patients evaluated in this study was too small to allow definitive conclusions to be drawn.
Footnotes
Disclosure Statement
No competing financial interests exist.