
Abstract
Abstract
Gastric transposition in children is a well-established treatment for long-gap esophageal atresia and long caustic strictures when preservation of the native esophagus is impossible, but does involve laparotomy and, often, thoracotomy incisions. The minimally invasive approach to this operation has been attempted in 7 patients to date in the UK, all at Great Ormond Street Hospital (London, UK). Four patients were male, 3 were female, with a mean age of 3 years and 7 months (range, 5 months to 13 years). Indications were long-gap esophageal atresia where primary anastomosis was impossible (5 patients) and caustic ingestion with long esophageal strictures (2 patients). The stomach was mobilized laparoscopically by using 5-mm instruments and a pneumoperitoneum of 10 mm Hg. Following pyloromyotomy or pyloroplasty, a tunnel in the posterior mediastinum was developed. The fundus of the stomach was drawn to the neck and sutured to the cervical esophagus. The patients were ventilated on our intensive care unit and then returned to the surgical ward before discharge. Gastric transposition was completed laparoscopically in 6 of 7 patients. The mean duration of surgery was 327 minutes (range, 240–455). All patients survived. Minor complications were pneumonia (2), pleural effusion (1), and hiatus hernia (2). The mean hospital stay was 16 days (range, 8–36). Our preliminary experience would suggest that laparoscopic gastric transposition is a safe alternative to open surgery with satisfactory results.
Introduction
Methods
We retrospectively reviewed our initial experience of laparoscopic gastric transposition at Great Ormond Street Hospital (London, UK). MIS has been undertaken in 7 patients to date. Four patients were male and 3 female, with ages ranging from 5 months to 13 years. Four patients were referred from within the UK (Lincolnshire/Essex/Wales) and three from abroad (Dubai/Norway). Indications were esophageal atresia, with a four to six vertebral body gap, and long corrosive esophageal strictures resistant to multiple endoscopic dilatations (Table 1).
Technique
Pediatric laparoscopic transpositions are performed either individually or jointly by the four consultant authors at Great Ormond Street Hospital. Under general anesthetic, with the patient postioned in the supine, a pneumoperitoneum of 10 mm Hg is induced via a 10-mm Hasson umbilical port. A Nathanson liver retractor is then inserted, as in a laparoscopic fundoplication, to allow access to the esophageal hiatus. Two small incisions are then made laterally for 5-mm instruments. After disconnection of the gastrostomy from the anterior abdominal wall, either a pyloromyotomy (Fig. 1) or pyloroplasty is performed, according to the preference of the operating surgeon.
Pyloromyotomy.
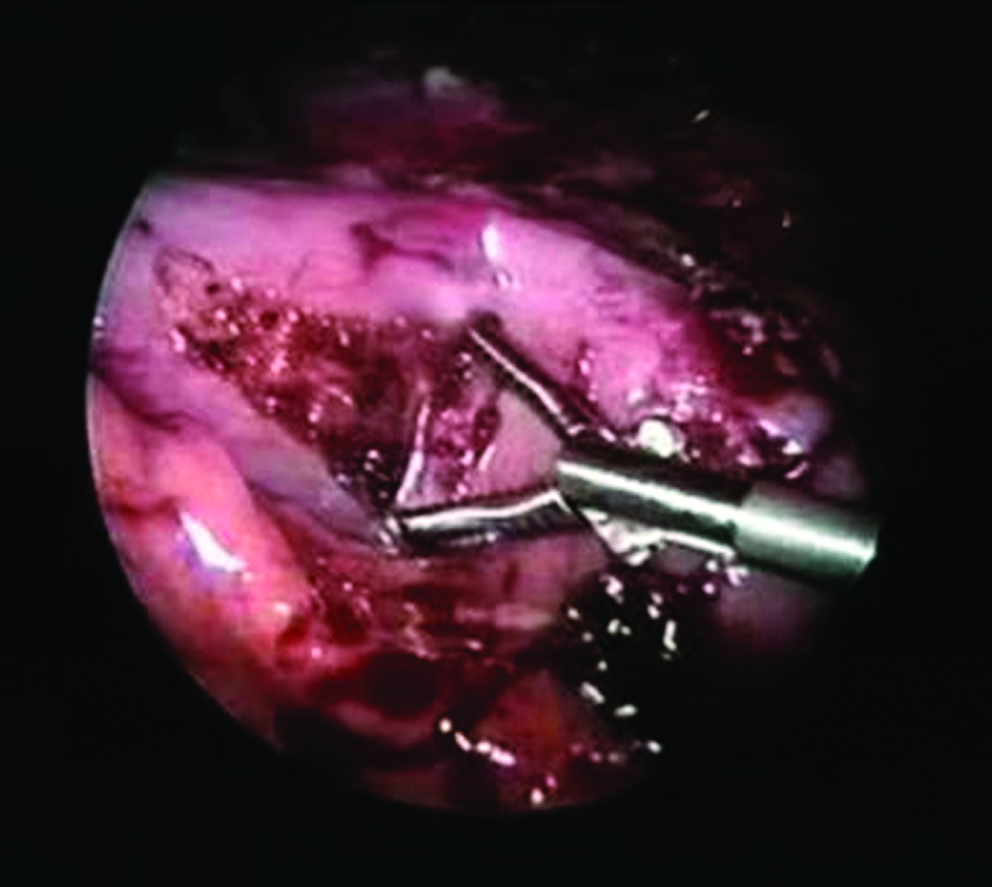
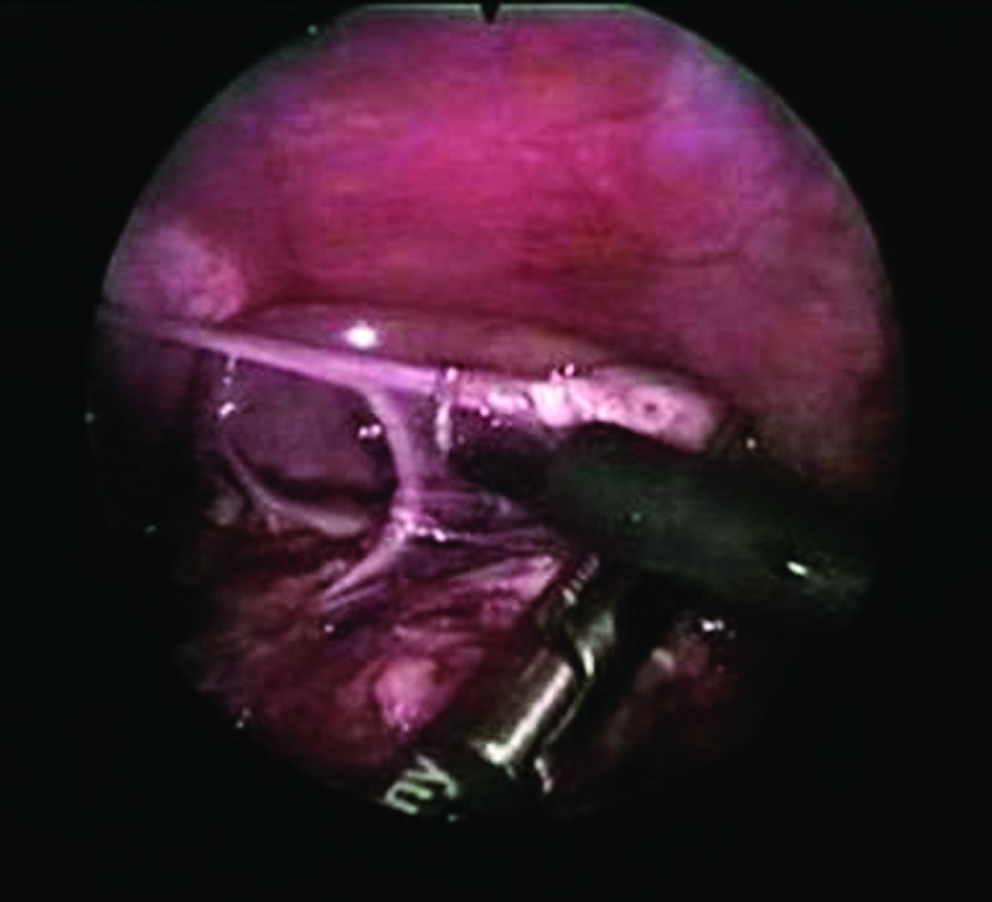
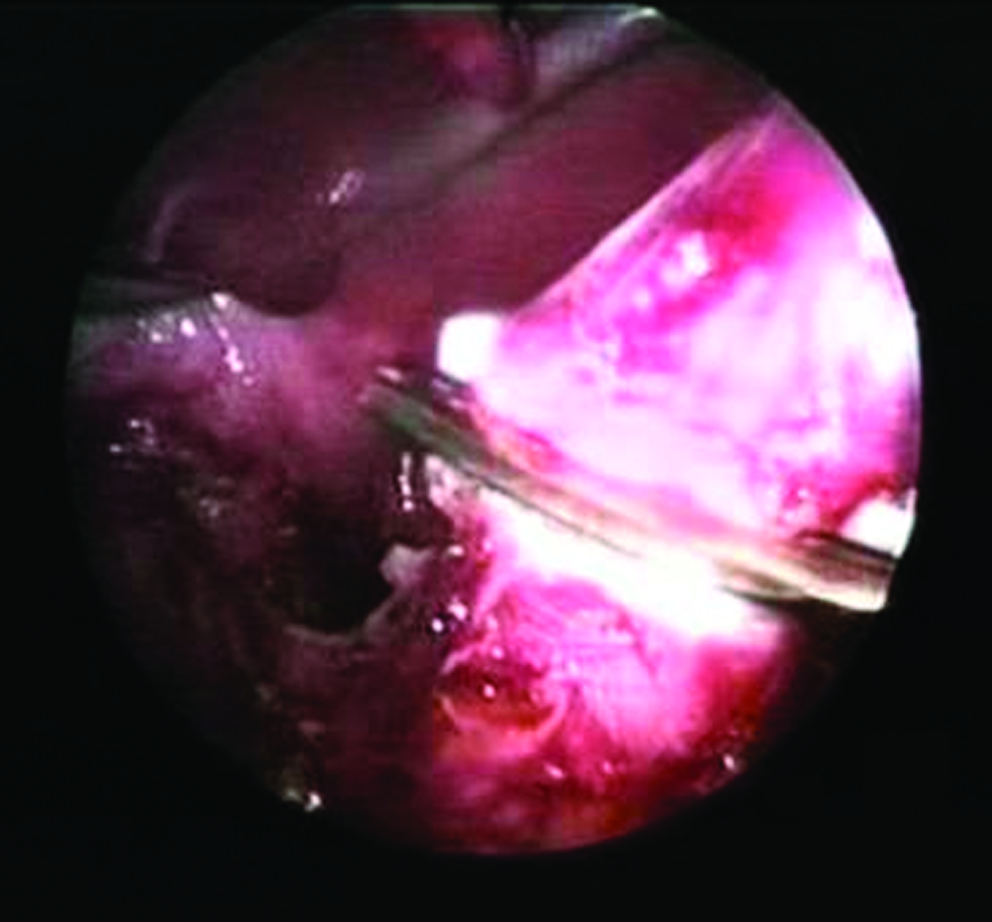
The stomach is carefully mobilized, using the Harmonic Scalpel to divide the greater omentum, gastrohepatic ligament, and short gastric vessels, with preservation of the gastroepiploic arcades and vagus nerves (Fig. 2). The distal esophageal stump is resected, using the Harmonic Scalpel (Ethicon, UK) (Fig. 3) and the stump securely oversewn. Following mobilization of the cervical esophagostomy, a posterior mediastinal tunnel is developed from above, using digital dissection. The posterior tunnel is developed from below, using blunt dissection and monopolar cautery. A long blunt-ended forceps and, then, increasing sizes of a Hegar dilator (Seward Thackray, UK) (Fig. 4) are used to dilate the track sufficiently to accommodate the transposed stomach. The camera can then be introduced into the posterior mediastinum to allow further development of the space under direct vision. Significant adhesions can be encountered in the mediastinum, especially if there has been corrosive esophageal injury. This may necessitate thoracoscopy (or thoracotomy) to divide safely.
Mobilization of the distal esophagus with preservation of the vagus nerve.
Resection of the distal esophageal stump.
Development of a posterior mediastinal tunnel, using a Hegar dilator.
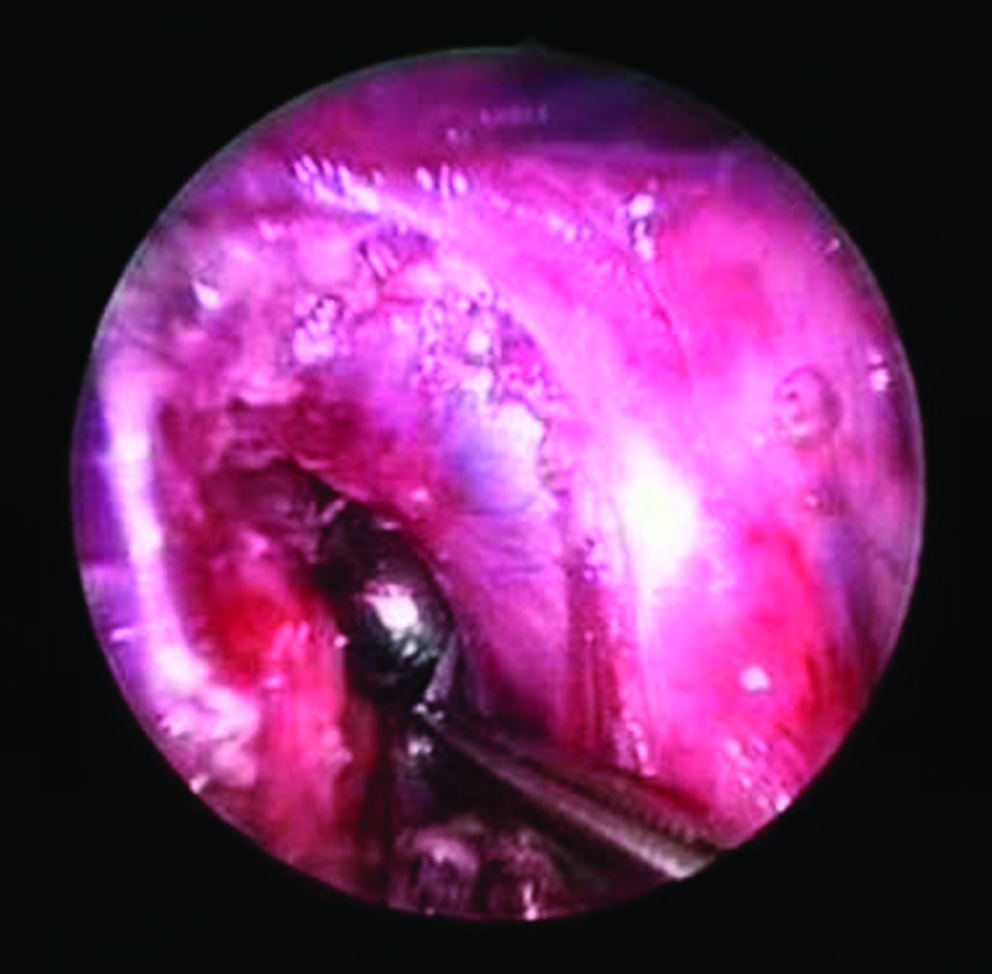
After securing the most proximal part of the fundus to the tip of an appropriately sized intercostal drain, using a nonabsorbable suture, the stomach is drawn into the neck and sutured to the cervical esophagus in a single-layer anastomosis, using interrupted sutures (Fig. 5). The wounds are closed with interrupted sutures, and the post sites are closed with tissue glue. A nasogastric tube is used, with the tip positioned in the middle of the mediastinum. If the chest is not opened, a chest drain is not required.

Elevation of the securely sutured proximal esophagus into the mediastinum, using an intercostal drain inserted via the cervical esophagostomy wound.
Postoperatively, patients are ventilated on the intensive care unit and then transferred to the surgical ward. Paralysis is required to prevent swallowing and movement at the esophagogastric anastomosis. Opiates are administered via a nurse-controlled pump system. Those children who have been feeding orally or regularly sham fed with esophagostomy can be managed without jejunostomy. Enteral feeds are commenced immediately if a jejunostomy is being used or when gastric function returns if oral feeding is expected. All are followed up at regular intervals in our outpatient clinic or at their tertiary pediatric surgical center abroad for 1–3 years.
Results
Results are summarized in Table 2. Gastric transposition was completed laparoscopically in 6 of 7 patients. In the 13-year-old boy with extensive corrosive strictures, dense adhesions between the liver and stomach from a previous open fundoplication precluded a laparoscopic approach, and an open transposition was subsequently performed. The mean anaesthetic time was 327 minutes (range, 240–455). All patients survived. There were no anastomotic leaks or strictures, either clinically or radiologically.
Early complications were pneumonia and pleural effusion in 2 patients. All were ventilated on the pediatric intensive care unit for 4–5 days. The mean hospital stay before discharge home was 16 days (range, 8–36). The 2 patients who developed postoperative pneumonia stayed on the surgical ward for a full course of intravenous antibiotics. Those with esophageal atresia were assessed for safe swallowing and oral feeds gradually established with specialist nursing support. A 5-month-old girl had a very prolonged stay due to a hospital epidemic of viral gastroenteritis.
Two patients had jejunal tubes placed at the time of surgery, one of which has since been removed as it was no longer required, and the other was used to supplement enteral nutrition. A patient with prolonged gastric paresis required a transpyloric tube, which has subsequently been removed after full oral feeds were established. Two patients developed a hiatus hernia and have since had these laparoscopically repaired. All children are now orally fed, swallow without difficulty, and parents report an excellent cosmetic outcome.
Discussion
Gastric transposition in children, first 1 described by Sweet in 1948, 2 was popularized by Prof. Spitz, MD, PhD, in the United Kingdom as a method of esophageal replacement when salvage of the native esophagus has failed 1 (Spitz 2009). In his experience (n = 192), he employed cervical and abdominal incisions, blunt posterior mediastinal dissection, and an additional lateral thoracotomy in 47% of cases to perform a transhiatal mobilization and single cervical anastomosis. Indications were long-gap esophageal atresia (138), corrosive strictures following caustic ingestion (29), and, rarely, peptic strictures (9). Patient age ranged from 7 days to 17 years. Median postoperative ventilation time was 4 days. Mortality (4.6%) was attributed to cardiopulmonary failure in patients with multiple previous attempts at esophageal replacement. Morbidity included anastomotic leakage (12%), strictures requiring dilatation (20%), initial swallowing difficulties (30%), delayed gastric emptying (9%), jejunal tube complications (4%), and dumping syndrome (3%). Nevertheless, long-term outcomes compared favorably with other methods of esophageal replacement (normal eating habits or only occasional dysphagia in 90%).
Minimally invasive esophagectomy, while well described in adult practice, remains an emerging technique in pediatric patients.3,4 Cury et al. described the use of thoracoscopic esophagectomy in 2 children with strictures, but use of a laparotomy incision in both cases to mobilize the stomach did little to limit the nature of the open insult. 5 In a report from Pittsburgh, Nwomeh et al. described a combined thoracoscopic and laparoscopic approach in a 17-year-old girl with a long corrosive esophageal stricture. 6 The procedure took 7 hours, and the researchers cautioned that the technique required advanced laparoscopic and thoracoscopic skills as well as experience in open pediatric oesophageal surgery.
Shalaby et al. recently reported the only pediatric case series in the literature to date. 7 Twenty-seven children underwent laparoscopic transhiatal esophagectomies and gastric transpositions for corrosive strictures at Al-Azhar University Hospital (Cairo, Egypt) and Dar-Alshifa Hospital (Kuwait City, Kuwait) between 2000 and 2003. Their ages ranged from 3 to 13 years. Eight had lower third, 12 middle third, and 7 multiple esophageal strictures. Several esophageal dilatations were performed before surgery was undertaken. None had previous abdominal surgery or comorbidities. All procedures were performed by the same operating surgeon. The researchers report an impressive mean operating time of 160 minutes and hospital stay of 4 days. Complications included anastomotic leakage (11.1%), strictures (14.8%), and pneumothorax requiring intercostal drainage (3.7%). In the longer term, 29.6% had reflux, but all could swallow without difficulty, were thriving on oral feeds, and cosmetic results were deemed excellent. The researchers conclude that the technique has significant advantages over the open approach in terms of hospital stay, reduced complication rate, and cosmetic outcome.
Conclusions
Our preliminary experience would suggest that laparoscopic gastric transposition is a safe and viable alternative to open surgery, with potentially improved outcomes in terms of mortality and morbidity. It should only be performed in centers with considerable experience in the open technique. The laparoscopic approach may be contraindicated in severe caustic strictures and/or significant previous abdominal surgery where dense adhesions make mobilization difficult. We have not yet encountered any significant leak or stenosis in this series, but we conclude that it remains an early time in our experience. It can be difficult to judge the gap at the esophageal hiatus as, on some occasions, the stomach will retract into the chest. It may be worth repairing the esophageal hiatus prophylactically after the cervical anastomosis is complete to avoid development of hiatus hernia (and need for reoperation) in later life.
Footnotes
Disclosure Statement
No competing financial interests exist.