
Abstract
Abstract
Background:
The aim of this study was to describe our technique of combined endolaparoscopic approach to the management of intraluminal gastric neoplasms and to review the clinical outcome.
Methods:
Between February 2006 and January 2008, a total of 12 patients with gastric neoplasm ≤4 cm with a mainly intraluminal component received the combined endolaparoscopic intragastric excision and were prospectively analyzed. All lesions were localized endoscopically and then treated by using a combined endoscopic submucosal dissection and laparoscopic intragastric technique.
Results:
Eight of 12 lesions were gastrointestinal stromal tumours. The remaining lesions were adenomatous polyp with focal intramucosal adenocarcinoma, leiomyoma, and pancreatic heterotopia. All except 1 case was successfully treated with this technique (91.6%). There were no mortalities, and there was only 1 case of reactionary hemorrhage from the port site requiring a reoperation. The median operating time was 120 minutes, with a median blood loss of 35 mL. Length of hospital stay ranged from 3 to 12 days. There were no recurrences during the follow-up period.
Conclusions:
This combined endolaparoscopic intragastric excision technique is a truly minimally invasive alternative for selected gastric neoplasm. It is safe and feasible with a satisfactory short-term outcome.
Introduction
Patients and Methods
A total of 12 patients were included to receive the ELITE procedure for the excision of gastric tumors between February 2006 and January 2008. This group consisted of 7 men and 5 women, with a median age of 73 years (range, 47–83). The selection criteria included gastric tumors ≤4 cm in maximum diameter without an extramural component that were not located at the anterior gastric wall. Lesions that were located at the anterior gastric wall would undergo a laparoscopic wedge resection or limited laparoscopic gastrectomy. Preoperative investigations included esophagogastroduodenoscopy (OGD) with biopsy, endoscopic ultrasound (EUS), and computer tomography (CT) to identify the nature and location of the lesion. Obvious malignant lesions with lymphatic and/or peritoneal involvement were excluded.
Operative techniques
The patient is positioned in the modified lithotomy position with a reverse Trendelenburg tilt under general anaesthesia. A 10-mm 30-degree laparoscope is introduced through a subumbilical port following carbon dioxide (CO2) insufflation up to 10 mm Hg. A 10-mm accessory port is inserted under direct laparoscopic guidance for the application of a laparoscopic detachable DeBakey clamp at the proximal jejunum (Fig. 1). This allows maximum stomach distension for the percutaneous insertion of intragastric ports while avoiding distension of the distal bowel, which would obscure the laparoscopic view.
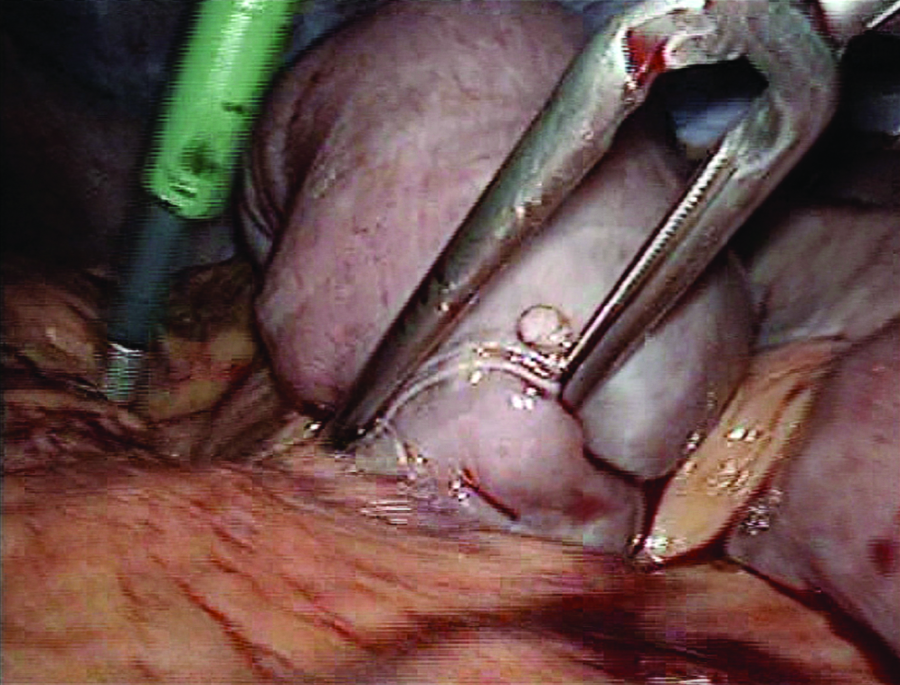
Laparoscopic insertion of detachable small bowel clamp to avoid distension of the distal bowel.
The position of the laparoscopic surgeon is variable, depending on the location of the lesion, but in general, for lesions located in the upper part of stomach (i.e., fundus/cardia), the operating surgeon stands between the patient's legs, and for lesions located in the lower part (i.e., antrum/pylorus), the operating surgeon is positioned on the left side of the patient (Fig. 2).

Operative setup. Positions of surgeon 1 and assistant 1 when operating on antropyloric lesions. Positions of surgeon 2 and assistant 2 when operating on lesions located at the fundus/cardia.
Intraoperative gastroscopy
The indications for intraoperative gastroscopy are as follows: 1) to identify the exact location of a tumor, as they are intraluminal and cannot be identified laparoscopically, 2) to facilitate the percutaneous insertion of intragastric ports, 3) to perform ESD, and 4) to retrieve the specimen. A single-channel gastroscope is introduced perorally with an overtube, and the stomach is distended with CO2. The subsequent percutaneous insertion of three 5.5-mm intragastric ports is performed under direct vision from the gastroscope. Their positions are variable, depending on the location of the lesion, but the principle of triangulation of the working ports and laparoscope should remain, and it is preferable to allow at least a 3-cm separation between the intragastric ports to permit adequate range of movement. The intragastric ports, Pediports™ (United States Surgical, Norwalk, CT), used by us, have a unique rotating actuator and woodford spike that elevate and fix the gastric wall to the anterior abdominal wall (Fig. 3).
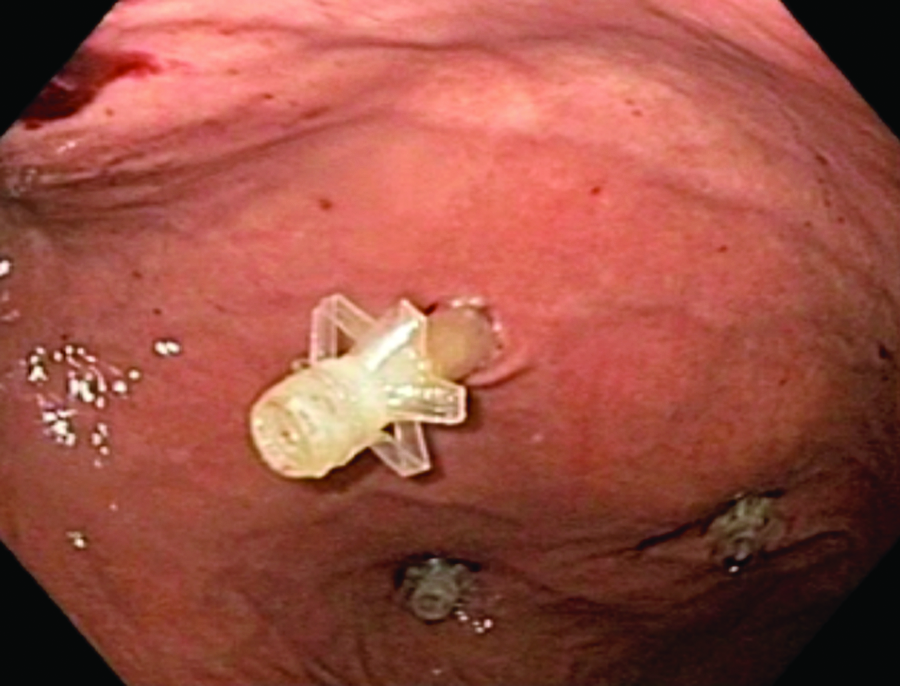
Percutaneous insertion of Pediports™ (US Surgical, Norwalk, CT) under direct endoscopic guidance.
Techniques in excision
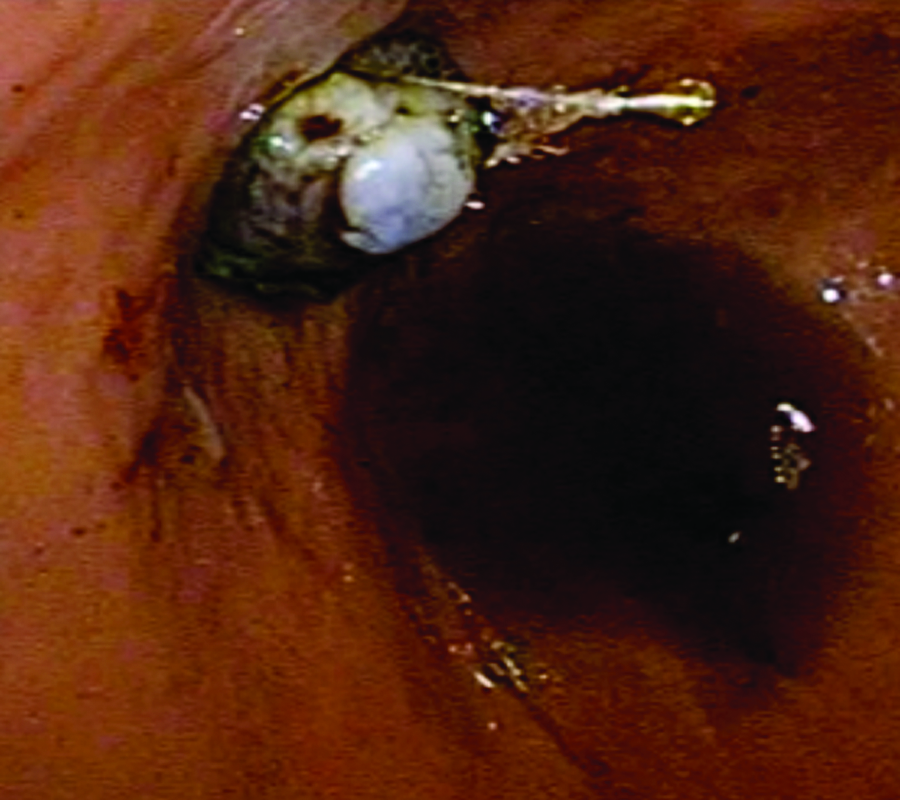
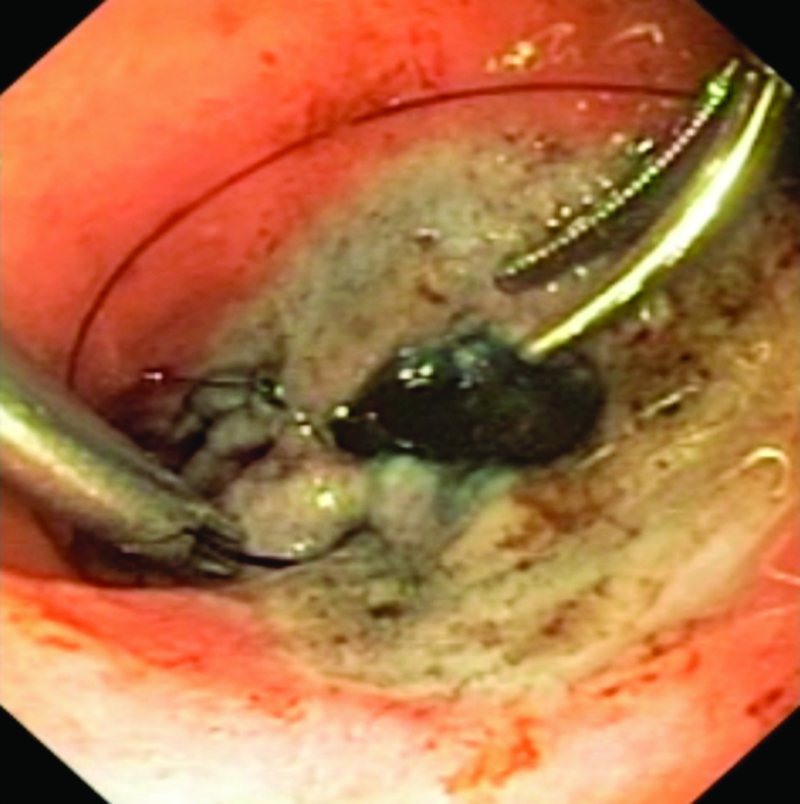
All lesions are initially dissected using the conventional ESD technique. 5 Following mucosal marking of the planned resection margin using endoscopic cautery (via needle knife), the submucosal plane is raised by using normal saline, adrenaline, and an indigo-carmine injection mixture. The mucosa around the lesion is incised, and the submucosal dissection is performed with an insulation-tipped diathermy knife (IT knife; Olympus Medical Systems Corp., Tokyo, Japan) with the 80W ENDO-CUT mode, effect 3 (ERBE) (Fig. 4). The subsequent seromuscular dissection is completed using laparoscopic ultrasonic dissector device via intragastric ports aided by counter retraction using laparoscopic forceps (Fig. 5).
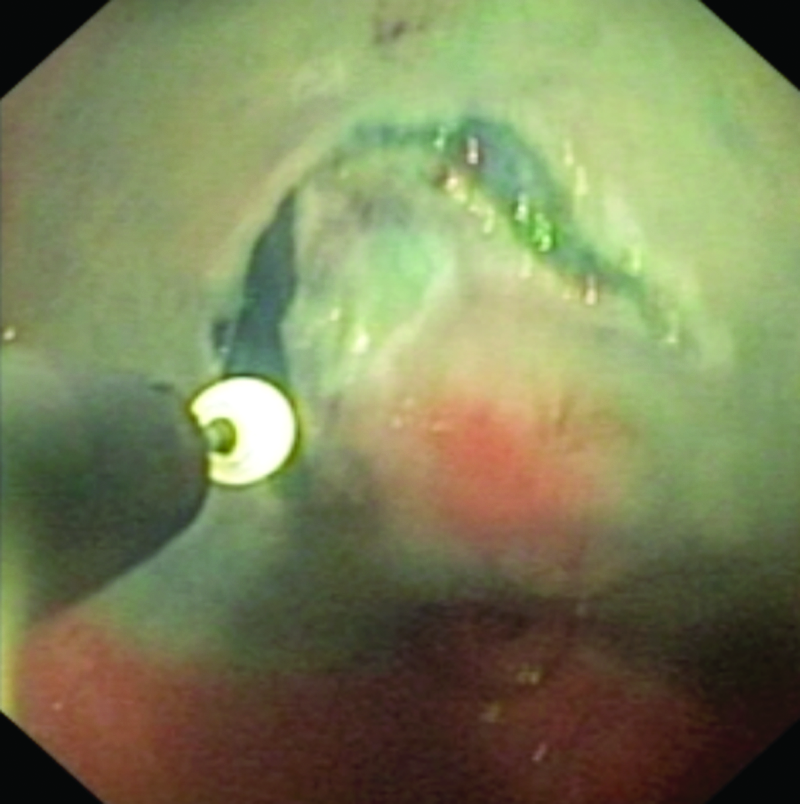
Endoscopic submucosal dissection using an IT knife (Olympus Medical Systems Corp., Tokyo, Japan).
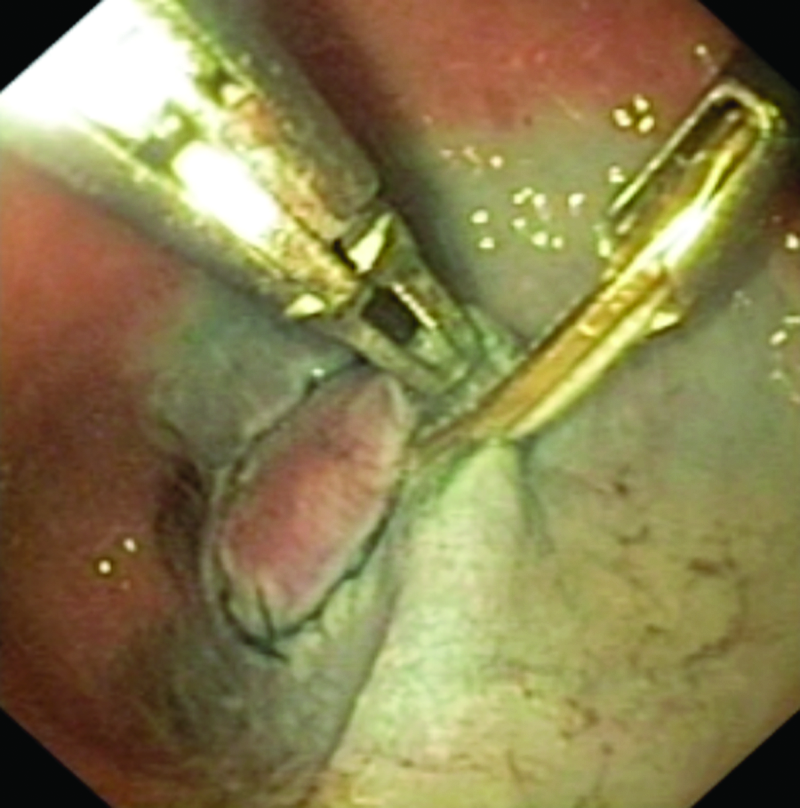
Laparoscopic-assisted dissection.
The resected specimen is retrieved transorally inside an endoscopic retrieval bag, Roth Net™ (US Endoscopy, Mentor, OH) (Fig. 6) The non-full-thickness resection defect is closed intragastrically, and the full thickness transgastric port-site defects are closed extraluminally, using 3/0 intracorporeal absorbable sutures (Fig. 7). At the end of the operation, the detachable DeBakey clamp is retrieved and a nasogastric tube is inserted for decompression. Abdominal drains are not routinely inserted.
Transoral extraction of a specimen.
Intragastric closure of a defect.
Results
Patients' presenting symptoms, preoperative diagnosis, final pathology, resection margin, location, operative techniques, operation time, blood loss, length of hospital stay, and complications are summarized in Table 1. Of the 12 resected specimens, 8 were gastrointestinal stromal tumors, all of which had clear resection margins. Patient 3 was under investigation for symptomatic anemia, and during OGD, a 25-mm adenomatous polyp with active oozing was found at the antrum, requiring endoscopic hemostasis. Following complete resection by ELITE, this polyp was incidentally found to have focal intramucosal adenocarcinoma. The resection margin was clear. However, immediately postoperatively, this patient suffered hypovolemic shock and fresh blood was noted to be oozing from one of the trocar-site wounds. Relaparoscopy showed active bleeding from that trocar wound due to accidental injury of the inferior epigastric artery. Hemostasis was achieved with plicating sutures, and she recovered uneventfully. Patient 7 had a preoperative diagnosis of GIST that, in fact, turned out to be leiomyoma. Patient 10 had an endoscopically suspicious lesion at the cardia, but despite repeated multiple biopsies, histology did not reveal any malignancy. Since she was reluctant to undergo a radical resection, we, therefore, offered her ELITE. Histology from the resected specimen confirmed a well-differentiated adenocarcinoma but with distal resection margin involvement. She subsequently received laparoscopic-assisted total gastrectomy and recovered uneventfully.
GIST, gastrointestinal stromal tumour; ESD, endoscopic mucosal dissection, ELITE, endolaparoscopic intragastric tumor excision.
Eleven of 12 patients successfully underwent the ELITE procedure (91.6%). The 1 unsuccessful case was due to the unexpected extramural component of GIST, despite preoperative investigations, resulting in a failed ESD. It was converted to laparoscopic transgastric resection using Endo-GIA linear stapling device (United States Surgical, Norwalk, CT). Six lesions were located in the upper part of the stomach (4 at the cardia and 2 at the fundus) and 3 in the antropyloric region.
The median operation time was 120 minutes (range, 44–225), with a median blood loss of 35 mL (range, 5–250). Mean length of stay was 4.5 days (range, 3–12) without intensive care unit admission. There was no operative mortality. All patients were followed up with surveillance OGD 1 month postoperatively and, thereafter, half-yearly. None of these patients had evidence of tumor recurrence during the median follow-up period of 8.5 months (range, 1–24).
Discussions
Minimally invasive surgery is ideal for benign gastric neoplasm and early gastric cancer, because lymphatic spread is rare, and therefore, local resection is sufficient.4,8 Laparoscopic resection is currently the standard treatment for gastric GIST. 9 Due to their variable location and degree of extramural or intraluminal component in the stomach, methods of laparoscopic resection are extremely diverse. As such, a tailored approach should be adopted in individual cases to ensure the best functional and oncologic outcome. 11
Laparoscopic wedge resection, using endoscopic stapling devices, is most commonly performed and can be easily applied to lesions in the anterior gastric wall. Stapling devices can also be used for posterior wall lesions as in laparoscopic transgastric resection via anterior gastrotomy. One of the drawbacks of using stapling devices is their inflexibility. This often results in excessive tissue loss and, therefore, inaccurate resection margin. For the management of GIST, where a resection margin per se is not essential as long as the tumor capsule is not breached, this may result in functional loss where lesions are located close to the esophagogastric junction (OGJ) and pylorus. In these cases, an open resection with partial gastrectomy will most likely be required prior to ELITE.10–13 In our series, of the 4 patients with such located lesions who had undergone ELITE, none complained of postoperative obstructive symptoms during the follow-up period. The preserved function in these patients is due to the accurate endoscopic mucosal and submucosal dissection combined with the suture-closure technique.
The main selection criterion for ELITE is intraluminal lesion, as we believe this maximizes the complimentary roles between endoscopy and laparoscopy. In these circumstances, the laparoscopic localization of small intraluminal lesions alone is extremely difficult unless guided by laparoscopic ultrasound or endoscopy.14,15 Although the management of asymptomatic GIST ≤5 cm is controversial, complicated lesions (i.e., with ulceration) should ideally be excised to prevent symptom recurrence and related morbidities, as shown in our 5 cases that presented with bleeding. Further, these small lesions (≤4 cm) can easily be retrieved transorally without the need to extend the port-site wound, thus minimizing morbidities associated with access trauma.
Endoscopic mucosal dissection is a well-established treatment for early gastric cancer that is confined to the mucosa and submucosa layers. Evidence from large study series has confirmed its feasibility and excellent outcome, even for extensive dissection, regardless of size for nonulcerating tumor.16,17 In ELITE, where ESD is performed for lesions in the muscular layer, the endoscopic seromuscular dissection is often difficult due to vascularity and high risk of perforation. Therefore, in order to successfully complete the seromuscular dissection and to close the gastric defect, additional instruments are required. The concept of laparoscopic and endoscopic cooperative surgery (LECS) was first introduced by Hiki et al. 18 LECS combines ESD with laparoscopic stapling devices for closure of the defect, instead of using laparoscopic suturing techniques as in ELITE. Similar to LECS, the reported cases of the ELITE method of defect closure did not result in any morbidities and could be achieved with a comparable operation time.
Conclusions
In conclusion, ELITE for selected gastric neoplasms is feasible and can be performed safely with a satisfactory outcome. Its indication for small lesions with a mainly intraluminal component allows a truly minimally invasive alternative to other laparoscopic approaches.
Footnotes
Disclosure Statement
No competing financial interests exist.