
Abstract
Abstract
Purpose:
We aimed to investigate the role of the carbon-dioxide (CO2) pneumoperitoneum on the prevention of postoperative adhesion formation.
Methods:
Thirty adult male Sprague-Dawley rats (250–350 g) were used for this study. The rats were randomly divided into three groups; in the sham group (n = 10) only, laparotomy was made, in group 2 (n = 10), a pneumoperitoneum was applied for a half-hour duration, followed by laparatomy, and in group 3 (n = 10), pneumoperitoenum time was 2 hours and after a pneumoperitoneum laparotomy was made. A cecal abrasion model was studied for making an adhesion formation. On day 14, all rats were sacrificed and adhesions were scored. Tissue samples from adhesions and peritonea and the cecum wall were examined, both pathologically and biochemically, for tissue hydroxyproline content.
Results:
There was a statistically significant difference between the control and pneumoperitoneum groups, regarding adhesion numbers and grades (P < 0.001). Cecal tissue hydroxypyroline content level was lower in group 1, and statistically significant differences were observed between groups 1, 2, and 3 regarding hydroxyproline content (P < 0.001). There was a statistically significant difference between the control and pneumoperitoneum groups regarding inflammation (P = 0.002).
Conclusions:
Pretreatment with the CO2 pneumoperitoneum had a prophylactic effect on postoperative adhesion formation in this study.
Introduction
We could not find any studies about the direct relationship between preventive administration of the carbon-dioxide (CO2) pneumoperitoneum and adhesion formation in the English literature. The relationship between laparoscopy and postoperative adhesions has been studied on the basis of the less-tissue-trauma effect of laproscopy, and it has been compared with conventional open surgery about effects on adhesion formation. However, we are interested in the relationship between the CO2 pneumoperitoneum itself and adhesion formation. CO2 is usually preferred as the insufflating agent for laparoscopic surgeries because it is readily available, noncombustible, and chemically stable. Therefore, it is the most widely used and accepted insufflation gas with demonstrated immunologic advantages for laparoscopy.5–9 In this study, we aimed to assess whether the preventive administration of the CO2 pneumoperitoneum had a positive effect on postoperative intraperitoneal adhesion formation in a rat cecal abrasion model.
Methods
Animals
The Animal Studies Committee at Ankara Teaching and Research Hospital approved animal care and all experiments. Thirty adult male Sprague-Dawley rats (250–350 g) were used for the study. The animal housing environment maintained a 12-hour light-dark cycle, a temperature of 22°C, and allowed access to standard laboratory food and water ad libitum.
Experimental protocol
All surgical procedures were performed by a single surgeon under aseptic conditions. Animals were initially anesthetized with 60 mg/kg of intramuscular ketamine hydrochloride (Ketalar®, Parke-Davis, Morris Plains, NJ). The pneumoperitoneum was achieved by introducing an 18-gauge angiocatheter placed percutaneously through the abdominal wall and insufflating the abdomen with 4 mm Hg gas. For adhesion induction, we used a modified rat model of abdominal adhesion formation originally described by Krause et al. 10 ; a midline abdominal incision, 4 cm in length, was made. The cecum was put on gauze and abraded with a sterile, dry 4 × 4 cm surgical gauze until a punctuate hemorrhage occurred on the surface of the cecum. Opposing areas of the abdominal wall and the parietal peritoneum were also abraded with a #11 scalpel. The cecum was then returned to its original location in the abdomen, and the abdominal wall and subcutaneous skin were closed uninterrupted, using Vicryl® sutures (Johnson & Johnson, Tokyo, Japan). Animals were sacrificed and a wide U-shaped incision was made under costal margins to investigate the extent and the type of adhesion formation 14 days later by an observer blinded to the identity of the experimental groups (Figs. 1 and 2). Each animal was evaluated by use of a modified scale devised by Evans et al. 11 According to this scale, 0 = no adhesions, 1 = smooth adhesions splitting spontaneously or with weak traction, 2 = firm adhesions splitting by traction, and 3 = dense adhesions requiring sharp dissection. Next, the cecum and the opposite parietal peritoneum and the adhesion areas were excised for both histopathology and biochemical examination for tissue-peritoneal hydroxyproline level measurement.
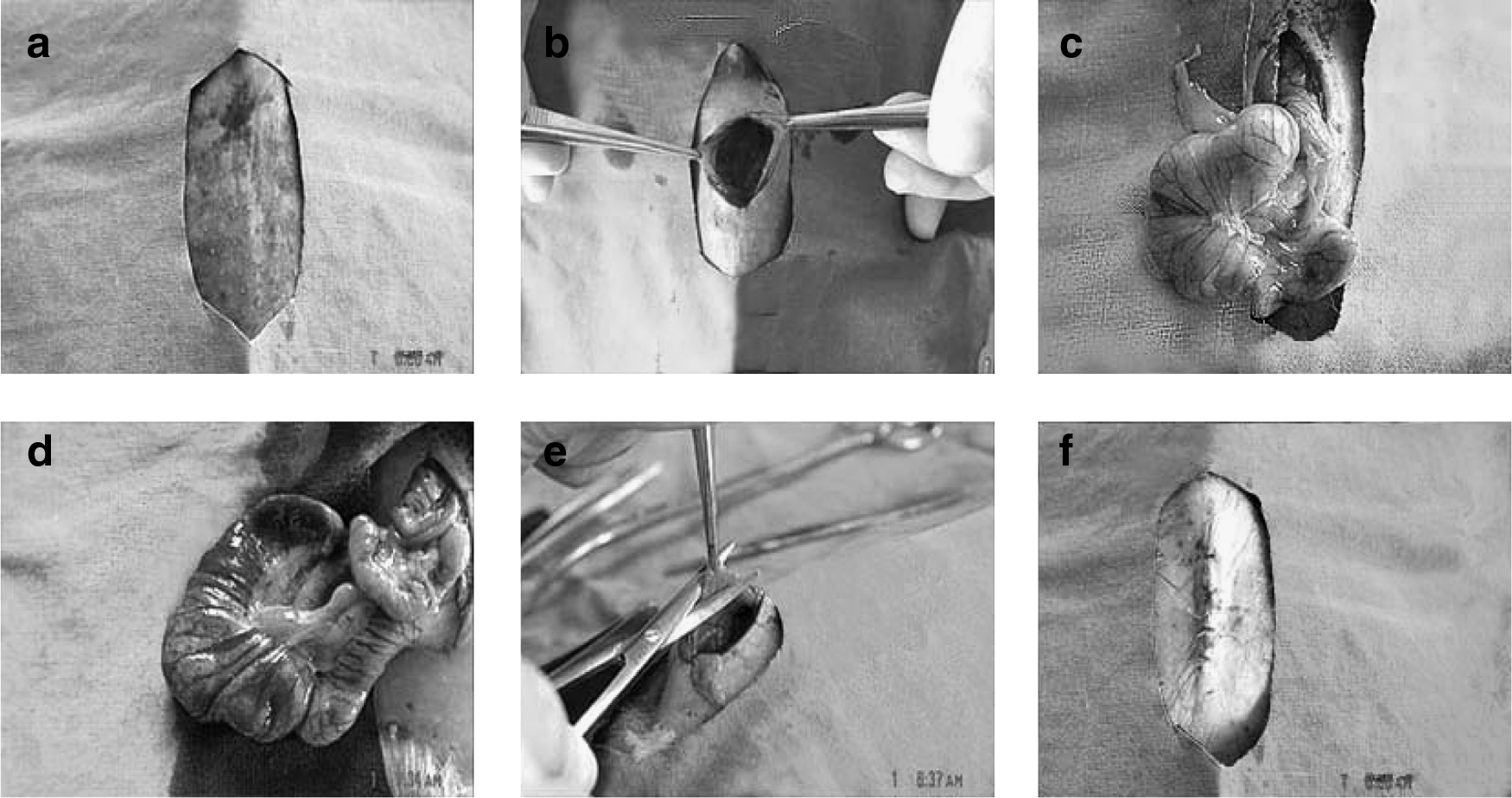
The adhesion model: (
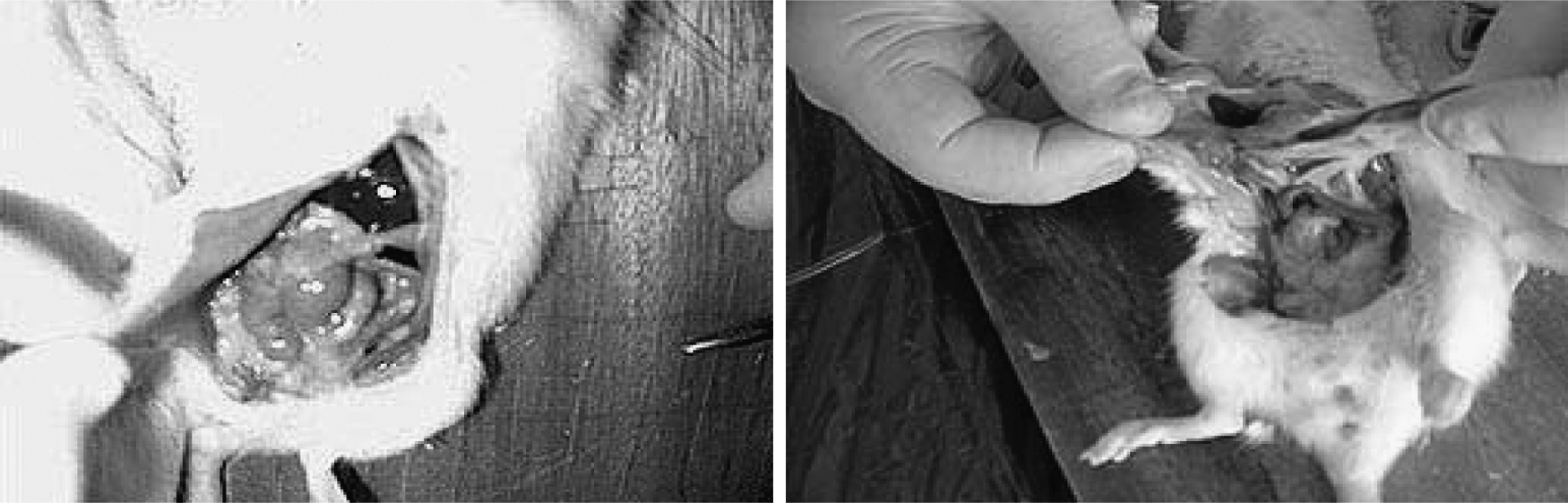
Evaluations of the adhesions after sacrification.
Thirty rats were divided into three different groups. In the first group (n = 10), laparotomies were performed and cecal and peritoneal abrasions were carried out and abdominal walls were closed. In the second group (n = 10), before laparotomy, the pneumoperitoneum was performed for 30 minutes, and after the pneumoperitoneum, laparotomies were performed and cecal and peritoneal abrasions were carried out as in group 1. In the third group (n = 10), before laparoromy, the pneumoperitoneum was applied for 2 hours, and after this, laparotomies were performed and cecal and peritoneal abrasions were carried out and abdominal walls were closed as in groups 1 and 2.
Tissue hydroxypyroline level measurement
Tissue samples were hydrolysed in 6 M of hydrochloric acid, at 105°C, for 18 hours and evaporated until they are dry. Hydroxypyroline levels were analyzed by colorimetric methods with Ehrlich's reagent (10 g p-dimethylaminobenzaldehyde, 11 mL perchloric acid). Hydroxypryoline contents were measured against standard concentrations and are expressed as micrograms per miligram of tissue. 12
Pathologic examination
Two samples, with a mean size of 1 × 1 × 0.4 cm from the cecum wall and parietal periton of each rat, were examined. The samples were fixed in a 10% formaldehyde solution. After dehydration, sections of 5-μm thickness from paraffine blocks were taken by a microtome. Under a light microscope, these sections were examined after hematoxylin and eosin staining. Inflamations were investigated by examination of the quantitative density of inflammatory cells and types, mesotel morphology, cellular responses, such as fibrosis, and neovascularitation. All of them were investigated by the same pathologist unaware of the study groups.
Statistical analysis
A sample size of 6 per group was required to detect at least a 2-unit difference between control and any case group in number of adezyon with a power of 80% at the 5% significance level. Sample-size estimation was calculated by using NSCC and PASS statistical package programs licensed by Jerry L. Hintze, PhD, 2001; NCSS and PASS, Number Cruncher Statistical Systems; Kaysville, UT). All analyses were performed by using an SPSS (v. 11.5) statistical software package (SPSS, Inc. Chicago, IL). Ordinal variables were described by median and range. Categoric variables were described by frequencies. Differences between the groups were analyzed by the Kruskal-Wallis or analysis of variance tests. When a statistical significance was present, Tukey's multiple test was used. A P-value less than 0.05 was considered significant.
Results
No mortality occurred in the study groups. The abdominal adhesions and adhesion scores are summarized in Table 1. There was a statistically significant difference between the control (group 1) and pneumoperitoneum groups (groups 2 and 3) regarding adhesion grades (P < 0.001). No statistically significant difference was observed between groups 2 and 3 (P = 0.759). Adhesion numbers were higher and statistically significant in group 1, as compared to groups 2 and 3 (P < 0.001). There was no statistically significant difference between groups 2 and 3.
μg·hydprol/mg = microgram hydroxyprolinen/milligram wet weight.
The difference between group 1 was statistically significant (P < 0.001).
The difference between group 1 was statistically significant (P < 0.01).
Kruskal-Wallis test.
One-way analysis of variance.
Mean ± standard deviation.
Median (min-max).
Hydroxyproline levels of the intra-abdominal wounds also are summarized in Table 1. There was a statistically significant difference between the control and pneumoperitoneum groups (groups 2 and 3) regarding hydroxyproline content (P < 0.001). While cecal tissue HP level was 0.16 ± 0.045 μg/mg tissue in group 1, this value was 0.27 ± 0.059 μg/mg tissue in group 2 and 0.34 ± 0.086 μg/mg tissue in group 3. There was no statistically significant difference between groups 2 and 3.
The results of the pathologic examinations of the study are summarized in Table 1. In the pathologic analysis, there was a statistically significant difference between the control and the pneumoperitoneum groups regarding inflammation (P = 0.002). There was no statistically significant difference between the pneumoperitoneum groups regarding inflammation. Grades, inflammation, and the hydroxyproline contents of the groups are seen in Figure 3.

Grades, inflammation, and hydroxyproline contents of the groups. Group (1 score was higher than the other groups (CO2 pneumoperitoneum). There was a statistically significant difference between the control group and the pneumoperitoneum groups regarding grades, inflammation, and hydroxyproline contents (P < 0.001, P = 0.002, and P < 0.001).
Discussion
In order to prevent adhesion formation, several agents and approaches have been used to date. Adhesions cause small intestine obstructions, chronic abdominal pain, and infertility and lead to serious morbidity and mortality by making the following surgery risky and difficult.13–16 Adhesion formation is a complicated process. Macrophages, fibroblasts, and mesothelial cells have a major role during the stages of adhesion formation. Tests and clinical studies showed that there is a dynamic balance between pro- and anti-inflamatory cytokines.17–19 Surgery is an important factor that causes the distortion of this balance. We know that intraperitoneal adhesion formation is promoted when two damaged surfaces come into contact. 20 Miyano et al. reported that CO2 insufflation would appear to alleviate the contact between damaged surfaces. 21 This is the mechanical effect of the pneumoperitoneum. Laparoscopy is associated with fewer entry and manipulation injuries; nevertheless, the pneumoperitoneum is also responsible from decrease in acute phase response. 22 As we emphasized before, there are many reports about the superiority of the laparoscopic procedures over conventional operations for reducing the incidence of postoperative adhesions. Mostly, we mentioned the technical specifications of laparoscopy to explain this condition, but very few comparative studies are available to prove this. Laparocopic surgery is associated with a lesser amount of blind dissection and lesser use of materials, such as retractor and compress, in the abdominal explorations. It is also associated with a reduced amount of washing and drying of the peritonei, thereby lesser contact of foreign materials and lesser tissue damage and bleeding at the surgical area, compared to conventional surgery.13,23 So, it is logical to state that laparoscopy causes fewer adhesions.
In contrast to these reports, Filmar et al. concluded that adhesions following laparotomy and laparoscopy were not different. Marana et al. and Jorgensen et al. found no differences between adhesions after laparotomy and laparoscopy. Yesildaglar et al. reported that the duration of the CO2 pneumoperitoneum was a cofactor in adhesion formation.24–27 Elkelani et al. reported that higher insufflation pressures and longer duration of the pneumoperitoneum were associated with increasing adhesion formation with pure CO2. They also found that adhesion formation was decreased with the addition of 3% oxygen to the CO2 pneumoperitoneum. 28 It is reported that the CO2 pneumoperitoneum enhanced adhesion formation and became known as a cofactor in postoperative adhesion formation. Peritoneal hypoxia was suggested as a mechanism, since the effect increased with the duration of the pneumoperitoneum and with insufflation pressure.29,30
The CO2 pneumoperitoneum is known to favorably modify the systemic immune response during laparoscopic surgery. It has been shown that CO2 insufflations cause local peritoneal acidosis without affecting systemic status. The CO2 pneumoperitoneum is considered to have beneficial immunomodulating effects and is a potent anti-inflammatory agent.6,31,32 It has been confirmed with experimental studies that the capnoperitoneum leads to a decrease in macrophage function and systemic inflammatory responses.32–36 Studies of West et al. demonstrated that when postinsufflation peritoneal pH was reduced to 6.1 by CO2, the intracellular pH of macrophages were also lowered. 37 It was shown that superoxide, as well as phagositosis and cytokine, production were suppressed by a decrease in intracellular pH.38–40 Following the laparoscopy, decreased proinflammatory cytokine production from peritoneal tissues can be responsible for lessening postoperative pain and adhesion formation.38,41
By using the simple adhesion model, we planned to measure the isolated effect of the pneumoperitoneum in adhesion formation in our study. We formed the groups by taking half-and 2-hour limits as the basis for the pneumoperitoneum. At the beginning of our study, we planned to measure whether the adherence effect of the pneumoperitoneum, if there was any, would change with the duration of the pneumoperitoneum. We revealed that, in pneumoperitoneum groups, adhesion formation and adhesion grades were lower, compared to the sham group, and the difference was statistically meaningful. At the same time, when the adhesion grades of two pneumoperitoneum groups were compared, there was no statistical difference between them. We think that it will be more practical, in clinical use, that the same effect should come about with the half-hour pneumoperitoneum.
In this study, histopathologic surveys reveal that cecal peritoneal inflammation scores were lower in pneumoperitoneum groups, compared to the laparotomy group. There was a statistically significant difference between the control group and the pneumoperitoneum groups regarding inflammation (P = 0.002). There was no statistically significant difference between the pneumoperitoneum groups regarding inflammation. Thus, we presume local peritoneal inflammation is dramatically reduced by the pneumoperitoneum and that postoperative adhesion formation decreases as a consequence.
Hydroxypyrolin (HP), which comes about by the degradation of collagen, develops by the hydroxylation of prolin amino acid and is a major component of collagen, keeping the stability of the three-part spiral structure of collagen through hydrogen bonds.42–45 In the Milligan et al. studies, since tissue hydroxypyrolin is a product of collagen breakdown, it was observed as especially higher in the neutrophil group. In this study, it is stated that, in especially neutrophil-dependent collagen-breakdown process, tissue HP levels may be an indicator. 45 A study by Altuntas et al. reveals that peritoneal HP levels are influential in the adhesion of seprafilm to polipropilen mesh. In that study, researchers claim that increase in HP level has the fundamental role in the adhesion-reducing effect of seprafilm. 44 In our study, cecal hydroxyprolin levels are found to be meaningfully high, statistically, among the pneumoperitoneum groups. Adhesion grades and tissue HP levels were statistically found to be different in the laparotomy group than in the pneumoperitoneum group (P < 0.001). In spite of documenting and defining the molecular source and pathophysiology of postoperative adhesion formation, the relation between the capnoperitoneum and adhesion formation and its mechanism is yet to be clarified. This study is the first experimental research to reveal that pretreatment with the CO2 pneumoperitoneum is effective in preventing postoperative adhesion formation.
Conclusions
Our results suggest that the CO2 pneumoperitoneum has positive effects on postoperative intraperitoneal adhesion development. As we know, intraperitoneal adhesion formation is promoted when two damaged surfaces come into contact. Therefore, CO2 insufflation would appear to alleviate the contact between damaged surfaces. Perhaps this is the mechanical effect of the pneumoperitoneum. However, in this study, we applied the CO2 pneumoperitoneum before the cecal abrasion. We cannot explain the pathophysiology by this mechanical effect. The pathophysiologic and molecular basis of postoperative adhesion formation has been well documented and described, but a correlation between the capnoperitoneum and postoperative adhesion formation and mechanisms of the prevention of adhesion formation by the capnoperitoneum is still unknown. We need more research on this subject to explore its mechanism.
Footnotes
Disclosure Statement
No competing financial interests exist.