
Abstract
Abstract
A 4-year-old male presented with abdominal pain. A computed tomography scan of the abdomen was negative, but a pleural effusion and mass was noted in the lower left thorax. Video-assisted thoracoscopic surgery revealed the mass to be a rare case of extralobar pulmonary sequestration that had undergone infarction.
Introduction
Case Report
A previously healthy 4-year-old male developed acute onset of abdominal pain without vomiting, diarrhea, or fever. Two days later, mild grunting respirations were noted. Examination by his primary care physician was remarkable for abdominal tenderness, and he was sent to a local emergency department. A computed tomography (CT) scan of the abdomen was normal, but a pleural effusion was noted in the left thorax. A chest radiograph showed a left-lower lobe opacity, and he was transferred to this institution for further evaluation.
Review of the abdominal CT showed a circumscribed, ovoid, soft-tissue density adjacent to the posterior left hemidiaphragm. Sonography of the left chest revealed an echogenic, well-circumscribed mass in the left medial posterior costophrenic angle. The mass did not appear to arise from the diaphragm and was closely associated with the posterior pleural margin. No color-flow vascularity could be demonstrated, and no feeding vessel either from the pulmonary or systemic circulation could be confirmed. At this stage, our differential diagnosis included infection-related inflammation or hemorrhage, infected or infarcted sequestration, neuroblastoma, or, less likely, a neoplasm involving the diaphragm (such as rhabdomyosarcoma) or pleura.
A limited CT with contrast was performed to confirm the presence or absence of calcifications, assess for incremental enhancement of the mass, and more definitively evaluate for a feeding vessel. This confirmed a teardrop-shaped mass of homogeneous attenuation in the lower posterior left thorax without extension into the neural foramina or below the diaphragm (Fig. 1). No feeding vessel was identified, and no adenopathy was noted.
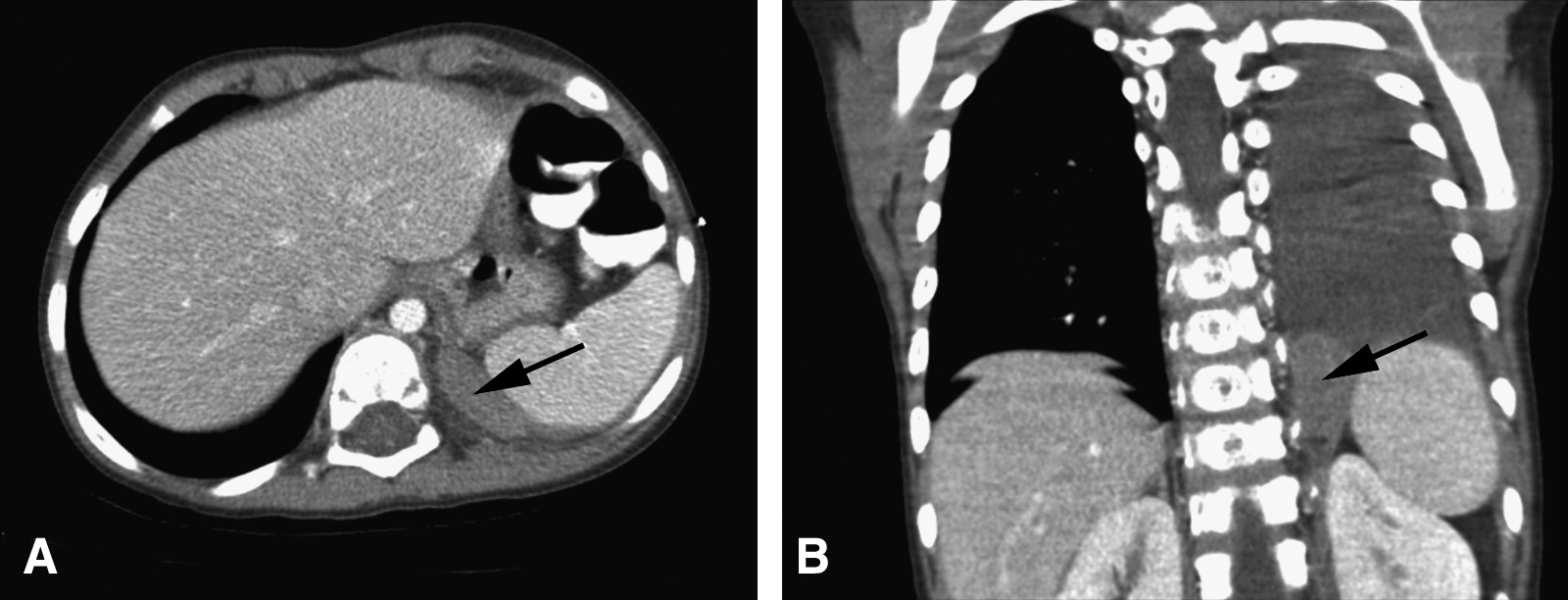
CTS of the abdomen. Axial (
The patient underwent video-assisted thoracoscopic surgery. Using one lung ventilation, the patient was placed in the right lateral position. With the surgeon standing to the front of the patient, three trocars were used to triangulate the mass, as demonstrated on the CT scan, (Fig. 2) with the mass medial and posterior in the chest. Low-pressure insufflation was used for lung retraction. The necrotic mass with accompanying bloody fluid was easily identified in the posterior medial sulcus at the diaphragm. With manipulation of the mass, the tethering blood vessel, which was visibly twisted, was seen arising from the sulcus, typical of a large feeding vessel for a sequestration passing through the diaphragm into the chest (Fig. 3). An endloop was used to encircle and ligate the stalk near the diaphragm, and the stalk was divided (Video 1). The entire mass was removed through one of the port sites without morcellation or enlargement of the site. The sites were closed with an absorbable suture after the lung was reexpanded under direct vision. The patient recovered without complication and was discharged from the hospital 3 days later.
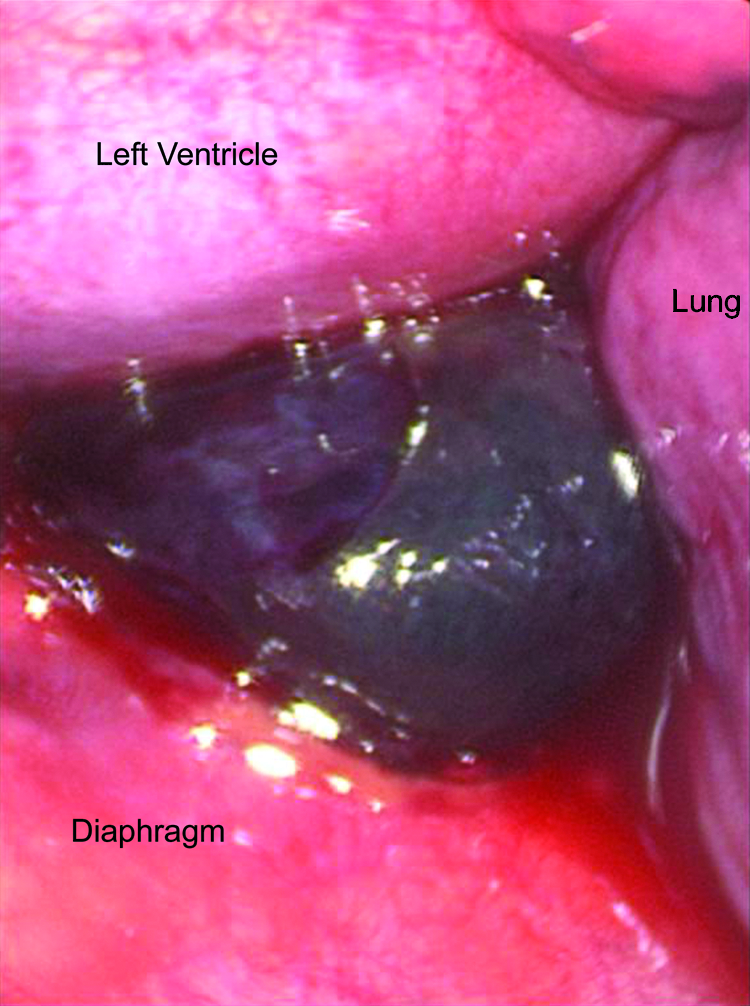
Initial thoracoscopic view of the necrotic extralobar sequestration adjacent to the diaphragm.
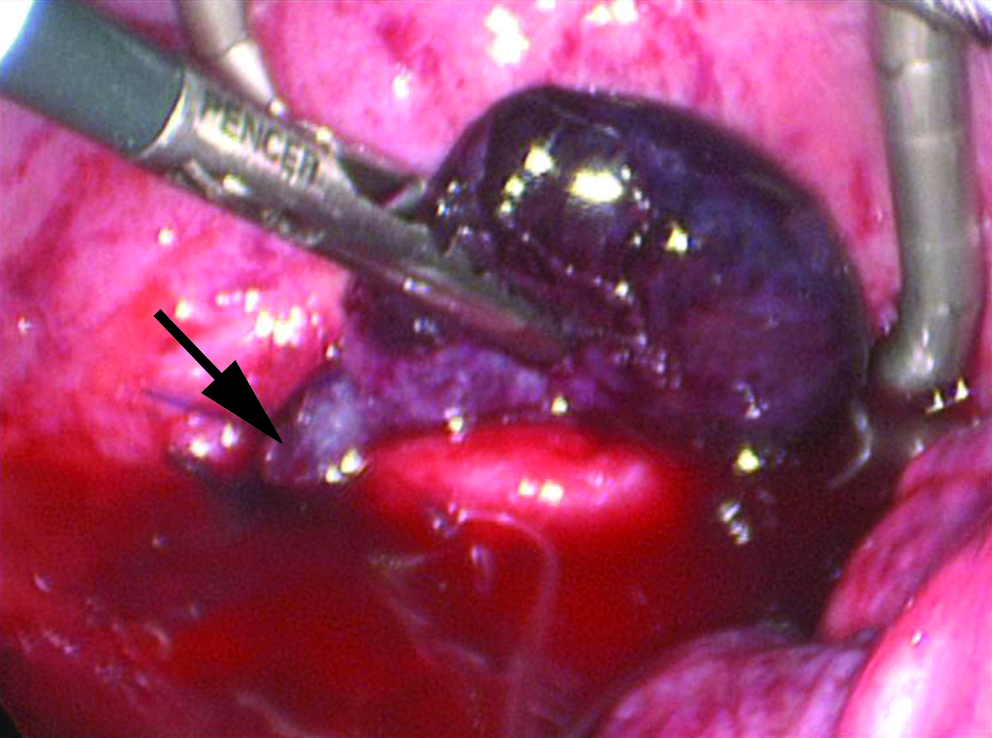
View of the base of the sequestration near the chest wall, with the feeding vessel (arrow) going through the diaphragm.
Pathology
The red-brown, firm, rubbery mass measured 3.4 × 2.7 × 0.9 cm. There was extensive acute hemorrhage and coagulative necrosis. Non-necrotic areas showed acute hemorrhage in fibroadipose tissue that contained several large arteries and veins. While no definitely identifiable bronchioles, alveoli, alveolar ducts, or cartilage were seen, the architecture of the necrotic tissue was consistent with lung (Fig. 4).
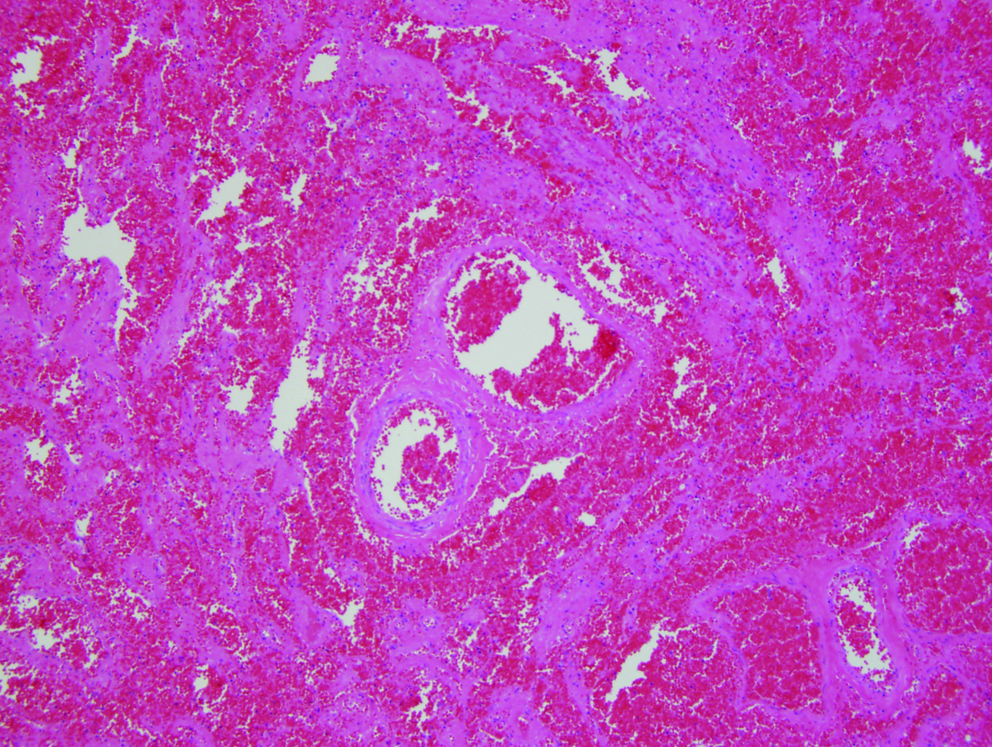
Lung architecture is discernable in the infarcted tissue. 10X; hematoxylin and eosin stain.
Discussion
Extralobar sequestration is a term used to describe a mass of pulmonary tissue anatomically separate from the normal lung1,4 and outside of the visceral pleura,1,5 but covered by its own pleural investment. 6 In 75% of the cases, blood supply to the sequestration is via a direct branch of the thoracic or abdominal aorta, with the remaining case receiving blood via smaller systemic arteries and the pulmonary artery. 7 The majority of patients with this entity present by 3 months of age, 1 often due to the presence of other congenital abnormalities, including congenital diaphragmatic hernia, cardiac, or gastrointestinal malformations. 8 About 90% of extralobar sequestrations occur in the left hemithorax.8,9 In older children and adults, these masses are often found incidentally in asymptomatic patients being evaluated for other causes. 3
A review of the literature demonstrates that infarction of an extralobar sequestration is extremely uncommon, with the current case being the youngest reported (Table 1). Chest and/or abdominal pain and a pleural effusion, often bloody, are common presenting features. While 1 case presented after blunt trauma, 10 most occur without an apparent triggering event. In previous cases, patients were initially diagnosed as having pneumonia with effusion2,6,10 or an unknown intrathoracic mass, often with effusion.3,11,12 All reported cases, including ours, underwent surgical excision for identification and treatment. While most extralobar sequestrations have a feeding systemic vessel, failure to identify such a vessel by imaging techniques does not rule out this entity in a patient presenting with an intrathoracic mass. In our case, the torsion resulted in cessation of blood flow within the mass, hence the inability to demonstrate the vessel by CT angiography or Doppler color-flow ultrasound.
Conclusions
In summary, we present an unusual case of a young boy with an infarcted extralobar sequestration. Diagnosis and curative excision was accomplished with video-assisted thoracoscopy. This rare entity should be included in the differential diagnosis of a child presenting with chest or abdominal pain, pleural effusion (especially if bloody), and an intrathoracic mass.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.