
Abstract
Abstract
With the advancement of laparoscopic equipment and growing operational experience, the number of case reports or descriptions of series of nephrectomies performed in patients with the preoperative diagnosis of venous system involvement has become more frequent in the medical literature. In this article, we present the case of a laparoscopic nephrectomy performed with retroperitoneoscopic access for preoperatively diagnosed renal vein and vena cava thrombus. Operation time was 130 minutes and blood loss was 50 mL. The weight of the specimen was 460 g. The postoperative course was uncomplicated. The pathology report revealed pT3b clear cell cancer (Fuhrman grade 2) with negative margins on the venous cutting line.
Introduction
Case Report
A 68-year-old male was admitted to our department due to a right kidney tumor diagnosed during an outpatient ultrasound examination. The patient's history included a single episode of hematuria. The general condition of the patient and laboratory findings proved to be normal; arterial hypertension was the only abnormality. An abdominal computed tomography scan revealed a pathologic mass measuring 6 cm in diameter within the right kidney and the presence of a thrombus that occupied the renal vein causing also its dilation (Fig. 1). The thrombus also involved the IVC. The presence of an accessory renal vein located below the main renal vein affected by the thrombus was also described. The patient was scheduled for a radical laparoscopic nephrectomy. Under general anesthesia, the retroperitoneal approach was created by using four trocars. After the preparation of the renal vascular pedicle, the accessory renal vein and renal artery were located, clipped, and cut. Such a maneuver allowed access to the renal vein containing the thrombus; the distal end of the thrombus balloted freely in the lumen of the IVC. The floating thrombus was carefully pushed into the renal vein, which was clamped below the thrombus, thus preventing the risk of cutting the vein altogether with the neoplastic tissue (Fig. 2). The vein was cut below the clamp by using the Endo-GIA™ stapler (Covidien Autosuture, Mansfield, MA). Macroscopically, the renal vein stumps were free from the malignant infiltration (Figs. 3 and 4). This observation was later confirmed by the histopathology report. What followed was a standard radical nephrectomy, performed according to the technique applied in our institution, 10 and the specimen was removed intact in the laparoscopic retrieval sac through the oblique hypogastric skin incision on the operated side. The mass of the specimen was 460 g. The surgery time was 130 minutes and estimated blood loss was 50 mL. The postoperative course was uneventful, and the patient was discharged home on the postoperative day. Histopathology revealed pT3b clear cell carcinoma (Fuhrman grade 2).

Computed tomography scan reveals the thrombus in the right renal vein and inferior vena cava.

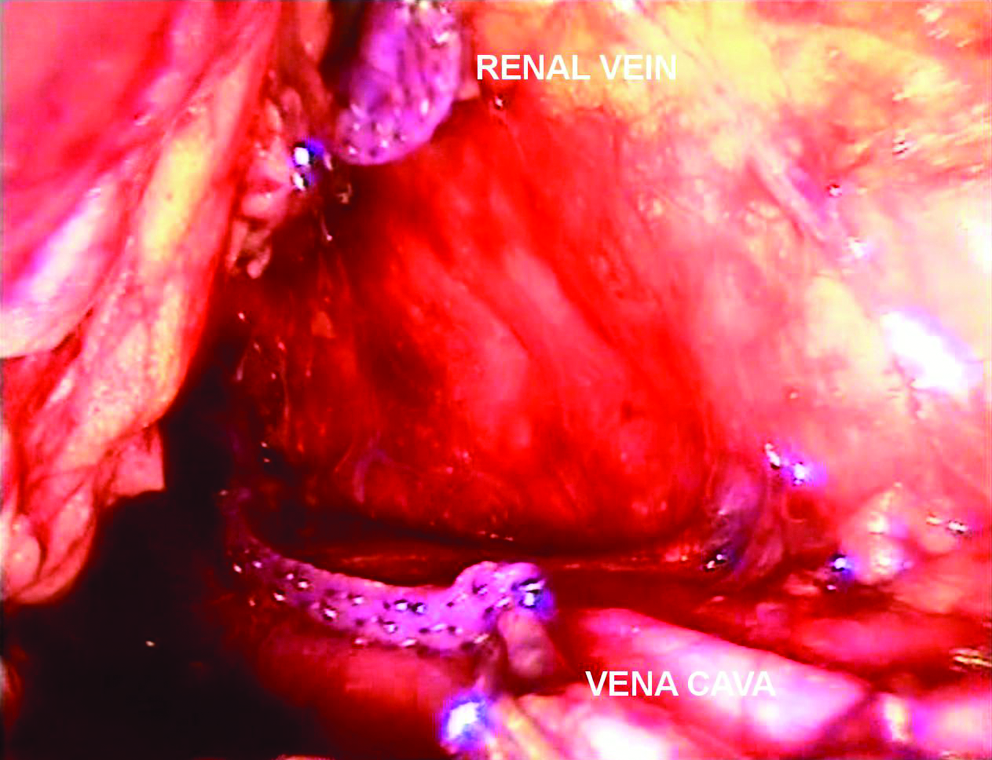
Renal vein clamped below the thrombus.
Stumps of renal vein and inferior vena cava macroscopically free of tumor.

The specimen after nephrectomy. The thrombus is visible in the lumen of the open renal vein.
Discussion
Laparoscopic nephrectomy is currently acknowledged as a standard treatment in grade T1–T3a renal cancer.7,11 At present, in many centers, the indications for laparoscopy include also cases with preoperatively diagnosed venous system involvement. The only accepted contraindication is significant limphadenopathy with infiltration of the IVC walls and organs adjacent to the kidney. 5 In cases with tumor thrombus, the preoperative evaluation of the level of penetration into the vena cava and a possibility of malignant infiltration of its walls are of paramount significance. The end of the thrombus freely balloting in the lumen of the IVC may be laparoscopically pushed into the renal vein in order to avoid cavotomy similarly as in an open surgery. The majority of researchers use the branches of the stapler for that purpose.5–7 In the case discussed above, an additional tool was used in order to displace the thrombus maximally toward the kidney to provide an oncologic margin within the stump of the renal vein. However, in cases with a huge volume of the thrombus, that maneuver may prove to be difficult or impossible to perform. Moreover, significant renal hilar limphadenopathy may also prevent the use of that technique; in such cases, the hand-assisted laparoscopy can be applied, or the conversion to open surgery is recommended. 8 Laparoscopy provides excellent visualization of renal vessels. In the described case, the tumor thrombus within the renal vein and its lower end within the IVC were distinctly visible, thus allowing a safe displacement of the thrombus into the renal vein under visual control. The use of the intraoperative Doppler ultrasound enables a precise localization of the thrombus.5–8 Such parameters as operative time, blood loss, and risk of major complications do not differ significantly in T3b patients, when compared to a large series of nephrectomy cases.5–7 The applied approach (i.e., transperitoneal or peritoneal) results from the surgeon's preferences, rather than the superiority of any of the techniques. In our opinion, despite the smaller working space, the retroperitoneal approach applied in our institution allows an early identification of vascular pedicle and closure of the renal artery. That technique allows to decrease the pressure in the renal venous system and to manipulate the thrombus in order to displace it. 6
Breaking the consecutive technical barrier in the laparoscopic treatment of renal malignancy is, beyond doubt, a milestone in the prognosis of the development of that procedure. Emerging reports on the pure laparoscopic removal of the thrombus from the IVC 12 and experimental animal surgery performed by a pioneering team from Cleveland may serve as promising proof. After the creation of cardiopulmonary bypass, 6 hypothermic calves underwent a successful nephrectomy en bloc with IVC thrombus. An angioscope was inserted inside the IVC to visually confirm complete thrombus clearance; then, the vena cava was suture repaired. Simultaneously, the second team performed a thoracoscopy with an incision and exploration of the right atrium, venoscopy, and right atrium suture repair. 13 The clinical application of these experimental results is only a matter of time.
Conclusions
Recent experience in laparoscopic nephrectomy in patients with grade T3b renal cancer has been promising. In conclusion, laparoscopic radical nephrectomy for stage T3b is feasible with adherence to mandatory oncologic principles in selected patients; however, long-term follow-up is needed in order to evaluate oncologic outcomes of that technique.