
Abstract
Abstract
Pneumoscrotum is a rare condition defined by the presence of gas within the scrotum. Most cases are associated with the pneumoperitoneum; the condition has been described after various diagnostic and therapeutic procedures and disease conditions. In this article, we report a case of a patient admitted to the emergency department for right-upper quadrant abdominal pain. Abdominal X-ray showed free air in the right subdiaphragm; computed tomography (CT) confirmed free air in the abdomen and detected free fluid in the pelvis. The patient underwent laparoscopy, at which time a 1-cm perforation on the anterior wall of the gastric antrum near the pylorus was identified. The perforation was sutured with three detached stitches of reabsorbable material. Approximately 2 days after the surgical procedure, physical examination of the patient showed significant scrotal swelling suspicious for the presence of subcutaneous air. A CT scan confirmed the presence of the pneumoscrotum. The patient returned to the operating room and underwent an exploratory laparotomy. A new perforation was identified beneath the previous one and was sutured with two detached stitches. The patient was discharged uneventfully after 8 days of hospitalization. Pneumoscrotum should be recognized as an early sign of recurrence in patients operated on laparoscopically for peptic ulcer.
Introduction
Case Report
A 17-year-old man was admitted to the emergency department for right-upper quadrant abdominal pain, which began 3 hours prior to admission. On physical examination, the patient showed right-upper quadrant tenderness. Percussion of the liver showed resonance, which was suspicious for free intra-abdominal gas. Abdominal auscultation showed rare abdominal movements. The patient had no fever and no signs of sepsis. Laboratory findings showed leukocytosis (19 × 109/L). Laboratory tests for hepatic and pancreatic function, electrolytes, renal function, and coagulation were normal. Abdominal X-ray showed free air in the right subdiaphragm. Computed tomography (CT) showed free air in the right subdiaphragm with free fluid in the pelvis.
The patient underwent a laparoscopic exploration. Prophylactic antibiotics and PPIs were administered at the initiation of surgery. Under general anesthesia, a 10-mm trocar was introduced trough the infraumbilical area via an open technique. Carbon dioxide was then insufflated through this trocar to create a pneumoperitoneum with a pressure of 12 mm Hg. Two 5-mm trocars were introduced into the right- and left-upper quadrants of the abdomen, respectively. After placement of these trocars, an adequate position was obtained by tilting the operation table to a 20-degree reverse position (i.e., the Trendelenburg position). A 1-cm perforation was identified on the anterior wall of the antrum, near the pylorus. The perforation was sutured with three detached stitches of reabsorbable material. The peritoneal cavity was irrigated with warm saline, using a pressurized suction-irrigation system, while special attention was paid to the right subphrenic, subhepatic, and pelvic regions. Air was inflated through a nasogastric tube (NGT) while the surgeon inspected the stomach, previously submerged in saline solution, to detect gastric leakage. No air bubbles could be detected. One suction drain was left around the perforation site at the end of the operation.
Twenty-four hours after the operation, the NGT was removed. During this period, the scrotum of the patient was clinically normal and no other symptoms were reported. Approximately 2 days after the surgical procedure, physical examination of the patient showed significant swelling of the scrotum, suspicious for the presence of s.c. air (Fig. 1). The testis was palpable. Laboratory data showed a white blood cell count of 20 × 109/L. ACT scan confirmed the presence of s.c. emphysema with the pneumoperitoneum and pneumoscrotum (Fig. 2). The patient was returned to the operating room for an open surgical exploration. On examination of the stomach and duodenum, a new perforation was identified beneath the previous one, localized on the anterior wall of the antrum and whose diameter was less than 1 cm. This new perforation was sutured with two detached stitches, using the Graham technique. The NGT was kept for 3 days after the procedure. Oral intake was started on hospital day 5. The patient was discharged uneventfully on hospital day 8.

Patient with a pneumoscrotum.
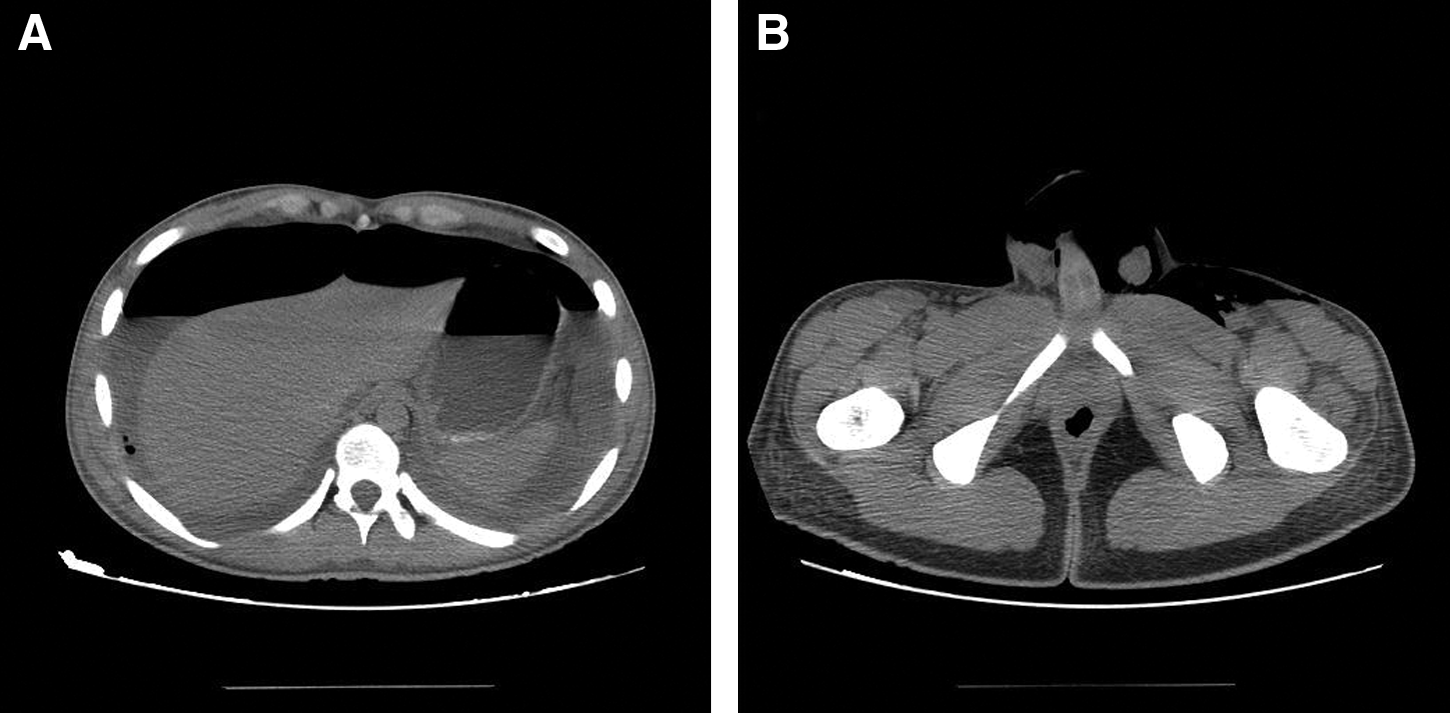
Computed tomography scan showing the pneumoperitoneum and free fluid collection in abdominal cavity (
Discussion
Until 2002, five therapeutic decisions regarding the management of perforated duodenal ulcer patients were recognized: 1) whether an operation is needed, 2) whether an omentopexy or definitive repair is necessary, 3) whether the patient is stable enough to undergo definitive repair, 4) which definitive repair is indicated, and 5) whether the availability of newer antacid agents should influence the choice of operation. 6 In 2002, a sixth decision was suggested: whether the procedure could be performed laparoscopically or by laparotomy. 7 Lunevicius and Morkevicius published a review comparing the outcome after laparoscopic and open repair for perforated peptic ulcer in 2005. This work was not limited solely to randomized trials, but also included both prospective and retrospective trials comparing laparoscopic and open repair. 8 Reoperation rates, reported in seven trials with a total of 490 patients, were 5.3 and 2.1% in the laparoscopic and open repair groups, respectively. 8 Subsequent meta-analysis showed a higher reoperation rate after laparoscopic repair, but the difference was not significant (P = 0.10). 8 The initial surgical approach in our patient was laparoscopic and in agreement with current guidelines requiring the absence of the following: other ulcer complications, such as bleeding and obstruction; large perforation; technical difficulty; previous upper abdominal operations, and serious associated cardiopulmonary disease. 9 Two days after the procedure, reoperation was performed via laparotomy due to previous laparoscopy complications. 10
Pneumoscrotum is an uncommon medical condition. There are three primary reasons for finding air in the scrotum. 5 First, s.c. or retroperitoneal air can dissect from the lungs along Camper's or Scarpa's fascias. 11 Second, local gas production or air introduction can produce air in the scrotum. 5 Third, an embryologic variant can result in air in the scrotum.5,11 The causes reported in the literature for the presence of air in the scrotum are reported in Table 1. The finding of air in the scrotal sac may be an early sign of a life-threatening condition or may represent an incidental finding associated with more common benign conditions. 11 The significance of scrotal air is related to the source of air production (i.e., local or peritoneal). Local air production suggests gas gangrene or scrotal trauma, which is infectious and may be fatal, unless treated appropriately. On the other hand, movement of air from the peritoneal space is usually noninfectious and can be treated conservatively. 12
Air can leave the intraperitoneal space and enter the scrotum via a patent processus vaginalis, which is present in approximately 15% of adults and 60% of infants.5,11 Pneumoscrotum may be a complication of laparoscopic access and is reported in the literature with a low incidence. 8 Two newborn babies who presented with scrotal pneumatoceles as a first sign of pneumoperitoneum due to gastric perforations are reported in the literature,13,14 but no case of pneumoscrotum due to gastric perforations in an adult has been recorded, to date. Obviously, at the first procedure, no air was present in the scrotum. Ultrasound can be used as a diagnostic technique for many diseases associated with pneumoscrotum, but we prefer to use the CT scan due to better availability in an emergency context. Treatment of pneumoscrotum is directed at the underlying disease. The condition itself is benign, and, owing to the elastic properties of the scrotal skin, there is no risk of urethral compression or vascular compromise. 11
Conclusions
This case report suggests the importance of clinical examination. Pneumoscrotum should always be considered as a precocious sign of recurrence in patients operated on laparoscopically for peptic ulcer.
Footnotes
Disclosure Statement
No competing financial interests exist.