
Abstract
Abstract
Laparoscopic cholecystectomy in patients with situs inversus can be a technically challenging procedure. Although laparoscopic cholecystectomy has been described in patients with situs inversus, no standard technique has been described. We are presenting our experience of laparoscopic cholecystectomy in two patients with situs inversus and discuss the problems encountered during surgery and likely remedies.
Introduction
Case 1
A 55-year-old female presented with epigastric pain, which was radiating to the back and was associated with nonbilious vomiting. On examination, she was dehydrated and tachycardia was present. The apex beat of the heart was on the right side. There was epigastric tenderness on abdominal examination. A chest radiograph revealed dextrocardia. Abdominal ultrasound revealed gallstones with features suggestive of acute pancreatitis and total reversal of the position of all viscera. Magnetic resonance imaging showed a left-sided liver and gallbladder with cholelithiasis and spleen on the right side. Biliary and vascular anatomy was normal, except for the reversal of sidedness (Fig. 1). She was diagnosed as a case of gallstone-induced pancreatitis with situs inversus viscerum. She was managed conservatively and discharged after 1 week and planned for elective cholecystectomy after 6 weeks. Laparoscopic cholecystectomy was planned, keeping in mind the mirror-image anatomy. All theater equipment was placed in a mirror-image position: the monitor on the left side and the surgeon and camera person on the right side of the patient (Fig. 2). The pneumoperitoneum was created by using a Veress needle. Four ports were used: a 10-mm umbilical port, a 10-mm subxiphoid port in the midline coming to the left of the falciform, a 5-mm subcostal left midclavicular port, and a 5-mm subcostal left anterior axillary port. There was a total reversal of the position of all the organs. The ileocaecal junction and appendix were in the left iliac fossa. There were mild adhesions at the fundus of the gallbladder (Fig. 3). The fundus was retracted by using the left anterior axillary port by the assistant. The Hartmann's pouch of the gallbladder was retracted by using the epigastric port, and the left midclavicular port was the main working port. Dissection of the Calot's triangle was done by the posterior approach, using the right hand through the left midclavicular port. The cystic duct–common bile duct junction was identified. The cystic duct and artery were clipped and divided. The gallbladder was dissected from the liver bed. The gallbladder was extracted through the epigastric port. Hemostasis was achieved and a drain was inserted. Total operative time was 70 minutes. She had an uneventful recovery and was discharged on postoperative day 1 after drain removal.
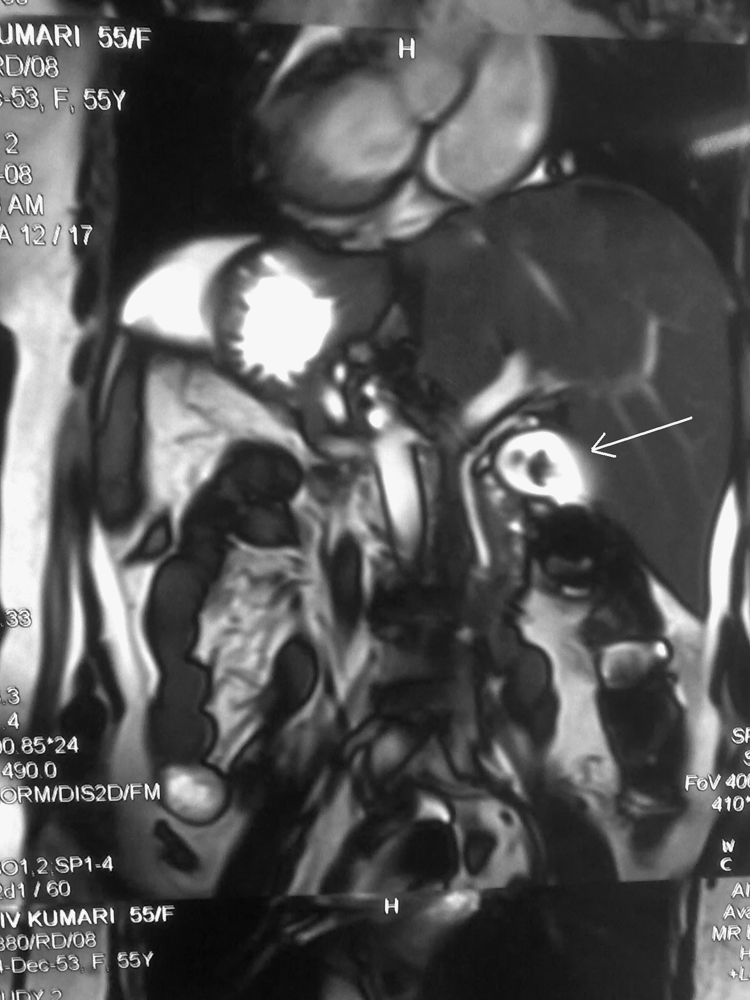
Magnetic resonance imaging showing the mirror-image anatomy.

Operation theater set-up and position of trocar placement.

Intraoperative left-sided gallbladder.
Case 2
A 26-year-old female presented with complaints of epigastric pain with nausea and vomiting for 2 days. There was no radiation of pain. On examination, the patient was dehydrated, febrile, and had local tenderness over the epigastrium. Her heart sounds were audible on the right side, her pulse rate was 90 beats per minute, and blood pressure was normal. An ultrasound scan of the abdomen showed a distended, acutely inflamed gallbladder containing multiple stones and was located on the left hypochondrium. The common bile duct was normal in caliber and free of stones. A chest skiagram showed the heart on the right side. Her total count was 12,000 cells/mm, and liver and kidney function was normal. An electrocardiogram showed a rights axis deviation. She was planned for laparoscopic cholecystectomy in the acute stage. The surgery was planned and carried out in a similar fashion to that mentioned above. The procedure was completed safely, and the patient was discharged on postoperative day 3.
Discussion
Fabricus reported first case of situs inversus in humans in 1600, and the incidence is currently in the range of 1:5000 to 1:20,000. It may be associated with other anatomic variations, such as heart malformation, Kartagener's syndrome, liver-lobe hypoplasia, biliary atresia, and vascular anomalies. However, there is no current evidence to suggest that situs inversus predisposes to cholelithiasis. 1 In the reported English literature, there have been only approximately 40 reports of open cholecystectomy and less than 20 cases of laparoscopic cholecystectomy in patients with situs inversus. Because of the rarity of the condition, the standard procedure and modifications for laparoscopic cholecystectomy in patients with situs inversus have not been described. The surgeon may get to operate on such patients only once in his or her lifetime and will not get a second case to improve on technique.
Although laparoscopic cholecystectomy has been described in patients with situs inversus, even in patients with acute cholecystitis or dense adhesions, the procedure nonetheless poses certain technical challenges for the whole operating team. The orientation and ergonomic challenges will usually result in an increased operative time. Operation time ranging from 15 to 75 minutes has been reported in the literature. Preoperative imaging can help in identifying vascular and biliary anatomy and anomalies. 2 The surgeon has to be meticulous in his or her dissection and keep on reminding him- or herself about the mirror-image anatomy at every step to prevent complications.
There are various technical and ergonomic difficulties faced, especially in right-handed surgeons performing laparoscopic cholecystectomy in these patients. The majority of reports describe that right-handed surgeons cross instruments within the peritoneal cavity to dissect with the right hand. 2 There is one interesting report of a comparison between a left-handed and a right-handed surgeon, where the left-handed surgeon did not face any problem in dissection because of better dexterity between two hands, as both his hands had adapted to work efficiently in surgeries and situations designed for right-handed surgeons. 3 There are few reports suggesting that the retraction of Hartman's pouch by the assistant from the midclavicular port may help the surgeon to perform surgery by using his or her right hand through the epigastric port.4,5 The major difficulties we faced were crossing of the hands and problems in applying liga clips, as we only have a 10-mm clip applicator, and the 10-mm port was in the epigastric region, from where it was very difficult to apply the clips.
Conclusions
We suggest the following modifications for surgeons who might encounter such a case in future: 1) use of a 30-degree telescope; 2) retraction of Hartmann's pouch through the midclavicular port by an assistant who should be experienced in laparoscopy; 3) use of a 10-mm midclavicular port instead of at the epigastric port, so that liga clips can be applied properly; the French position may not be very helpful, because the surgeon's dexterity will remain the same; 5) experienced laparoscopic surgeons should perform the surgery; and 6) if a left-handed surgeon is available, then the technical challenges will be less.
Footnotes
Disclosure Statement
No competing financial interests exist.