
Abstract
Abstract
Introduction:
Laparoscopic subtotal adrenalectomy (LSA) has emerged as a treatment option in the management of certain adrenal pathologies. After LSA, a satisfactory blood supply to the adrenal remnant is vital to preserve steroid function. The aim of this study was to review the adrenal blood supply with relevance to LSA.
Materials and Methods:
The adrenal blood supply was examined in three ways: 1) a review of six previous cadaver studies looking at adrenal blood supply; 2) a review of our 164 consecutive laparoscopic adrenalectomies (LAs) (January 1999–January 2009); the details of the main adrenal veins and variants had been prospectively recorded; and 3) dissection of 4 cadaver specimens (macroscopic and histologic examination was performed).
Results:
The six cadaver studies showed duplication or triplication of the main adrenal vein with variable frequency. Four of six studies described smaller peripheral veins surrounding the adrenal gland. The arterial supply appeared constant, with each adrenal gland supplied by up to 60 small arteries. In our series of LA, the main adrenal vein was constant. In 6 cases, the main vein was duplicated. Our cadaver dissection showed the large number of small peripheral veins and arteries surrounding the adrenal gland. Histology confirmed that these peripheral veins drained the adrenal gland.
Conclusions:
After LSA, a nonfunctioning adrenal remnant is unlikely due to an inadequate arterial supply. Division of the main adrenal vein appears safe, but excessive mobilization of the adrenal remnant should be avoided to prevent destruction of the peripheral veins.
Introduction
After subtotal adrenalectomy, a satisfactory blood supply to the adrenal remnant is vital to preserve function. It is not clear, from the literature, whether a preserved main adrenal vein is essential for remnant function. Nor is it clear, at time of surgery, that excessive mobilization would destroy the arteries surrounding the adrenal gland and lead to an ischaemic, nonfunctioning adrenal remnant. The aim of the current study was to review the importance of the adrenal gland blood supply when performing a laparoscopic subtotal adrenalectomy (LSA).
Materials and Methods
The blood supply of the adrenal gland was examined in three ways. An overview of the adrenal blood supply was studied in cadaver dissections. This involved a computer-assisted search of the Medline database. The combinations and terms included adrenal-suprarenal blood supply, adrenal-suprarenal arteries, adrenal-suprarenal veins, and adrenal vein variants. A review of our own consecutive laparoscopic adrenalectomy series was performed (January 1999–January 2009). The details of the main adrenal veins and variants had been recorded in each operation note.
Cadaver dissection of adrenal glands was performed. The arterial and venous supply was examined. The adrenal arteries were initially injected with a latex–India ink mixture via the carotid artery. The adrenal gland and its surrounding tissue were cleared by using the Spaltehoz technique (a 14-day technique involving alcohol and then methyl salicylate in the final step). Photography was performed by using a WolfVision LB9 visualizer (Klaus, Austria). The venous supply was examined by using standard dissection and then histologic techniques. A modified Masson's trichrome stain was used for microscopy.
Results
Literature overview
The main venous drainage described in cadaver studies has given differing results (Table 1).4–9 On the left side, the adrenal gland appeared to be drained by a single main vein in the majority of the studies. Only Clarke, in his study of 16 noninjected cadavers, found duplication of the main left adrenal vein in 5 cases. 6 On the right side, much more variation of the main adrenal vein was found. The main variants were duplication or triplication of the main adrenal vein. Johnstone, 5 Mikaelsson, 7 El-Sherief, 8 and Monkhouse and Khaligue 9 described the presence of smaller veins surrounding the adrenal gland (particularly on the lateral aspect). The nomenclature of these smaller veins varied: peripheral, capsular, or superficial. Using venous contrast, Mikaelsson 7 described how these peripheral veins originated from the adrenal gland, rather than the surrounding capsule or perirenal fat. Arterial blood supply was found to be remarkably consistent between the cadaver studies. The arteries supplying the adrenal gland took their origin from the following sources: inferior phrenic artery, aorta, and renal artery. All researchers described multiple small arteries surrounding and entering the gland. Anson et al. 4 described 50–60 small arteries supplying the adrenal gland.
Twelve right adrenal glands not suitable for dissection.
Adrenal vein variants visualized at time of laparoscopic adrenalectomy
Over the 10-year period, 144 patients underwent 164 laparoscopic adrenalectomies (LAs) (17 bilateral procedures, 3 patients delayed contralateral procedure). The main adrenal vein was identified in all cases at time of laparoscopy. In all cases, the right adrenal vein emerged from the anterior-inferior aspect of the gland and drained into the inferior vena cava (IVC). The left adrenal vein emerged from the inferomedial aspect of the gland and drained into the left renal vein. In 6 patients, the main adrenal vein was duplicated. Details of these variants are shown in Table 2. For 1 patient with a left-sided phaeochromocytoma, the drainage site of the second adrenal vein was unclear.
ACC, adrenocortical carcinoma; phaeo, phaeochromocytoma; IVC, inferior vena cava.
At time of laparoscopy, apart from the main adrenal vein, a large number of smaller vessels surrounded the adrenal gland. It was not possible to differentiate between veins and arteries. These vessels were all dealt with in a similar manner by diathermy or ultrasonic dissection. Blunt dissection was not performed, so as to avoid any unnecessary bleeding. For 4 patients with large (≥6 cm) phaeochromocytomas (n = 3) and an adrenal metastatic deposit secondary to renal-cell carcinoma (n = 1), there were increased numbers of periadrenal vessels. These were all divided without incident by careful ultrasonic dissection.
Cadaver dissection
Arterial supply
Four adrenal glands with intra-arterial latex were cleared of periadrenal fat by using techniques described in the Materials and Methods section. There were 2 left- and 2 right-sided glands. The arteries originated from the inferior phrenic artery, the aorta, and the renal artery. Division occurred in the fat surrounding the adrenal gland. The large number of small arteries surrounding and entering the glands are demonstrated in Figure 1.

The images show multiple arteries supplying the cleared adrenal glands. (
Venous drainage
The venous drainage was studied in 4 adrenal glands (2 left and 2 right). Using standard dissection techniques, the main venous drainage was via a single vein: the right one to join the IVC and the left one to join the left renal vein. However, a large number of smaller peripheral veins follow the numerous arteries surrounding the adrenal gland. These vessels, leaving the lateral aspect of a left adrenal gland, are demonstrated in Figure 2.

Gross dissection of the lateral surface of the left adrenal gland.
These lateral-placed veins were studied on histologic slides to ensure they were actually draining the gland, rather than running along the surface. Microscopic examination was performed in 2 cases (1 left and 1 right). This confirmed the veins drained the lateral aspect of the gland. Figure 3 demonstrates a peripheral situated vein progressively leaving the gland on repeated sectioning.
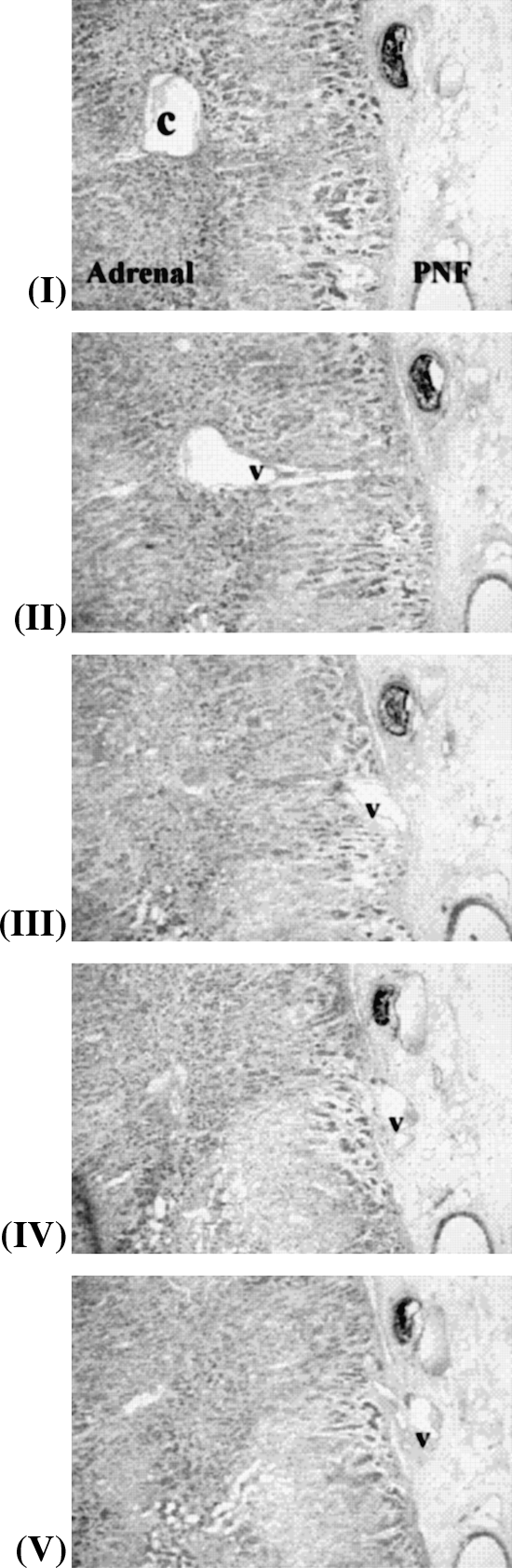
Five histological sections (I–V), showing a central vein (c) in the adrenal medulla drained by a superficial vein (v) penetrating the capsule into the perinephric fat (PNF).
Discussion
LSA is becoming an attractive option in certain patients with adrenal pathologies (e.g., familial phaeochromocytomas, aldosterone-producing adenomas, and cortisol-producing adenomas). This can eliminate the need for hormone substitution in the majority of patients. Adequate arterial supply and venous return is essential to allow a resulting functioning adrenal remnant for patients undergoing subtotal adrenalectomy. This study has shown, from our own and previous cadaver dissection, multiple small arteries completely surrounding the adrenal gland. The main adrenal vein was remarkably constant. However, when variation does occur, this was usually duplicated or triplicated. In addition to the main adrenal vein, cadaver studies have shown a network of peripheral veins surrounding the adrenal gland. These veins were closely related to the arteries.
From the small series describing subtotal adrenalectomy, it was not clear whether preservation of the main adrenal vein was essential to allow subsequent adrenal remnant function. Imai et al. described LSA in 5 patients (aldosterone-producing adenoma or weak-functioning adrenocortical adenoma) with preservation of the main adrenal vein. 10 The researchers hypothesized preservation of the main vein was essential to avoid venous congestion, which would lead to a nonfunctioning remnant. The resultant function of the adrenal remnant was not reported. Roukounakis et al. reported the importance of adrenal vein preservation for 7 patients undergoing subtotal adrenalectomy for aldosterone-producing adenomas or myelolipomas. Again, details of postoperative adrenal function was not reported. 11 Janetschek et al. described subtotal adrenalectomy in 6 patients with inherited phaeochromocytoma. 12 In a mean follow-up of 18 months, there were no recurrences. The researchers felt preservation of the main vein was essential to allow for a functioning adrenal remnant.
Ikeda et al. felt the adrenal vein could be divided without consequence to the adrenal remnant. 13 They described subtotal adrenalectomy with main vein division for 6 patients (aldosterone-producing adenoma, inherited phaeochromocytoma). Postoperative adrenal function was assessed by I-adosterol scintigrams. However, scintigraphy is not a suitable test to determine sufficient endocrine function. Brauckhoff et al. advocated a selective approach for division of the main adrenal vein, depending on the site of the adrenal tumor. 14 Of the 14 patients, 4 patients underwent bilateral subtotal adrenalectomy with division of the main adrenal vein. No patient required substitution with exogenous steroids. Postoperative adrenal function was assessed by serum levels of cortisol and adrenocorticotropic hormone (ACTH) within the normal range. Walz et al. demonstrated similar findings. 15 Subtotal adrenalectomy was performed in 2 patients with bilateral hereditary phaeochromocytoma. Postoperative cortisol levels were within the normal range.
Our study has shown the consistency of the main adrenal vein. In 158 of 164 laparoscopic arenalectomies, the main adrenal vein was single and originated from the same site. Duplication of the main adrenal vein occurred in 6 cases. A number of peripheral vessels always surrounded the gland. It was not clear at laparoscopy if these represented arteries or veins. An overview of cadaver studies, assessing the venous drainage of the adrenal gland, consistently demonstrated smaller veins surrounding the adrenal gland. Mikaelsson examined adrenal venous drainage in 22 fresh cadaver specimens. 7 The cadavers had been injected with contrast into the vena cava. Using a combination of dissection and radiologic examination, the researcher demonstrated that these peripheral veins drained the adrenal gland. In addition, from using gross dissection and histologic methods, we demonstrated that it was possible to follow the venous drainage from the adrenal gland to these peripheral veins. This has helped to establish that these peripheral veins drain the adrenal gland. Therefore, we support the findings of Brauckhoff and Walz, that division of the adrenal vein can be performed safely without causing venous congestion and nonfunctioning of the adrenal remnant. However, when the main adrenal vein is divided, excessive mobilization of the adrenal gland should be avoided due to concern that the above-mentioned peripheral veins may be destroyed and, potentially, result in a nonfunctioning adrenal remnant.
It was clear, from our cadaver dissection, that the adrenal gland is supplied by many small arteries that surround the gland. This is in agreement with Anson et al. 4 In their study of 450 cadavers, it was observed that the adrenal gland is supplied by up to 60 small arteries originating from the aorta, as well as the inferior phrenic and renal arteries. Therefore, it would appear unlikely that the adrenal remnant would become ischemic due to inadequate arterial supply during a subtotal adrenalectomy. An almost complete mobilization of the adrenal remnant would be required to achieve this.
Factors other than adrenal blood supply should also be considered to preserve adrenal remnant function. Selection is important, as small, isolated, peripheral, and well-demarcated lesions are most suitable. Centrally placed lesions can make the procedure more demanding or, in some cases, impossible. At initial dissection, a decision is made to divide or preserve the adrenal vein. Careful mobilization of the adrenal tissue containing the lesion is performed. Subtotal adrenalectomy is then performed by using ultrasonic dissection. Using this technique, collateral damage to adjacent tissue is limited to less than 5 mm. Alternatively, a vascular stapler can be utilized. However, it is important to leave a sufficiently functioning adrenal remnant. Brauckhoff et al., 16 in a series of 22 patients, found that an adrenal remnant size <25% of normal gland size should be avoided to prevent adrenal hypofunction. Intraoperative ultrasound may be used to determine normal adrenal tissue and identify the resection margins.
Conclusions
This study has shown, during LSA, that a nonfunctioning adrenal remnant is unlikely due to an inadequate arterial supply. Division of the main adrenal vein can be performed safely without risk of venous congestion. However, once the main adrenal vein is divided, excessive mobilization of the adrenal remnant should be avoided to prevent destruction of the smaller peripheral veins necessary for venous drainage.
Disclosure Statement
No competing financial interests exist.