
Abstract
Abstract
Objective:
The aim of this pilot study was to assess the safety, feasibility, and short-term outcomes of transumbilical multiple-port laparoscopic cholecystectomy (TUMP-LC), using conventional laparoscopic equipment, and to compare it with the currently published studies on single-incision laparoscopic Cholecystectomy.
Materials and Methods:
During the 4-month study period, data from all consecutive patients referred for cholecystectomy to the General and Minimally Invasive Surgery Unit of our institution who agreed to undergo TUMP-LC were included in a prospective study. Outcome measures included completion rate of attempted TUMP-LC, operative time, conversion rate, length of hospital stay, postoperative pain, and assessment of complications. The data were analyzed and compared with studies obtained from a MEDLINE search on four-port laparoscopic cholecystectomy at its initial period and recently published studies of single-incision laparoscopic cholecystectomy.
Results:
Fifty patients completed our protocol. In 47 patients, TUMP-LC was completed successfully without any complications. In 2 patients, the procedure was converted electively to a standard four-incision laparoscopic cholecystectomy without any additional morbidity. In 1 patient, an additional epigastric 5-mm port had to be placed to control bleeding from the gallbladder fossa. One patient had a postoperative biliary leak from an accessory duct in the gallbladder fossa, which was managed by endoscopic retrograde cholangiopancreatography and biliary stenting.
Conclusions:
TUMP-LC is both feasible and safe. It can be performed with standard laparoscopic instruments, and, thus, there is minimal additional challenge to an experienced laparoscopic surgeon. With progressive experience and development in technology, TUMP-LC will probably be performed widely. But, disciplined, evidence-based investigations and randomized studies comparing it to existing techniques must be carried out before the actual place of this procedure in current surgical practice is determined.
Introduction
Materials and Methods
This was a prospective trial conducted at Fortis Escorts Hospital and Research Center, (Faridabad, India). Patients presenting with symptoms of Biliary colic and Ultrasound confirmed cholelithiasis was properly consented to undergo TUMP-LC. All operations were performed by the same surgical team that was specially trained in this type of surgery. Our first TUMP-LC operation on a human was performed in May 2009. Between then and August 2009, a total of 50 patients have undergone TUMP-LC under an institutional review board–approved protocol. Exclusion criteria were age >75 years and body mass index (BMI) >34.
Operative time and intraoperative complications were monitored. Postoperative analgesia requirement and duration of stay were noted. Follow-up of 1 month and time to return to normal activity and wound infection were recorded. Since the inception of the TUMP-LC technique at our center, it has undergone a series of modifications. Certain aspects of the procedure remained constant throughout, while others were altered as we learned from our experience. Below, we will attempt to describe each of these changes as they were introduced to give a sense of the evolution of the procedure.
Operative technique
The patient position was similar to the standard four-port laparoscopic cholecystectomy, with the patient in the supine position, the surgeon and assistant on the patient's left side, and the monitor near the patient's right shoulder. The procedure for the initial 10 cases was performed through a transumbilical incision about 20 mm in size (Fig. 1). The pneumoperitoneum was created with a Veress needle. A 10-mm port was placed, through which a 45-cm 50-degree laparoscope (HD 50° Panoview Richard Wolf, Vernon Hills, IL) was introduced. Two 5-mm ports were placed 1 cm anterior and to the right and left of the 10-mm ports (Fig. 2). The 5-mm port placed on the left side was a reusable, metallic, low-profile valveless port, which was self-fabricated and used after the first 15 cases. As it was a valveless port, there was a reasonable range of movement between all three ports. The gallbladder was retracted with a suture passed through the fundus to the right-upper abdominal wall. Dissection was done by using both standard instruments and articulating graspers and dissectors. The dissecting instruments were crossed over intracorporeally to carry out the surgery.

Umbilical flap for port placement.

All ports placed through the umbilicus.
The aim of the operative procedure was the same as with conventional laparoscopy, that is, dissection of the gallbladder until the critical view of safety was obtained, followed by transection of the cystic duct and cystic artery and removal of the gallbladder. The critical view of safety was obtained when the triangle of Calot was dissected free of all tissues, except for the cystic duct and artery, and the base of the liver was exposed. 23 The cystic duct and artery were then clipped by using LT 300 endoclips (LIGACLIP®; Ethicon Endo Surgery, Guaynabo, Puerto Rico). Exchange of the telescope from 10 to 5 mm was done during use of the clips. The gallbladder was placed in a self-fabricated tissue-retrieval bag made of a polythene bag 10 × 8 cm in size with a 1-0 nylon suture tied as a purse string at its opening (Fig. 3). The gallbladder was inserted in the endobag and removed through the 10-mm port. All ports were then closed with port-closure (braided and coated polyglycolic acid No. 1, ½ circle, reverse cutting 23-mm) sutures.
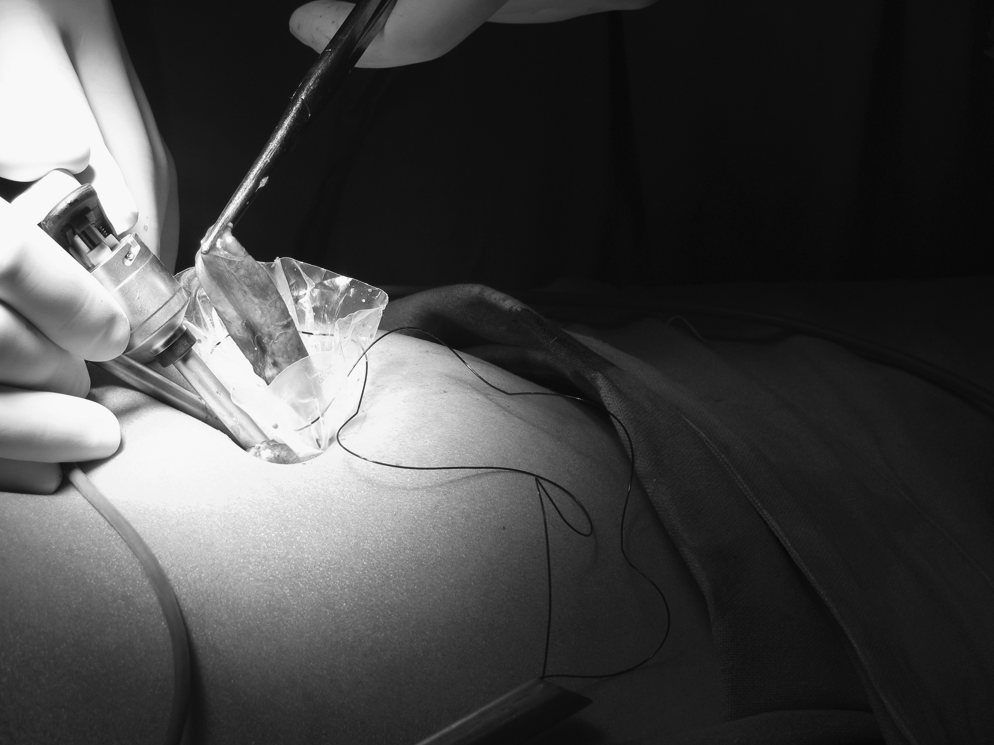
Gallbladder delivered out through a specially designed endobag.
During the initial 10 cases, we encountered several technical challenges. The traction at the fundus of the gallbladder by the suture was not adequate for proper dissection. Also, the change of telescope for clipping the cystic artery and duct increased the operative time. The use of articulating graspers and dissectors was also technically difficult, as they were flexible, and it also increased operative costs. The flaps raised to place the ports at the umbilicus led to seroma formation in 2 patients.
The following modifications to the above technique were done after reviewing the difficulties faced in the first 10 cases.
Placement of a fourth 5-mm grasper for fundal retraction through the umbilical incision just lateral to the 10 mm port. This was placed without any port. Thus, the fundal traction could be manipulated, as required, and this grasper was not changed until the end of surgery (Fig. 4). Use of a 5-mm endoclip (Autosuture™; US Surgical, Norwalk, CT) applicator, thus reducing the time for telescope change (Fig. 5). Curvilinear incision along the lower border of the umbilicus without raising any flaps. We used only conventional laparoscopic instruments, as we encountered difficulty in firm grasping and retraction of the gallbladder with articulating instruments. Surgery was preferably carried out without the crossing over of hand instruments intracorporeally.

Gallbladder fundus held with a grasper placed without a port.
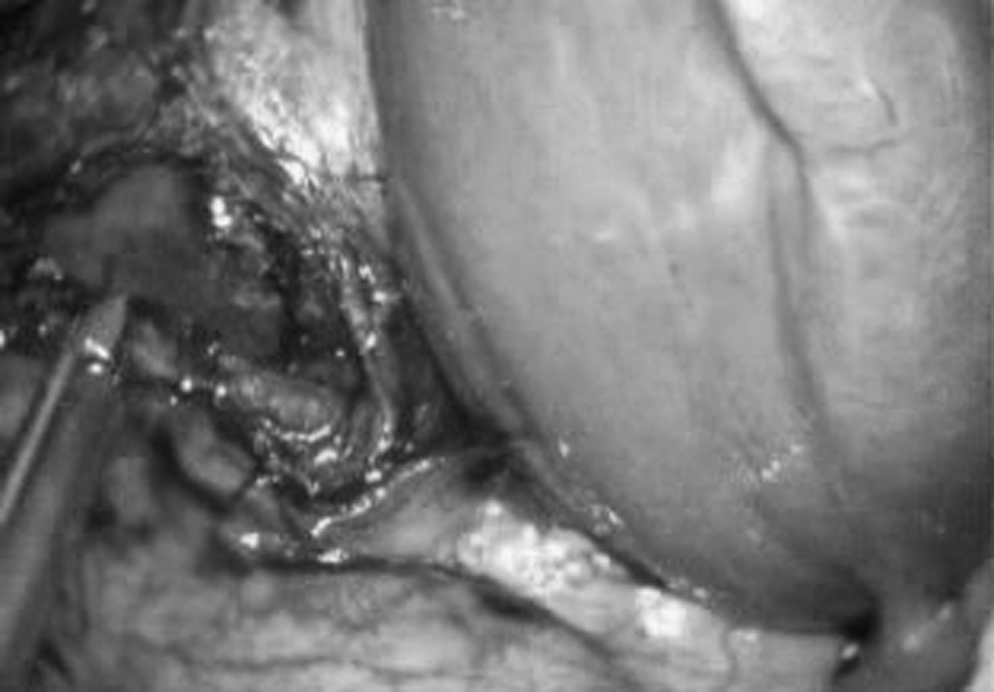
Calot's triangle dissected and cystic duct clipped.
Results
Fifty consecutive patients underwent TUMP-LC over a period of 4 months, from May to August 2009. Of these patients, 38 were female and 12 male. The average age of patients was 44.98 years (range, 23–70). Twenty-six of these patients, all of whom were females, had previous abdominal surgeries, which were cesarean sections (21 patients) and open abdominal hysterectomy (5 patients).
Intraoperative difficulties, complications, and conversions
Adhesiolysis for significant adhesions to the gallbladder was carried out in 32 cases, using routine monopolar cautery dissection without any intraoperative complications. In 2 patients (4%), the procedure had to be converted electively to standard four-port laparoscopic cholecystectomy due to dense adhesions in the region of Calot's triangle and inability to clearly define the anatomy in the region. The surgery was completed without any complication, and the patients had an uneventful recovery. None of the patients required a conversion to an open procedure. In 1 patient, an additional 5-mm port had to be placed from the epigastric region due to bleeding from the gallbladder fossa resulting in poor visualization. However, hemostasis was quickly achieved after the port placement and required no blood transfusion.
In the other 47 (94%) patients, the surgery was completed through a single incision. There were no intraoperative complications. None of the patients required intra- or postoperative blood transfusions. It should also be noted that, in 3 cases, there was spillage of multiple calculi during the gallbladder dissection, which resulted in some technical difficulty in the extraction of stones, as they had to all be collected in the endobag before extraction, resulting in increased operative time.
Duration of surgery
We divided our cases into five groups for a comparative study of the duration of surgery: group A (first 10 cases); group B (second 10 cases); group C (third 10 cases); group D (fourth 10 cases); and group E (fifth 10 cases). In group A, the mean operative time was 87.77 minutes, while it decreased significantly to 53.5 in group E. The trend toward a reduction in operating time with increasing surgical experience (Fig. 6) was confirmed, with the Pearson's coefficient being −0.43.

Length of operation for TUMP-LC; there is a moderate negative correlation with a Pearson's coefficient of −0.43.
Postoperative stay and complications
Postoperative stay varied from 1 to 3 days. Median duration of stay was 1 day. All patients were given pre- and postoperative antibiotics as per hospital antibiotic policy. None of the patients required the placement of intra-abdominal drains. Postoperative analgesia was covered adequately by the injection of diclofenac sodium (75 mg) twice-daily on the day of surgery. No patient required added analgesia.
One patient was readmitted on postoperative day 5 with pain in the abdomen. Ultrasonography showed free fluid in Morrison's pouch. Diagnostic Laparoscopy showed bilious collection in Morrison's pouch of about 500 mL. An accessory duct was visualized in the gallbladder fossa, and the duct was clipped by using a 5-mm endoclip. Endoscopic retrograde cholangiopancreatography, (ECRP), carried out during the same anesthesia, demonstrated normal a cystic duct and both hepatic ducts; no contrast leakage was visualized. A papillotomy as done, and a 10-Fr biliary stent was placed. A drain was placed in the gallbladder fossa. The patient was discharged with the drain, which was removed after 15 days. Three patients developed a seroma at the umbilicus, which was noted at the first postoperative visit at the outpatient department after 1 week. It subsided on conservative management. Postoperative scar followed on OPD until 7 days after discharge was satisfactory (Figs. 7 and 8). The median times to full activity and normal employment were 4 (range, 3–9) and 8 days (range, 6–14), respectively.

Immediately postoperative incision site.

Postoperative scar after 7 days in OPD.
Discussion
The evolution of laparoscopic surgery has transformed many disciplines, allowing multiple procedures to be performed via a laparoscopic approach. This, along with enhanced recovery programs, has shortened the length of hospital stay and has led to a reduction in morbidity related to the surgical wound. The standard approach to laparoscopic cholecystectomy consists of four skin incisions, where four separate ports are placed: one for the optic source and three for surgical instruments. SILS refines the use of laparoscopic surgery, allowing procedures to be carried out through a single incision, making the procedure even more minimally invasive. Single-incision laparoscopic cholecystectomy was first reported by Navarra et al. 19 in 1997 and Puskin and Rajpal 20 in 1999. However, technical limitations delayed its development in the initial period. With gradual advancement, a number of procedures, including cholecystectomy, appendicectomy, hysterectomy, urologic procedures, adrenalectomy, and bariatric procedures, are being treated by this methodology.
As with any new surgical technique, there is a learning curve. Single-incision laparoscopic cholecystectomy is technically more challenging, compared with conventional laparoscopic cholecystectomy. In-line positioning of the laparoscope, close proximity of working instruments with limited triangulation, limited range of motion of the laparoscope and instruments, and decreased number of ports all contributed to increased difficulty. The major technical difficulty of single-incision laparoscopic cholecystectomy stems from the use of crossed-over instruments. This requires the surgeon to “reprogram” his hand-eye coordination, because his right hand will be moving the left-sided instrument and the left hand the right-sided instrument on-screen. We overcame this limitation by carrying out the operations without the cross-over of instruments after the first 10 surgeries. In our study, of 50 patients, in 47 (94%), the procedure was completed successfully. Tacchino et al. 21 (12 patients) and Albrink et al. 22 (9 patients) reported no conversion and a 100% successful completion rate. However, in the series of 29 patients by Philipp et al. 23 a 48% successful completion rate was reported, with the remainder requiring one to three additional skin incisions.
It is logical to compare the conversion rate of TUMP-LC to that of the standard laparoscopic cholecystectomy. In effect, it would denote the failure rate to perform the attempted procedure. However, it must be noted that the conversion of a standard laparoscopic cholecystectomy signifies a conversion to an open procedure, while in the single-incision laparoscopic cholecystectomy, it is, initially, a conversion to a standard laparoscopic procedure or, ultimately, an open procedure. Also, a reasonable comparison, if at all, should be made with laparoscopic cholecystectomy at its initial period. So, in comparison, a similar study of 100 initial cases of laparoscopic cholecystectomy 24 had a conversion rate of 4%. The Mayo Clinic experience 25 of its initial 200 cases of laparoscopic cholecystectomy had a conversion rate of 2.5%, and a series of 303 patients by Dolan et al. 26 had a conversion of 3.9%. However, in our series, a conversion of 4% to the standard laparoscopic procedure, without any conversion to open, signifies that an early conversion in the face of difficulties does not have any adverse effects on patient outcome or cause additional morbidities in patients. In comparison with recent studies on single-incision laparoscopic cholecystectomy, Hernandez et al., 29 in their series of 100 cases, reported no conversions, while Kuon Lee et al. 30 had a conversion of 5 cases in their study of 37 (31.5%). It is probable that, with experience and technological advancements, the conversion rate will gradually decrease.
The technical constraints, as well as the inevitable learning curve, may, obviously, lead to an increased operative time for single-incision laparoscopic cholecystectomy procedures. In our series, there was a trend toward reduced operative times with more experience, as demonstrated by a Pearson's coefficient of −0.43 for TUMP-LC. The average operative time in the last 10 cases was 53.5 minutes (Table 1). In the study by Tacchino et al., 21 of 12 patients undergoing single-incision laparoscopic cholecystectomy, the operative time stabilized to an average of 50 minutes after first 5 cases, which is almost similar to our study. The average operative time in the study by Albrink et al. 22 on 9 patients was 73 minutes. Similarly, Vidal et al. 27 reported that a median operating time of 62 minutes in the LESS group was not significantly different than that in the standard laparoscopic cholecystectomy group. In the study by Philipp et al., 23 the operative time was significantly longer in single-incision laparoscopic cholecystectomy (29 cases), compared with conventional laparoscopic cholecystectomy (22 cases) (85 versus 67 minutes; P = 0.01). However, historic data of 50 consecutive patients, who were operated on immediately prior to the commencement of the current series at our center by standard four-port laparoscopic cholecystectomy, had an average operative time of 49.16 minutes (range, 30–70), which is not statistically significant to the operative time of TUMP-LC (P-value, 0.83). Thus, operative time with TUMP-LC approximated the time of standard laparoscopic cholecystectomy, as the learning curve was crossed, and one can be confident that, with experience, the operative time of TUMP-LC will reduce further.
Bleeding from gallbladder fossa needed one extra epigastric port.
Mesenteric injury and an inadvertent injury of the right hepatic duct.
All conversions to standard laparoscopic cholecystectomy.
Minor complication 3 wound seroma.
Three patients had pain control issues and 1 had urinary retention).
One major complication of an accessory bile duct leak in our study was managed by relaparoscopy and clipping of the duct, followed by ERCP and stenting (Table 1). A similar complication of postoperative biliary leak from an accessory duct of Lushka, following single-incision laparoscopic cholecystectomy, was reported by Chow et al. 28 Hernandez et al. 29 reported 1 patient with a cystic stump leak in their series of 100 cases. It may be reasonable to assume that, possibly, the visualization in single-incision laparoscopic cholecystectomy is, to some extent, inferior, compared to standard laparoscopic cholecystectomy, which requires a more cautious approach during dissection. Minor complications (e.g., seroma, wound infection) occurred in 3 patients (6%). All these 3 cases occurred in our initial 10 cases; the application of pressure dressing with a specially designed abdominal belt applied for 2 weeks and the change of incision from trans- to infraumbilical in the later cases reduced its incidence to nil. None of the above studies on single-incision laparoscopic cholecystectomy have reported the incidence of minor wound complications. Postoperative analgesia requirement was similar to the standard laparoscopic cholecystectomy. However, Philipp et al. 23 reported a tendency toward greater postoperative pain in the single-incision laparoscopic cholecystectomy group. The median postoperative duration of stay was 1 day (range, 1–3) is comparable to conventional four-port laparoscopic cholecystectomy (1 day) at our center.
The concept of single-incision surgery is attractive and an understandable innovation, as laparoscopic surgery has become more commonplace. But there are important issues that should be addressed as it is further developed and used. Is there hope in decreasing pain and having a faster recovery through single-incision laparoscopic cholecystectomy? Is it worth performing single-incision surgery for improving cosmesis? In answer to the first question, indirect evidence can be found in the study conducted by Bisgaard et al., 31 who reported a lower 1-week morbidity in a group of patients subjected to laparoscopic cholecystectomy with down-sized trocars. Moreover, as cosmetic improvement becomes increasingly important to patients, this advantage in single-incision laparoscopic cholecystectomy cannot be ignored, especially when it is performed through the umbilicus. However, prospective, randomized, multicenter trials are needed for comparing standard laparoscopy to single-incision laparoscopic cholecystectomy in order to understand the outcome benefits, if any. Although there are obvious theoretic benefits, the practical benefits and potential risks are still unclear. But the fact that laparoscopic cholecystectomy is currently the gold standard and is being liberally performed in almost all hospitals worldwide, and is being considered safe and effective, should not limit its further technical evolution. The technical challenge and the use of expensive instrumentation are common reasons leading to hesitation in embarking upon any new technique. The procedure of single-incision laparoscopic cholecystectomy can be made more acceptable by making it ergonomically matched to the standard four-port technique, just as we have moved away from the articulating and crossing over of instruments toward the standard orientation of instruments, as in four-port laparoscopic cholecystectomy.
Conclusions
To conclude, TUMP-LC has the potential to offer real benefits to patients, but the actual outcome is still unclear. Prospective studies are needed to determine the impact on postoperative pain, recovery, wound complications, patient satisfaction, and cosmesis to identify advantages over the standard laparoscopic cholecystectomy. The development of a standardized technique and additional experience is needed for more consistent success. Nonetheless, in the present scenario, we found the single-incision laparoscopic cholecystectomy to be safe, effective, and feasible.
Footnotes
Disclosure Statement
No competing financial interests exist.