
Abstract
Abstract
Background:
Laparoscopic cholecystectomy has become the standard, in most pediatric surgery centers. In the search for a less-invasive procedure, a single-incision laparoscopic approach has been reported in adults and very few children.
Objective:
The aim of this study was to present our initial experience of cholecystectomy, using single-incision pediatric endosurgery (SIPES), including the technique, the intraoperative challenges, and the outcome.
Methods:
All pediatric patients who underwent a SIPES cholecystectomy from March through September 2009 were prospectively evaluated.
Results:
Twenty-five children underwent a SIPES cholecystectomy. The most frequent indications were symptomatic cholelithiasis in 17 patients (68%) and biliary dyskinesia in 5 (20%). Five patients had sickle-cell anemia. The mean operative time was 73 minutes (range, 30–122). Median hospital stay was 1 day. In 17 patients (68%), a percutaneous 2-mm grasper was used to retract the gallbladder over the liver. No complications were noted, and no conversion to an open procedure was required. In 5 patients, additional trocars were added. On follow-up, 3 days to 2 months later, no complications were noted. No patients were readmitted, and there were no wound infections.
Conclusions:
Cholecystectomy, when using the SIPES approach in children, is a safe, reasonable alternative to conventional laparoscopy, leaving an inconspicuous scar. Whether SIPES offers any further benefit to the patient, besides improved cosmesis, should be evaluated in future studies.
Introduction
Methods
Approval from the institutional review board of our hospital was obtained (protocol no.: X090814001). All pediatric patients who underwent a SIPES cholecystectomy from March through September 2009 were prospectively evaluated. Variables entered into the database were age, weight, gender, indication for the procedure, operative time, blood loss, intra- and postoperative complications, and postoperative hospitalization times. Information on the follow-up in the outpatient setting after discharge was also available. Operative times were analyzed over the course of the observation interval for a possible learning curve.
Technique
The patient was placed in the supine position, then securely taped and strapped to the operating table. The surgeon stood on the patient's left and the assistant on the right, with the dual monitors placed on opposite sides. A 2-cm vertical transumbilical incision was performed, and an area of approximately 3 cm of fascia was cleanly dissected to provide adequate access. In most cases, a 5-mm expandable Step™ trocar (Covidien, Mansfield, MA) was placed in the middle of the umbilicus, and the capnoperitoneum was insufflated. Two further 5-mm trocars were placed in separate umbilical fascial incisions at the 2 and 10 O'clock positions (Fig. 1A). A separate grasper for gallbladder retraction was placed through a stab incision without a trocar in the inferior part of the wound. A 5-mm diameter, 54-cm-long, 30-degree endoscope was used with a right-angle light-cord adapter. In selected cases, a 2-mm MiniLap Alligator grasper (Stryker Endoscopy, San Jose, CA) was placed directly through a stab incision in the right flank to facilitate retraction of the gallbladder. In some older adolescents, a special SILS™ trocar (Covidien) was used for umbilical access (Fig. 1B).
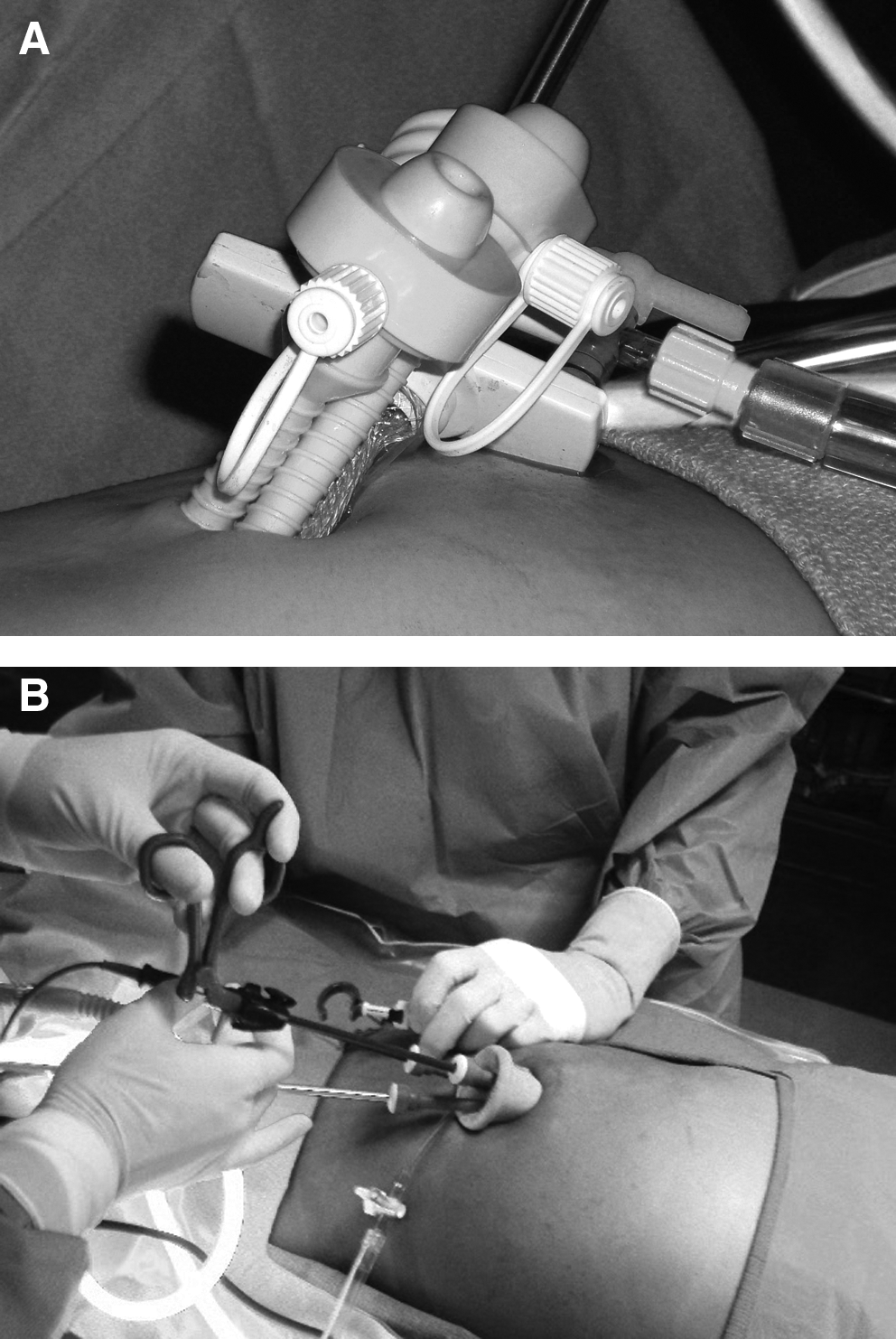
Trocar placement, using individual trocars (
The actual gallbladder dissection corresponded to the standard laparoscopic technique. In most cases, standard nonroticulating instruments were used, and dissection of the Calot triangle was performed with hook electrocautery and a Maryland grasper. The duct was clipped by using 5-mm polymer Weck clips (Teleflex Medical, Research Triangle Park, NC). Once the gallbladder was free, the Step trocar was upsized to 10 mm to accommodate the endoscopic retrieval bag, in which the gallbladder was removed from the abdomen. The capnoperitoneum was desufflated and the fascial incisions were closed by using 2-0 polydioxanone sutures. Skin was closed by using interrupted 4-0 poliglecaprone subcuticular stitches.
Results
Between March and September 2009, 25 children underwent a SIPES cholecystectomy in our division. The operations were performed by three attending surgeons. Of the 25 patients, 20 were females. The mean age of the patients was 12 years (range, 8–17). Mean weight was 54 kg (range, 22–107). Indications included 17 patients with symptomatic cholelithiasis (68%), of which 5 had sickle-cell anemia. Further, 5 patients were diagnosed with biliary dyskinesia (20%), 2 patients with acute cholecystitis, and 1 with chronic abdominal pain.
The mean operative time (from incision to completed wound closure) was 73 minutes (range, 30–122). Using a linear regression curve, there was a weak trend toward decreased operative times over the study interval (Fig. 2). Median hospital stay was 1 day (range, 1–4), and mean recorded blood loss was 5.2 mL. All procedures were completed laparoscopically. In 17 patients (68%), an additional 2-mm Alligator grasper (Stryker Endoscopy) was introduced percutaneously through a stab incision in the right-upper quadrant to grasp the gallbladder and to retract it over the liver.

Operating times (incision to closure) in minutes (y-axis) versus date (x-axis).
No complications were noted during the procedures. No conversion to an open procedure was required; but, in 5 patients (20%), additional trocars were added. In 4 of these, two additional 5-mm trocars were added due to difficulty in the dissection of the structures in the Calot triangle. In another patient, a 10-mm trocar was added because of a large cystic duct that required a 10-mm clip placed at an angle.
In 5 patients, a liver biopsy was performed in the same operation, using the 2-mm right-upper quadrant stab incision of the Alligator grasper (Stryker Endoscopy) for the biopsy needle. In the patient with chronic abdominal pain, an appendectomy was performed after the cholecystectomy, using the same single umbilical incision. One of the patients with symptomatic cholelithiasis had an incidentally discovered omphalomesenteric band that was recognized and divided without difficulty and without placing additional ports. All patients were given a regular diet within hours after surgery. Children with sickle-cell anemia were admitted for 2 days postoperatively and given intravenous hydration and oxygen via a nasal cannula to reduce the risk of erythrocyte sickling. All others were discharged on postoperative day 1.
Follow-up information was available for 21 patients, with a median follow-up time of 3 weeks (range, 3 days to 2 months). Once healed, the scar was barely visible and had contracted in length (Fig. 3). Sixteen children had no abdominal pain when seen in the outpatient clinic. Five patients had either persistent or recurrent abdominal pain, either at the umbilical incision site (n = 2) or in the right-upper quadrant and epigastrium. One patient had transient right-shoulder pain for 2 days following the procedure. There were no wound infections recorded.

Postoperative scar.
Discussion
In 1997, Navarra et al. 7 performed the first laparoscopic single-incision cholecystectomy in adults. Since then, the number of publications have increased substantially every year. However, in the pediatric age range, only a few reports with a small number of patients are available.4–6 To date, this is the largest series of SIPES cholecystectomies published.
We did not select the patients for the procedure preoperatively, but offered this new technique to all our patients who were scheduled for cholecystectomy during the study period. Potential risks and benefits were explained, and the patient and parents were made aware of the possibility of adding additional trocars, access sites, or conversion to an open technique, if the surgeon deemed this necessary, during the procedure. The indications very much resembled our standard practice before the introduction of SIPES.
Our mean operative time of 73 minutes was comparable to that published for single-incision laparoscopic cholecystectomies in adults, which ranged from 40 to 150 minutes in a systematic review article. 3 In the previously published pediatric studies, the mean operating time ranged from 304 to 99 minutes. 5 Of note, our patient population was not preselected, so that children with acute cholecystitis and gallbladder hydrops were included. Further, in some of our cases, additional procedures, such as the liver biopsy and appendectomy, were part of the operative times.
We were surprised to find that although the frequency of SIPES cholecystectomies increased over the study period, we could not demonstrate a substantial learning curve. This may be due to the fact that basic surgical principles of SIPES do not differ much from those of conventional laparoscopic cholecystectomies, and that the challenges are overcome relatively quickly. Of note, the 25 procedures were distributed among three attending pediatric surgeons, who operated with different fellows and residents. Under these circumstances, it may take larger numbers to demonstrate an improvement in operative speed.
In almost two thirds of cases, liver retraction was achieved by placing a 2-mm Alligator grasper (Stryker Endoscopy) through a stab incision in the right-upper quadrant. This was particularly helpful in large or obese children, where retraction from the umbilicus requires a relatively long locking grasper to give adequate exposure. Another option, described in the literature, 4 is to retract the gallbladder with a percutaneous suture from the right-upper quadrant. However, we have no experience with this method of retraction, at this time.
We found that roticulating instruments were sometimes helpful, but not necessary, to perform the operations. Instrument clashing was avoided by using a long telescope, which separated the hands of the surgeon from the assistant's. Lateral retraction of the gallbladder with the left hand during the dissection phase effectively kept both of the surgeon's hands from getting in their way. This maneuver leads to a crossing of the instruments at the umbilicus, which can feel awkward, at first. Using a special SILS (Covidien) trocar added convenience, but was not essential. Clashing of the surgeon's hands can be further minimized by using two instruments of different lengths. A surgeon should be aware that using single-use roticulating instruments and special single-incision access trocars significantly increases the cost of the procedure. No intraoperative or postoperative complications were noted in our series. We feel that it is important to realize that trocars should be added when the visualization or workspace limitations of the SIPES approach compromises the operation. Following this premise, the SIPES cholecystectomy seems to be a safe procedure without increased morbidity for the patient.
Our follow-up consisted of at least one postoperative visit to the outpatient clinic. At that time, photodocumentation of the umbilical incision was performed, in most patients. The families were instructed to call for any problems regarding the incision or abdominal symptoms. A formal pain assessment was not performed in this study, but, subjectively, we did not appreciate a reduction of postoperative pain, compared to standard laparoscopy. This is an issue that warrants further investigation, since decreased pain is one of the acclaimed arguments in favor of laparoendoscopic single-site surgery.
Conclusions
In summary, a SIPES cholecystectomy for a variety of indications in children is a safe, reasonable alternative to the conventional laparoscopic approach. If the surgeon feels that workspace or visualization is suboptimal during the operation, additional trocars should be added. Whether SIPES offers any further benefit to the patient, besides improved cosmesis, is open to debate and should be evaluated in future studies.
Footnotes
Disclosure Statement
No competing financial interests exist.