
Abstract
Abstract
Introduction:
An inanimate technical skills trainer for laparoscopic pyloromyotomy (LP) has not been described. A middle fidelity model, reproducing the three consistent steps in LP, was developed as a component of a teaching module for surgical residents, and tested on medical students, residents, and pediatric surgeons.
Materials and Methods:
In the first phase of the study, a cohort of 29 pediatric surgeons used the LP model and completed questionnaires about the model's realism and accuracy. Descriptive statistics were used to analyze questionnaire responses. Chi-square tests were performed to determine if level of experience influenced responses. For the second phase of the study, medical students and surgical residents individually participated in the training of cognitive knowledge about hypertrophic pyloric stenosis and skills acquisition for LP. Subject testing consisted of simulator task performance and multiple-choice quiz administration immediately after training and repeated at 8 weeks after training. Data were analyzed by using paired sample t-tests and one-way analyses of variance (ANOVA).
Results:
The pediatric surgeons agreed that the model accurately simulated essential components of the pyloromyotomy, and that the model would be an excellent tool to introduce surgeons to LP. A total of 26 students and early surgical residents completed the training and testing. Knowledge-based test performance improved from pre- to postinstruction by 17.45 [standard error of the mean (SEM) + 3.5] (P < 0.001) and from preinstruction to 8 weeks by 4.54 (SEM = 3.2) (P = 0.17). Mean improvement in time of simulator task performance was 85.2 ± 75.4 seconds. Based on a one-way ANOVA, higher level of training was associated with decreased mean times (P = 0.04).
Conclusions:
Face and content validities of the simulation were demonstrated by the pediatric surgeons. An effective training experience was demonstrated with medical students and residents. At 2 months, simulator task-completion rates and task-performance times showed technical skills were retained, whereas, based on test scores, cognitive knowledge was not as well retained.
Introduction
One of the ongoing debates in surgical education is the optimal use of precious operative time for training. Gone are the days when residents would stand in the operating room and observe many operations before participating in them. Reduced work-hour restrictions have had many positive results, but one of the challenging consequences continues to be the imparting of surgical skills to our residents with less operative theater exposure than previous generations. This observation has led to the necessity of skills acquisition outside of the operating room and the subsequent incorporation of training centers into resident training programs. 9 Each residency has tried to tackle this task in different ways. Skills acquisition in minimally invasive surgery (MIS) is one area where training and practice outside the operating room was already in place and accepted before the duty-hours restrictions. The most obvious example of this training outside the operating room is the Fundamentals of Laparoscopic Surgery (FLS) curriculum. Formal completion of the FLS curriculum through the American College of Surgeons is now a requirement for all residents in training. 10 These “skills training” exercises continue to expand. Common to all of these is the development of individual “skill sets” or maneuvers that are common to many procedures (e.g., separating different types of tissue, cutting, and sewing) or specific to others (e.g., fashioning a posterior wrap of the fundus around the esophagus). The procedure for performing an LP incorporates common skills from other minimally invasive procedures and three skills that are nearly unique to this procedure. Designing a model to teach and practice these unique skills for the LP can provide a safe environment in which to develop the necessary skills outside the operating room and minimize operative complications.
There are three main types of models currently used in surgery simulation, and these models may be low, middle, or high fidelity. Hybrid simulators can be generally thought of as middle fidelity simulators, in that they use a box with inanimate objects or organs. Hybrid simulator performance evaluation does not require observation and feedback by an experienced surgeon, because performance can be monitored by a computer, which is able to give objective feedback, based on preprogrammed metrics. These simulators also provide the same tactile feedback as actual surgery.
Laparoscopic pyloromyotomy middle fidelity model
There have been multiple studies demonstrating the need for simulation training in the field of laparoscopic surgery. These studies have shown the validity and reliability of low fidelity models for training purposes. The potential for simulation in pediatric surgery is immense and has yet to be explored thoroughly. Procedures, such as LP, can be accurately simulated by using a middle fidelity model, which demonstrates construct validity.
The middle fidelity model used in the training of LP is the adaptation of a low fidelity model placed into a hybrid environment. An inanimate LP model was inserted into the ProMIS® trainer (Fig. 1). The ProMIS (Haptica, Inc., Boston, MA) is a hybrid simulator combining a box simulator and a computer. Real instruments can be passed through ports enabling the manipulation of objects in the box, and feedback and analysis is achieved by tracking the instruments in three-dimensional space. The ProMIS is able to compare the performance of the trainee to a defined proficiency level. 12 A comparative study, by Botden et al., concluded that the ProMIS AR laparoscopic simulator provided haptic feedback, didactic value, and construct validity to the user, with a laparoscopic cholecystectomy as the procedure. We utilized the ProMIS software to “create” a best-fit model for the skills set in LP 13 (Fig. 2).

Laparoscopic pyloromyotomy model within the trainer.
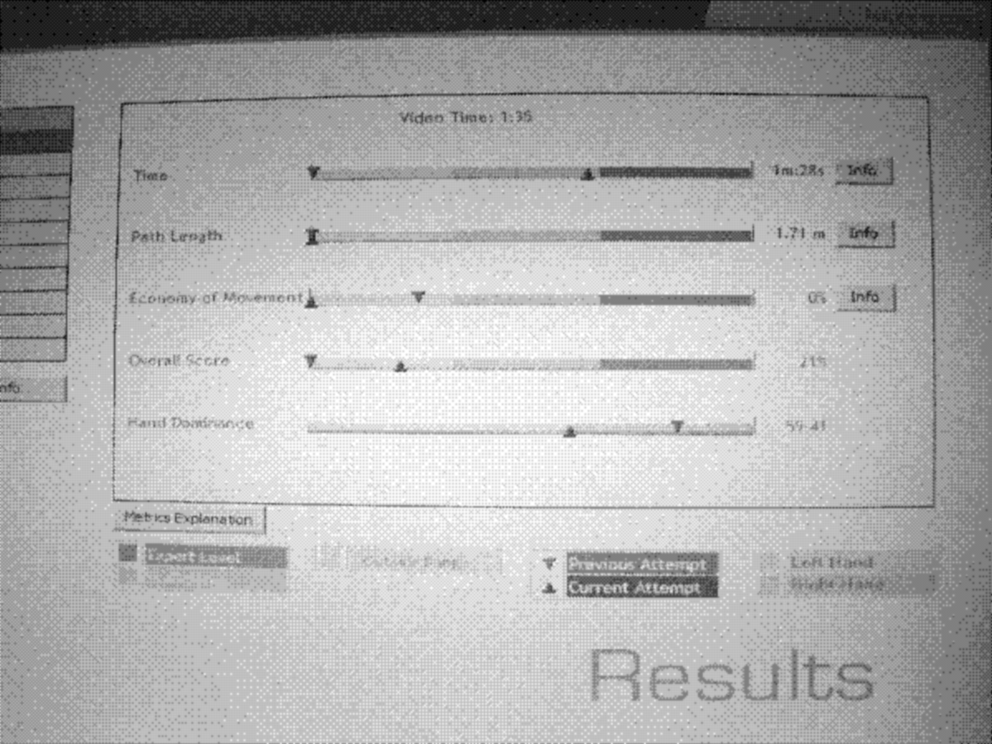
Best-fit movements.
The aims of this study were to assess the credibility of a middle fidelity pyloromyotomy simulation and to pilot test the effectiveness of the simulation used in conjunction with a pyloric stenosis/LP teaching module with medical students and early general surgery residents. The Institutional Internal Review Board approved the study protocol.
Materials and Methods
A middle fidelity model, focusing on the three consistent steps of LP, was developed for training surgical residents. These steps are 1) linear cut in the serosa of the pyloric channel with a retractable knife; 2) “cracking” the muscle with the blunt tip of the knife to begin the myotomy; and 3) completion of the pyloromyotomy, using a pyloromyotomy spreader until both halves of the muscle move independently. The model consisted of simple materials to simulate the stomach and “swollen” pylorus (Fig. 3). For the first phase of the study, a cohort of pediatric surgeons was asked to use the LP simulation. After using the simulation, each surgeon completed a 12-item questionnaire, using a four-point scale about the model's realism and accuracy. The surgeons' responses to the questionnaire items were analyzed from using descriptive statistics, and chi-square tests were used to determine if surgeons' level of experience influenced their responses.
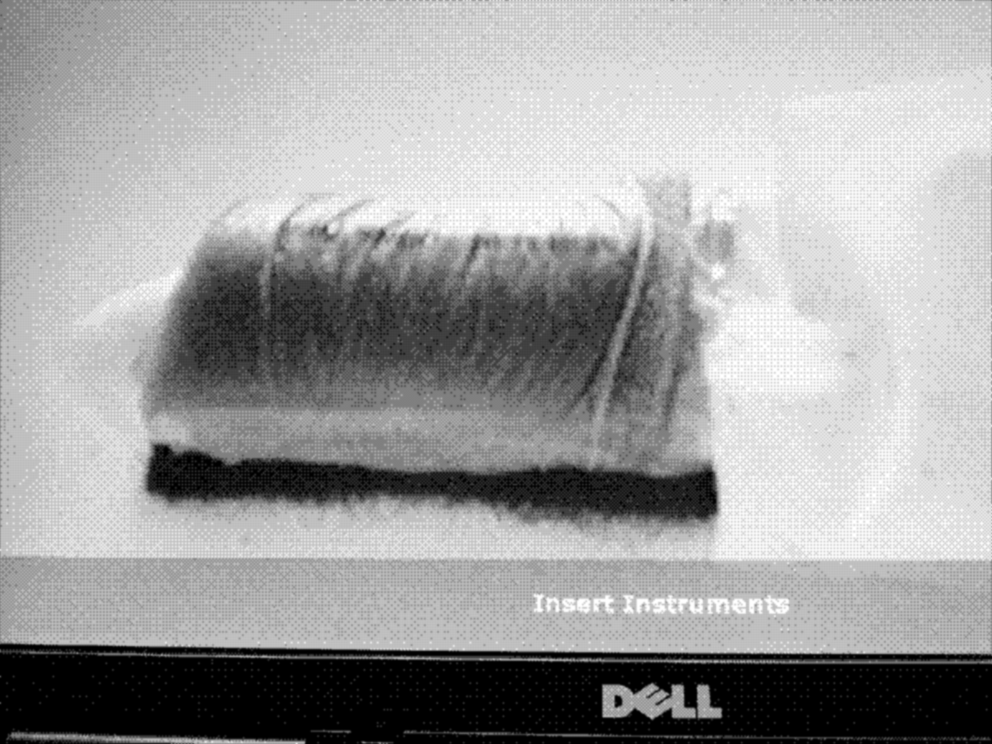
Laparoscopic pyloromyotomy model.
After the pediatric surgeons had verified the credibility of the LP simulation, medical students and junior surgery residents were recruited for the second phase of the study—testing of the effectiveness of a pyloric stenosis/LP as a teaching module. Subjects participated individually in the training and testing. Training materials included 1) a didactic overview of pyloric stenosis, 2) narrated videos of an actual LP and the LP model, followed by 3) two rounds of three attempts, each using the LP simulation. The two rounds of simulation were separated by 8 weeks of inactivity (Table 1). Both videos were narrated by one of the authors (JI). The overview of pyloric stenosis concentrated on care of the newborn with pyloric stenosis, including signs/symptoms, workup, incidence, surgical treatment, postoperative care, and complications. The LP model was inserted into the ProMIS trainer, which automatically recorded information about each subject's performance (Fig. 2).
Before completing training, the medical students and residents completed a questionnaire concerning their level of training and experience with laparoscopic surgery and a multiple-choice test of pyloromyotomy content knowledge. After the initial testing and didactic education, subjects participated in the simulation in two rounds (round 1 immediately after training and round 2 after 8 weeks). In round 1, subjects took the multiple-choice quiz and performed the task (LP) three times, using the LP model. ProMIS automatically recorded unbiased values for each subject's time, instrument path lengths, and smoothness, and a trained observer recorded information on task completion (i.e., whether or not the three steps of the procedure were completed). In order to determine if subjects had retained cognitive information or technical skill from the training period, subjects were retested 8 weeks after training (round 2). In round 2, subjects performed the task by using the LP model three times and then took the multiple-choice quiz. Outcome measures included simulator output: the LP step completion, as recorded by the observer, and preinstruction, postinstruction, and follow-up knowledge-based quiz scores. Data were analyzed from using paired-sample t-tests and one-way analysis of variance (ANOVA).
Results
A total of 29 pediatric surgeons used the LP simulation and completed the 12-item questionnaire, using a four-point Likert scale (1 = strong disagree; 2 = disagree; 3 = agree; 4 = strongly agree). The questionnaire focused on the surgeons' experience with LP, impressions of the model's realism and accuracy, and perception of the model as a teaching tool. Based on the questionnaire responses, a majority of the surgeons (55%) had performed at least 26 LPs in the previous year. Nearly two thirds (59%) of the surgeons' self-perceived skill at performing an LP was advanced or expert. The surgeons agreed that the model accurately simulated essential components of the pyloromyotomy [mean = 3.2; standard deviation (SD) = 0.4). Table 2 presents the surgeons' ratings of questionnaire responses. Based on chi-square tests, no influence on item responses was found, based on level of experience, with pyloromyotomy.
N = 29.
For the second phase of the study, medical students and junior surgical residents were recruited to undergo testing of effectiveness of the three-component LP teaching module. A total of 26 subjects completed the study. Table 3 presents the level of training of the subjects. Twenty-three subjects (88%) completed each of the steps of LP in round 1 (postinstruction simulator use × 3). Three (12%) trainees missed steps in the simulation and were thereby excluded from the time analyses. These subjects were all third-year medical students. For the remaining subjects, mean time was 156 ± 60.9 seconds, and the mean improvement between runs 1 and 3 was 85.2 ± 75.4 seconds. Based on a one-way ANOVA, higher level of training was associated with quicker mean times (P = 0.04) but less improvement between runs 1 and 3 (P = 0.03).
Simulations occurred during two rounds separated by an 8-week delay. Each round consisted of three runs each.
After the 8-week delay, 6 third-year and 3 fourth-year students neglected steps of the pyloromyotomy simulation and had to be removed from time and efficiency analyses. Of the 16 subjects (62%) that completed all steps for both rounds, mean times decreased by 35.05 seconds from round 1 to 2 (P < 0.001) after the 8-week delay. Knowledge-based test-percent scores improved from pre- to postinstruction by +17.45 (standard error of the mean; SEM = 3.5) (P < 0.001) and from preinstruction to 8-week follow-up by +4.54 (SEM = 3.2) (P = 0.17).
Discussion
Tander et al. judged the “learning curve” for LP to be 10 procedures. 11 A study by Vegunta et al. also illustrated that LP operating time decreased progressively with experience. Specifically, the median time required for surgery was 29 minutes in the first 60 cases performed by a group of surgeons, compared to 21.5 in the last 65 cases performed by these same surgeons. In addition, of the total of 7 complications occurring during the cases in the study, 6 occurred during the first half of cases, while 1 complication occurred during the second half. 1 These studies illustrate the ability of surgeons to improve the laparoscopic technique by acquiring proper experience, and a training model that has validity, efficacy, and reliability could help to train surgeons without increased risks to patients during the learning curve. This study successfully created a low-cost middle fidelity model of LP that emphasized the three unique maneuvers required to successfully complete the procedure. The maneuvers in the simulation are the same as during the operation and helps the learner gain experience in the “skills set” necessary to perform an LP. The “tissue” is more forgiving than actual tissue, so that it allows even the novice to practice.
The jump from a low to middle fidelity model involves designing a simulation that teaches the maneuvers necessary for a specific operation or portion of one. It should allow for a reenactment of these maneuvers in real time and in the proper sequence. For this reason, before using the model on test subjects, credibility and face validity must be measured from using a group of “experts” in the procedure. For our model of LP, we tested it on a cohort of pediatric surgeons and credibility was validated by them. This LP model was deemed to provide an effective training experience.
The next step would be to demonstrate that a model is a worthwhile training experience. To do this, one must demonstrate that practicing on it confers the skill on the user and allows the user to retain the skills over time. Construct validity of the LP model was demonstrated. At 2 months, task-completion rates and task-performance times show that technical skills were retained. Interestingly, based on knowledge-test scores, we demonstrated that the initial teaching method (i.e., narrated PowerPoint presentation) significantly improved cognitive knowledge about pyloric stenosis; however, the cognitive knowledge was not as well retained as the skills knowledge after 8 weeks.
Conclusions
The limitations of this study included a small sample of test subjects and the inability to factor in random MIS learning experiences during the 8 weeks in between testing. The ultimate goal of any simulation remains to demonstrate that any given model teaches skills that then correspond to skill attainment in the operating room, which has not been demonstrated with the LP model yet.
Footnotes
Acknowledgments
This work was supported by the Children's Miracle Network. The authors would like to thank Andrew R. Pulito, MD. Dr Pulito was the first “test subject.” Before there was any interest in using this to teach many, the original LP model was designed to teach one.
Disclosure Statement
No competing financial interests exist.