
Abstract
Abstract
Background:
The division of the short gastric vessels (SGVs) is a common practice during laparoscopic floppy Nissen fundoplication (NF) to achieve an adequate mobilization of the gastric fundus. However, the terminal branches of splenic vessels can also be ligated during SGV division, resulting in splenic infarction (SI). The aim of this study was to evaluate our results with SI as a complication of laparoscopic floppy NF.
Materials and Methods:
All patients with direct laparoscopic evidence of SI during laparoscopic floppy NF, between August 1993 and August 2009 and under the care of two surgeons, were included in this retrospective study.
Results:
Over the past 16-year period, 2100 patients underwent laparoscopic floppy NF, and splenic infarction was demonstrated in 20 cases (0.95%). There were 11 women (55%) and 9 men (45%), with a mean age of 35.2 years (range, 25–68). The classic pattern, in all cases, was a small area of infarction, less than 10–15% of the total splenic volume, localized mainly in the upper pole. There were no conversions. The mean length of hospital stay was 1.2 days (range, 1–2). During the follow-up period of 3 months, only 2 patients (10%) had persistent abdominal pain, in which computed tomography demonstrated the infarcted areas involving less than 15% of the splenic parenchyma. All cases were managed succesfully with observation alone.
Conclusions:
Based on the results, partial SI is a recognizable condition during laparoscopic floppy NF. Conservative therapy and close follow-up, without any unnecessary intervention, is an appropriate management that provides a favorable outcome.
Introduction
Whether uncontrolled bleeding occurs or not, the terminal branches of splenic vessels can be injured or ligated during SGV divison, as these branches run posterior to the plane of dissection. This risk is increased in the case of bleeding. 14 Because the peripheral splenic arterial branches have very little collateral circulation, an area of ischemia or infarction will occur immediately distal to the involved branch or branches.14–16 To the best of our knowledge, very few cases of splenic infarction (SI), as a complication of laparoscopic NF, have been described, and little information exists concerning this issue in the literature.11,14,15,17
Since we performed the first laparoscopic NF in August 1993, 2100 patients with proven gastroesophageal reflux disease have undergone this procedure at Istanbul University, Cerrahpasa Medical School (Istanbul, Turkey) and Bahcelievler Medical Park Hospital (Istanbul, Turkey). This study was undertaken to review our experiences with SI following SGV division and to describe, from our material, the clinical importance of this condition. We have also reviewed the literature and combined these data with our clinical data in order to provide a considerably larger group for evaluation.
Materials and Methods
Patients
Of 2100 patients, 20 (0.95%) were diagnosed by means of direct intraoperative evidence of SI during laparoscopic NF between August 1993 and August 2009. The medical records of these 20 cases were prospectively entered in a database, and the data were retrospectively reviewed. We have also outlined our operative technique in floppy NF, management strategy, and the outcome for these patients.
Operative technique
Laparoscopic total fundoplication was performed by using a standard operative technique. All operations were performed by the same experienced surgical team (TI and EE). In brief, a five-trocar technique, with dissection of the esophagus, together with the vagus nerve, was performed. Following the full exposition of the hiatal crura, a nylon tape was passed around the distal esophagus to facilitate the mobilization of the posterior stomach during subsequent maneuvers. A window, of about 5 cm in length, was created behind the lower esophagus, and then, the hiatal crura were approximated by two stitches. Next, the SGVs were divided by using either clips or the LigaSure™ Vessel Sealing System (Valleylab, Boulder, CO). The point on the greater curvature, where the left gastroepiploic artery terminates, was identified, and a window into the lesser sac was made by dividing the SGVs (Fig. 1). Through this window up to the left crura of the esophageal hiatus, complete mobilization of the gastric fundus was performed. A 2-cm floppy 360-degree fundic wrap was created, without a calibration boguie in the esophagus, and secured with two interrupted simple sutures, with only the upper suture passing through the esophageal musculature.
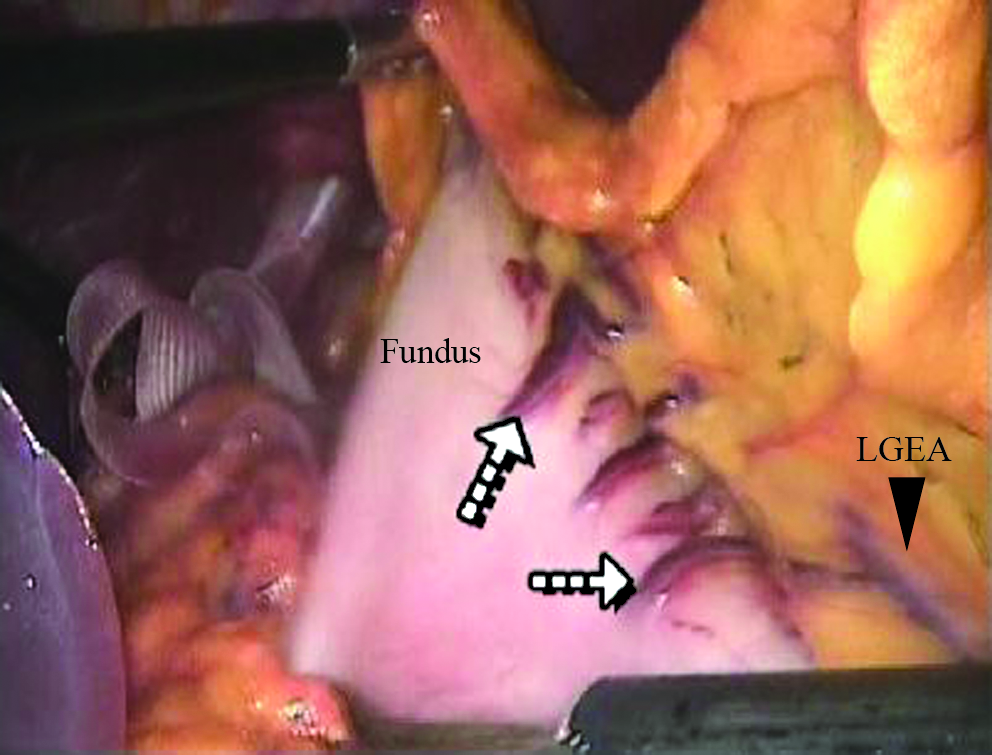
Intraoperative laparoscopic view of the begining point of the dissection on the greater curvature, where the left gastroepiploic artery (LGEA) terminates (upper and lower arrows indicate the short gastric vessels and first branch of the LGEA, respectively).
Evaluation of intraoperative results
The following issues were evaluated: presence of adhesion bands, any significant bleeding, estimated size and location of splenic infarction, and conversion to open technique.
Evaluation of postoperative follow-up
Postoperative symptoms and signs, need for any interventions (i.e., radiologic or surgical), hospital-stay length, morbidity, and mortality were evaluated.
Results
The incidence of SI was 20:2100 (0.95%). SI was demonstrated in 11 women (55%) and 9 men (45%), with a mean age of 35.2 years (range, 25–68).
Intraoperative results
Adhesion bands, due to previous surgery involving upper abdominal quadrants, such as the gallbladder, stomach, and left lobe of the liver, were inspected in 4 (20%) cases; however, none of these were intense bands. There was neither significant intraoperative bleeding nor splenic capsular tears in any cases. The infarcted area was recognized, at the time of surgery, in all cases subsequent to mobilization of the fundus of the stomach. The classic pattern, on laparoscopic examination, was a small area of discrete color changes, suggesting an infarction of less than 10–15% of the total splenic volume, localized mainly in the upper pole, with this being realized in all cases (Fig. 2). There were no conversions to an open technique. Mean operative time was 55.0 minutes (range, 45–95).
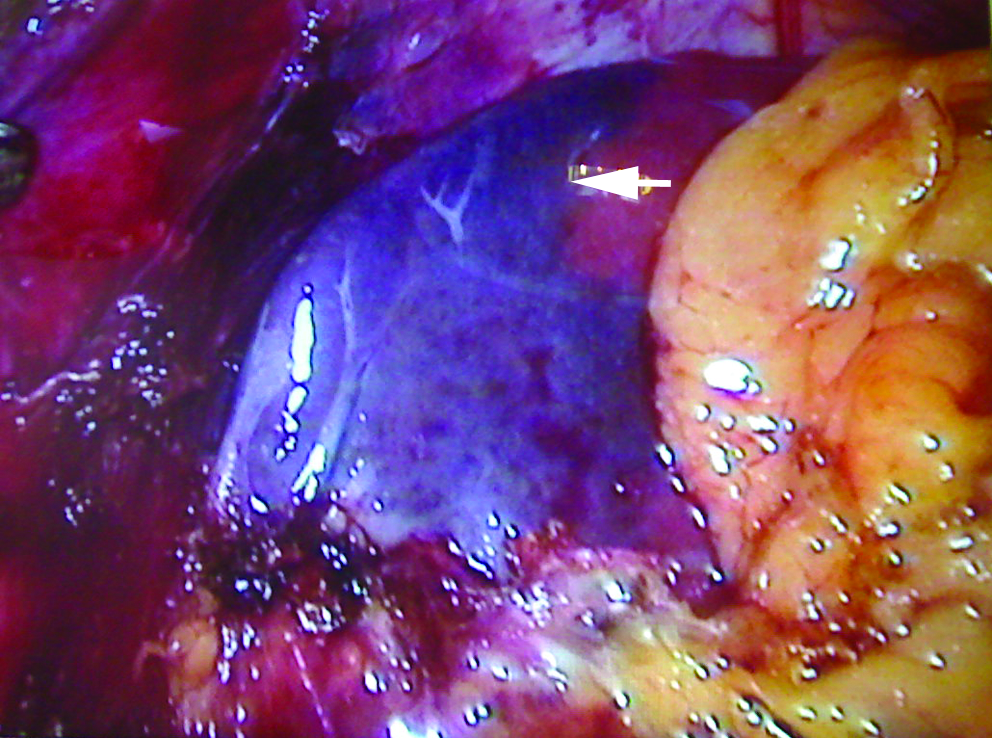
Intraoperative laparoscopic view of a splenic infarction localized in the upper pole (arrow).
Postoperative follow-up
On postoperative day 1, nasogastric tubes were removed, oral fluid intake was started thereafter, and discharge from the hospital was encouraged in all the cases with splenic infarction. Postoperatively, these cases were followed up clinically for 6 months. Abdominal or left-flank pain was the most common symptom, and left-upper quadrant tenderness was the most common sign during postoperative day 1 in all patients. After dicharge, only 2 patients (10%) had persistent left-upper quadrant pain lasting 6–10 days, in which a computed tomography (CT) scan demonstrated the infarcted areas as a low-attenuation wedge of tissue involving less than 15% of the splenic parenchyma (Fig. 3). None of the cases required any further surgical or radiologic intervention. All cases were managed succesfully with observation alone. Mean hospital stay was 1.2 days (range, 1–2). There were neither mortalities nor serious complications during the follow-up period.
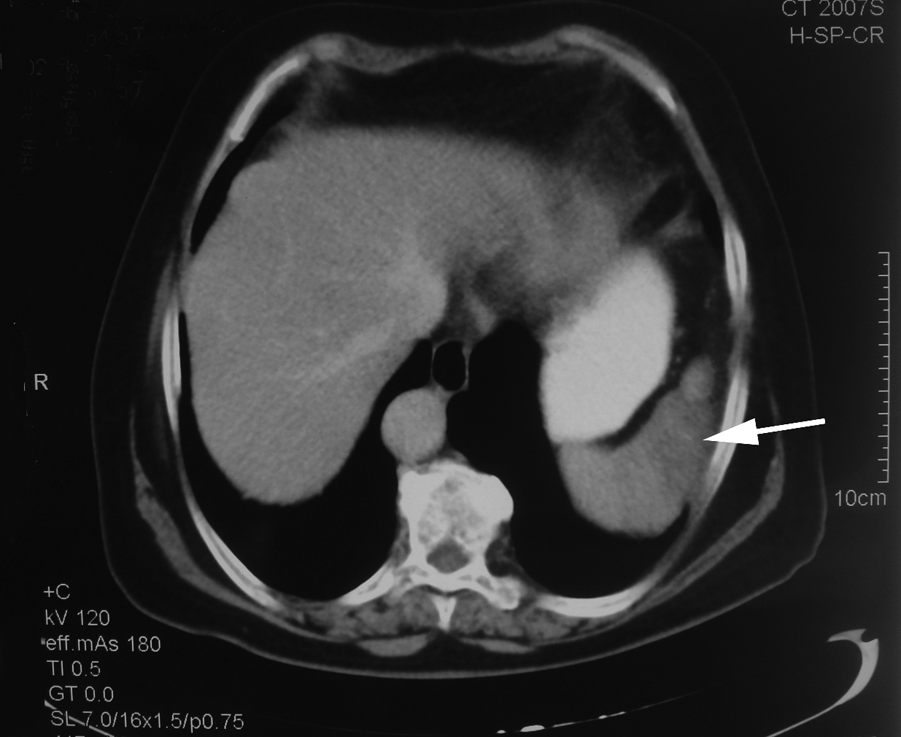
Computed tomography scan of a patient with persistent abdominal pain after laparoscopic floppy Nissen fundoplication, which demonstrated an infarcted area as a wedge of splenic tissue (arrow).
Discussion
The spleen derives most of its blood from the splenic artery, the longest and largest of the three main branches of the celiac artery. It follows a tortuous course posterior to the omental bursa, anterior to the left kidney, and along the superior border of the pancreas. Near the hilus, the artery divides into numerous branches, chief of which are the superior polar, left gastroepiploic, and superior and inferior terminal arteries. The well-developed superior polar artery arises some distance from the hilus and, before entering the spleen, gives off the short gastric arteries to the stomach. The left gastroepiploic artery passes along the inferior pole of the spleen to supply part of the greater curvature of the stomach and greater omentum. The ultimate branches are end-vessels, each of which supplies a wedge-shaped area, the base of which is directed toward the periphery of the spleen. If one of these vessels is plugged, no blood passes directly into the area it supplies, and an infarction results.11,15,18–22
SI is caused by a heterogeneous group of diseases and produces a spectrum of clinical manifestations. According to the previously published series, thromboembolism and malignant or nonmalignant hematologic diseases were the two most common causes. Other causes include the obstruction of the splenic vessels, infiltrative diseases, and vasculitides.22–24 On the other hand, the incidence of SI as a complication of surgery is not well defined. We reviewed the literature, and a total of only 5 such cases were found. A single case of partial SI was reported in a series of 169 laparoscopic adrenelectomies, 25 and the other 4 cases of SI occurred as a complication of laparoscopic NF, during or following the procedure, with the estimated incidence of the clinically significant cases being less than 1%.11,14 Our current data are in line with these previous estimations. We found that 0.9% of our patients who underwent laparoscopic floppy NF developed such a condition. Of particular note, all these complicated cases were diagnosed during the direct laparoscopic evidence of SI. In actuality, we presume that the real incidence is higher, because some cases of SI, if any, without any intraoperative findings, such as discrete color change and postoperative clinical evidence, may have gone undiagnosed.
As a complication of laparoscopic NF, Wilkinson et al. 14 reported 2 cases with radiographic evidence of SI that resulted from a peripheral splenic branch injury. During postoperative follow-up, the first case, with a segmental infarction of the upper pole of the spleen, was managed conservatively, and complete resolution of the infarcted area was demonstrated on the control CT scan. On the other hand, the other patient, who deveoped a persistent superior pole infarction with intense surrounding inflammation on the control CT scan, had to undergo a splenectomy. Both cases did well without sequelae during the follow-up. In a randomized trial in adults who underwent laparoscopic Nissen versus partial fundoplication, an infarction of 75% of the spleen in 1 of 112 patients, following the clipping of a bleeding vessel during the division of the SGVs, was reported. Also, no further surgical intervention was required in this case. 17 Martinez et al. 11 reported an intraoperative discrete color change, with its persistence suggesting ischemia, in the upper splenic pole after SGV division. Consequently, the resulting infarcted area led to the formation of a splenic abscess, which necessitated an open splenectomy. Last, a case of a vanishing spleen, with a fatal consequence, was reported by Dijkman et al. 15 in a pediatric patient who underwent NF, where discoloring of the proximal third of the spleen was noted following the division of SGVs.
In the surgical setting, although the necessity of dividing the SGVs remains controversial, as similar success rates are reported with partial fundoplication without the division of SGVs,8–10 we believe that full mobilization of the gastric fundus is necessary to obtain a loose fundoplication, thereby reducing anatomic and functional dysfunction. This step is a daunting task and should be performed cautiously, as working at this plane of dissection provides limited exposure. With the introduction of new energy-source technology, the LigaSure Vessel Sealing System and the Ultracision Harmonic Scalpel (Ultracision™, Ethicon Endo-Surgery, Cincinnati, OH) offer the possibility of making this process quicker and easier. Despite several trials having reported that the ultrasonic coagulating scalpel was less prone to intraoperative complications and postoperative morbidity,12,13,26 we prefered the use of clips and LigaSure, since they carry a cost advantage to our institution. There was no significant bleeding during SGV division in these 20 cases presented. The occurrence of SI can be explained by possible variations in the vascular anatomy of the spleen.
In general, clinical presentation depends on the natural history of SI. The infarction is usually silent, if it is secondary to the focal ischemia, or it may progress to splenic abscess or massive subcapsular hemorrhage with eventual rupture, if it is secondary to the occlusion of a major splenic vessel.11,24 The population included in our series represents a category of patients where the diagnosis of SI was made during laparoscopic floppy NF, before the onset of symptoms and signs. Considering the results of our study, none of the patients experienced persistent postoperative symptoms, except in 2 cases, where moderate left-upper quadrant abdominal pains, lasting 6–10 days, were reported on follow-up visits. No further attention was given to these events due to the regression of the infarcted areas demonstrated on control CT scans and the gradual resolution of the symptoms.
After diagnosing intraoperative partial SI, we recommend conservative management with close follow-up. If SI causes symptoms that are severe enough to merit further investigation, radiologic studies help identify the clinical course of the infarcted area within the spleen. The classic pattern on a CT scan demonstrates a well-defined hypodense area surrounded by normal-appearing, contrast-enhanced splenic parenchyma. If the infarction gradually involves the entire spleen, the CT scan may fail to demonstrate this classic pattern.14,23,24 Ultrasonography can also be used to differentiate between a hypoechoic acute infarction and a hyperechoic healed lesion and to demonstrate the evolution of the SI into an abscess. 24 When the patient's clinical signs are normal and radiologic studies, if necessary, do not merit any further intervention, conservative therapy, aimed at pain relief alone, is adequate.
Conclusions
Based on the results of the present study, we may conclude that partial SI can be a recognizable condition during laparoscopic floppy NF. Conservative therapy and close follow-up, without any unnecessary intervention, is an appropriate management option that provides a favorable clinical outcome.
Footnotes
Acknowledgments
The authors wish to thank Mr. Paul Hallam for his linguistic assistance.
Disclosure Statement
No competing financial interests exist.
The abstract of this article was presented in the 9th National Endoscopic Laparoscopic Surgery Congress during October 28–31, 2009, in Antalya, Turkey.