
Abstract
Abstract
Background:
Laparoscopic bowel resection for right colonic diseases with peritonitis is technically difficult and time-consuming, particularly in the presence of hard adhesion and dense inflammation. Moreover, peritonitis frequently leads to an emergency operation. Therefore, we evaluated the feasibility and effectiveness of emergency laparoscopic bowel resection in patients with these diseases.
Methods:
During 3 years (November 2006 to October 2009), we enrolled 31 consecutive patients who underwent an emergency laparoscopic bowel resection for right colonic disease with peritonitis. In 2 patients, perforated malignancy was suspected preoperatively, but there was no patient with malignancy at pathologic finding. We analyzed the clinical outcomes, including complications.
Results:
The mean operating time was 140 minutes, and the mean hospital stay was 10 days. There was 1 conversion (3%), and the other intraoperative procedures were uneventful. Four complications (13%) occurred after treatment (1 intra-abdominal abscess, 2 wound abscesses, and 1 adhesive ileus). The intra-abdominal abscess was treated by subsequent percutaneous drainage; the wound abscesses were treated conservatively. One patient with an adhesive ileus 12 months after treatment was managed with a bowel resection. After a median follow-up of 16 months, the other patients had no complications.
Conclusions:
Emergency laparoscopic bowel resection may be a feasible, effective method for the treatment of right colonic diseases with peritonitis.
Introduction
Use of the minimally invasive procedure in patients with right colonic diseases allows for the identification as well as treatment of an unsuspected, causative disease. When these diseases occur with peritonitis, patients commonly undergo an emergency operation. These procedures can frequently be technically difficult, and bowel resection may be necessary at times. In our institution, two surgeons performed an emergency laparoscopic bowel resection in the management of right colonic disease with peritonitis. In the present study, we analyzed the clinical outcomes after laparoscopic bowel resection for 31 consecutive patients with right colonic peritonitis.
Materials and Methods
Between November 2006 and October 2009, a total of 40 patients had suspected right-sided colonic mass with the provisional diagnosis of acute abdomen after radiologic evaluation, and all these patients underwent an emergency laparoscopy. Of these, 31 patients treated with laparoscopic bowel resection were included in the present study. Nine patients treated with minor surgery, such as appendectomy or partial cecectomy or diverticulectomy, were excluded. There was no conversion in laparoscopic minor surgery. Five patients had a history of prior abdominal surgery (3 appendectomies, 1 primary repair for peptic ulcer perforation, and 1 hysterectomy).
During the operation, three ports were employed: an 11-mm camera port (supraumbilical) and two 5-mm ports (left-lower quadrant, LLQ; hypogastric midline) (Fig. 1). The patients were placed in the Trendelenburg position, right-side up. An operator and an assistant stood on the left side of the patient. A mesocolic dissection was performed, with the right hand on the 5-mm LLQ port and the left hand grasping the 5-mm hypogastric midline port. With medial-to-lateral side dissection by the right hand, the pedicle of ileocolic vessels was identified and divided (Fig. 2). Then, we started lateral-to-medial side dissection without a positional change of operator or camera assistant. We performed a paracolic lateral dissection with a laparoscopic hook in the left hand by the 5-mm hypogastric midline port, while grasping forceps with the right hand by the 5-mm LLQ port (Fig. 3). The cecum and appendix were mobilized first, followed by the right colon. If the diseased portion of the bowel was long, mobilization of the hepatic flexure colon was performed. During the procedure, dissection was performed by a change of the hand, according to a convenient surgical plane. After the cecum and ascending colon were separated from the retroperitoneal tissues, duodenum, and pancreatic head, a small midline incision was made by an extension of the umbilical port, and a specimen was extracted. The mean length of midline incision was 5.9 ± 0.7 cm (range, 4.5–8). A stapled bowel anastomosis was performed. All patients were followed-up within 3 weeks of the operation, with a final telephonic review. The clinical outcomes, including complications and recurrent symptoms, were evaluated.
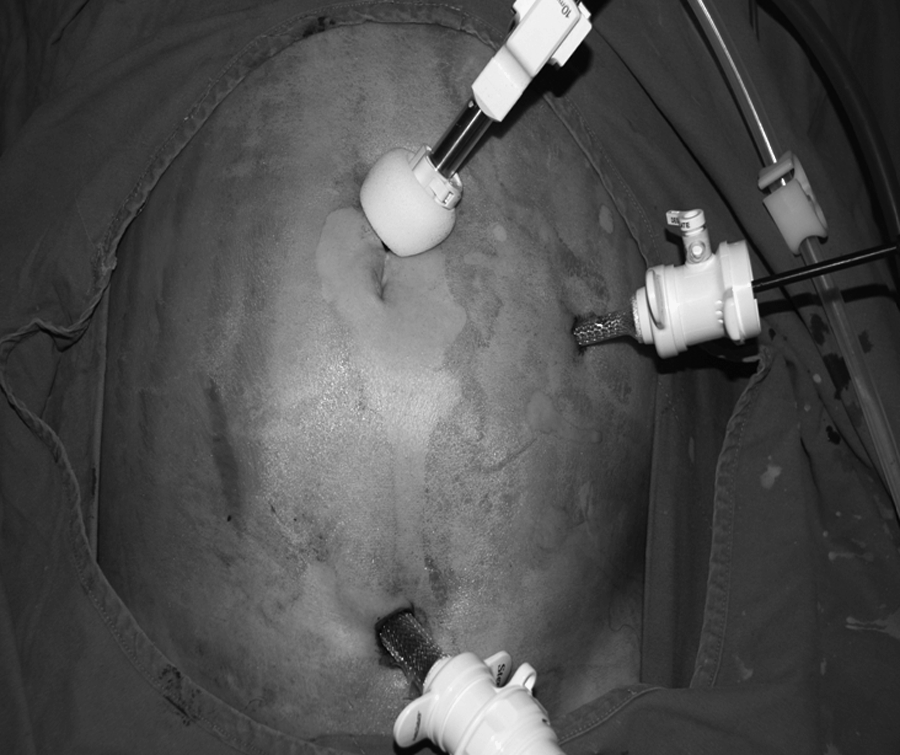
Laparoscopic three-port insertion.
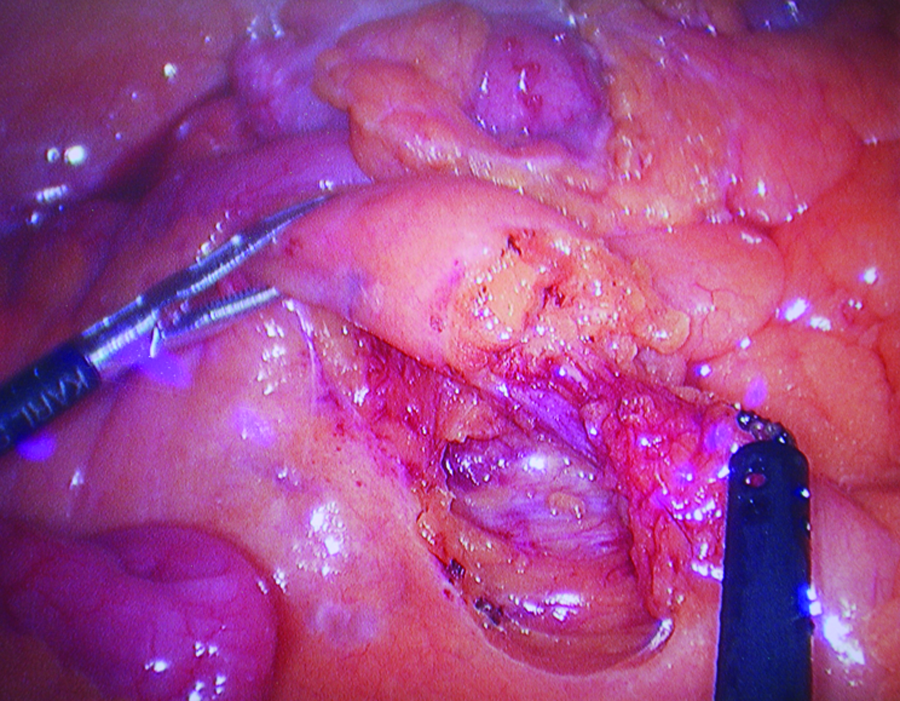
Laparoscopic medial-to-lateral dissection (dissection with right hand, grasping with left hand).
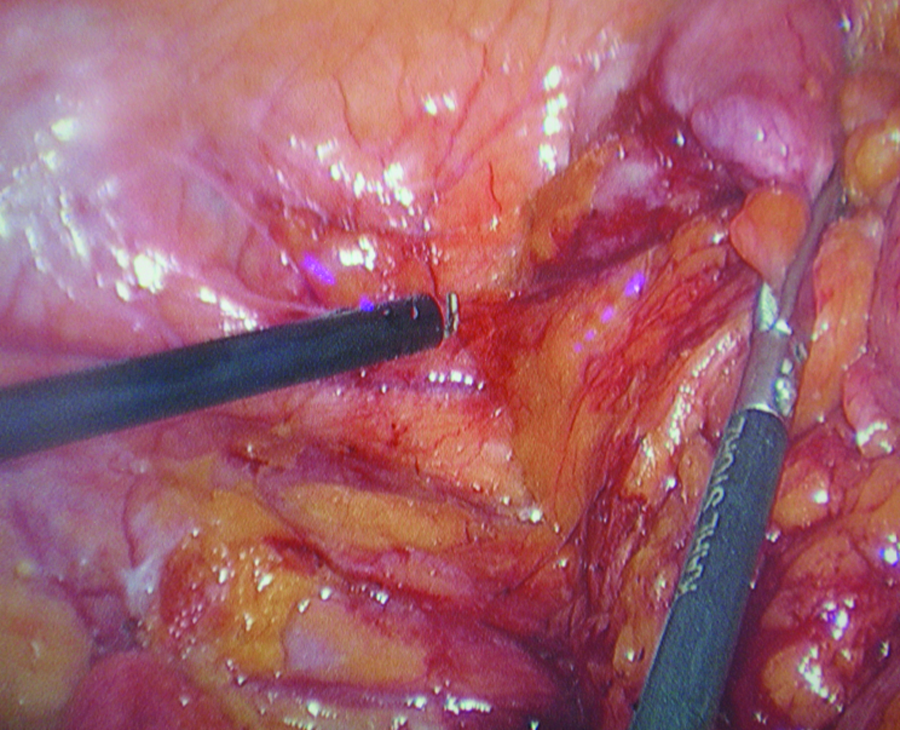
Laparoscopic lateral-to-medial dissection (dissection with left hand, grasping with right hand).
Results
We enrolled 31 patients from prospectively collected data. We performed ileocolic resection in 22 patients and right hemicolectomy in 9 patients. The mean body mass index (BMI) was 22.8 ± 2.8 (range, 16.5–31.2). The diagnosis was based on both clinical and radiologic evidence, including severe abdominal pain with tenderness, rebound tenderness, fever, and leukocytosis. Eighteen patients (58%) presented obstruction symptoms or sepsis. A computed tomography (CT) scan revealed the periappendiceal mass or right-sided pericolic mass formation with peritonitis.
In 31 patients, emergency laparoscopic bowel resection revealed various diseases (Table 1). There were 2 patients in whom malignancy was suspected preoperatively, but none had malignancy in pathologic findings. No patient had protective fecal diversion. In 1 patient, a conversion was necessary to manage massive bleeding from a mass during the procedure. The mass was proven to be intestinal tuberculosis at pathologic finding.
n = 31.
Mean patient age was 44.2 ± 14.8 years, and there were 21 men and 10 women. The mean operating time was 140 ± 21 minutes. In the postoperative period, patients had mean lengths of 4.8 days for resumption of diet, 6 days for antibiotics use, and 10 days of hospital stay (Table 2). Postoperative complications included 1 intra-abdominal abscess, 2 wound abscesses, and 1 adhesive ileus after treatment. There were no other complications, including prolonged ileus or incision hernia. The intra-abdominal abscess was treated by subsequent percutaneous drainage. The wound abscess was treated conservatively. One patient had an adhesive bowel obstruction 12 months after treatment for perforated diverticulitis and was managed with a small bowel resection (Table 3). One patient was admitted for abdominal pain 3 months after treatment of Crohn's disease, but there was no evidence of complication, then was discharged after supportive care. The other patients had no complications after a median follow-up of 16 months.
M/F, male/female; WBC, white blood cell.
Discussion
Other studies have shown that laparoscopic treatment of left-sided colonic diseases can be safely performed, with patients experiencing the benefits of decreased ileus and shorter hospital stay.5–7 Emergency laparoscopic management of left-sided colonic peritonitis has been shown to be a safe and feasible procedure.8–9 Despite good evidence on the benefits of emergency laparoscopy in select patients with peritonitis, use of this procedure varies significantly. In general, emergency operations have been associated with a significantly high likelihood of morbidity and mortality. 10 This finding appears to be based on varied experiences and resultant complications. In addition, some emergency operations may be performed in a setting with limited medical staff and resources. In this study, two surgeons performed emergency laparoscopic surgery for right colonic diseases with peritonitis. Use of emergency laparoscopy for right colonic disease has been studied in a limited number of conditions, such as Crohn's disease, in which laparoscopic management has been successful and has shown more short-term benefits than open surgery.11–13 However, right colonic diseases, including those affecting the appendix, terminal ileum, and cecum, have specific disease entities and can frequently cause acute abdominal pain with peritonitis.
The patients in this study were found to have various right colonic diseases. During the same period, we had 1323 patients who underwent surgical treatment for appendicitis, and 387 (29%) patients had perforated appendicitis. Of these patients with perforated appendicitis, bowel resection was necessary for severe inflammation in the 7 (1.8%) patients. In all of these patients, disease was associated with periappendiceal abscesses.
A total 29 patients were diagnosed with Crohn's disease in the same period. Most patients were treated conservatively, and 7 patients (24%) underwent surgical treatment. Of these, 2 patients underwent emergency laparoscopic ileocolic resection for intra-abdominal abscesses combined with internal fistula (including this study), 2 underwent elective laparoscopic surgery for obstruction, 1 underwent open intra-abdominal abscesses drainage and ileocolic resection, 1 underwent laparoscopic small bowel resection for combined small bowel cancer, and 1 underwent laparoscopic adhesiolysis and stricturoplasty for obstruction. In 1 patient, a large cecal lipoma resulted in obstructing ileocolic intussusception. Laparoscopy revealed bowel ischemia involving a distal ascending colon for chronic colonic obstruction. The patient subsequently underwent a laparoscopic ileocolic resection.
In the same period, we performed 93 elective right colonic resections and 31 emergencies. Of 93 elective operations, we had 89 laparoscopic surgeries, including 6 open conversions, and 4 open surgeries. The patients were 51 men and 42 women, whose ages ranged from 23 to 89 years, with a mean age of 63. The mean BMI was 24.6 ± 3.3 (range, 17–35.2).
In elective operations, 78 had malignant diseases and 15 had benign diseases. There were 5 open conversions in malignancy (2 for severe adhesion in previous abdominal surgery and 3 for suspected adjacent organ invasion, such as duodenum or pancreas) and 1 in benign diseases (adhesive ileus following surgery for perforated appendicitis, severe extensive adhesion between small bowels with retroperitoneum). There were 20 patients with a previous abdominal surgery history (3 gastrectomy, 3 colectomy, 1 small bowel resection, 4 hysterectomy, 1 cholecystectomy, and 8 appendectomy). Postoperative complications were observed in 13 (14%) patients (5 wound abscesses, 3 prolonged ileus, 3 intra-abdominal abscesses, and 2 enterocutaneous fistulae). Intra-abdominal abscesses were successfully managed by percutaneous drainage or antibiotics. Two fistulae were also treated nonoperatively. In 4 open right colonic resections, 1 had a 12-cm-sized large ileocecal mass preoperatively (pathology: lymphoma), 1 had suspected pseudomyxoma peritonei (pathology: perforated mucinous cystadenoma), 1 had large intra-abdominal abscess (pathology: Crohn's disease), and 1 had mucinous cystadenoma, which was diagnosed at the time of gynecologic open surgery for a suspected ovarian tumor. There were no complications in these patients, and BMI values were 26.1, 24.3, 20.6, and 27.6, respectively.
Much less literature on laparoscopic techniques exists on appropriate laparoscopic dissection for right colonic diseases. Laparoscopic medial-to-lateral dissection for right-sided colon cancer has been well examined. Early ligation of vessels and mesocolic dissection along a superior mesenteric vein are important to preserve oncologic principles.14–16 However, benign diseases are not associated with oncologic outcomes, and their clinical presentation often differs from that of malignant diseases. Benign diseases with severe adjacent adhesion and inflammation commonly present technical difficulties for dissection, and thus, relevant methods, using a laparoscopic approach, have not been fully addressed.
Balsara et al. demonstrated the lateral-to-medial approach with laparoscopic-assisted resection for ileocolic tuberculosis. 17 They accessed three ports in almost all patients with tuberculosis. They performed dissection with the right hand through the epigastric port, grasping the left hand through the hypogastric port. This method is useful in laparoscopy for benign diseases, but the operator may be exhausted from handling, and the instruments are prone to interfere with the camera located in the central area.
According to the preference of the laparoscopic surgeon, a convenient approach for dissection may be designed. If the surgeon can use both hands skillfully, the combined approach (i.e., medial-to-lateral and lateral-to-medial) will be feasible and comfortable. Therefore, we performed alternate dissection by using both hands by two surgeons and three ports. Alternate both-sided dissection appears to decrease the manual handling for the less outstretching operator arm and may not be disturbed by the camera located in the umbilical area. In addition, the operator can change the approach, according to accessible plane, considering each operative finding.
Severe phlegmon with abscess in the right-sided colonic area, and the inaccessibility to the retroperitoneal space, can make the disease technically challenging to manage. Retrocolic or retroperitoneal dissection was especially difficult. The dissection was performed carefully and slowly to save important structures; however, this effort may not significantly increase the operating time. We performed laparoscopic bowel resection with a mean operating time of 140 minutes. This finding is comparable to those in other reports, which demonstrated operating times of 75–185 minutes in patients with Crohn's disease. 18
Conclusions
In conclusion, laparoscopic surgery for right-sided colonic diseases with peritonitis, in an emergency situation, can be feasible, with allowable postoperative complications and a comparable operating time.
Footnotes
Disclosure Statement
No competing financial interests exist.