
Abstract
Abstract
Introduction:
The general aim of this report was to determine how a vascular accident (VA) or vascular incident (VI) could be prevented and controlled during thoracoscopic lung lobectomies (TLLs).
Materials and Methods:
Clinical records and videos of patients (n:21) who underwent a programmed TLL during a 3-year period at the Private Children's Hospital “Fundación Hospitalaria” and CEMIC University Hospital (Buenos Aires, Argentina) were reviewed retrospectively. A VA was defined as the accidental bleeding during dissection, depending on the surgeon and/or inflammatory conditions, adhesions, and so on. A VI was defined as the unexpected bleeding after successful vascular sealing, depending on the vascular-sealing device. The conversion criteria to thoracotomy were uncontrollable VA or VI, limited visibility, difficult dissection, and other.
Results:
There were no VA, but there was a 24% rate of VI (n:5). All the VI were arterial, not venous. All the VI were observed in children older than 7 years of age because of deficient sealing. All of them were successfully controlled with LigaSure™ (Valleylab, Boulder, CO) and/or one proximal Hem-o-Lok® clip (Weck Closure Systems, Research Triangle Park, NC) without conversion. Conversion was due to limited visibility (n:2) or difficult dissection (n:2) of the diseased lobe.
Conclusions:
Based on our early experience and a review of the literature, we believe TLL is a feasible and technically reproducible approach that avoids the inherent morbidity of a major thoracotomy incision. Bleeding should not be the main argument to decide in favor of a thoracotomy. LigaSure's reliability would depend on vascular diameter and on patient age. VIs can be prevented in older children by using the sealing device and a proximal Hem-o-Lok clip.
Introduction
Nonetheless, the approach is not routinely performed, in most hospitals. TLL impact on intra- and postoperative morbidity has not yet been fully evaluated. According to the reviewed literature, the most frequent complications are prolonged air leak, infection, pneumothorax, and the need to convert the access in thoracotomy. 4 The risk of intraoperative bleeding discourages many surgeons who would rather perform an open thoracotomy. Unfortunately, there is no sufficient information about how a vascular accident (VA) or vascular incident (VI) could be prevented or controlled thoracoscopically.
At the Private Children's Hospital “Fundación Hospitalaria” and CEMIC University Hospital (Buenos Aires, Argentina), TLL constitutes the procedure of choice for children who require the surgical excision of one or more lobes of diseased lung. The causes of bleeding as well as the most frequent complications associated to TLL were evaluated in our series. The general aim of this report was to determine how a VA or VI could be prevented and controlled. The specific aims of this report were to determine if a VA or VI could be a cause of conversion and which could be the best vessel-sealing method for TLL.
Materials and Methods
Clinical records and videos of patients who underwent a programmed TLL during a 3-year period (2005–2008) at both institutions were reviewed retrospectively. Twenty-one patients were included; there were no contraindications or exclusion criteria for the approach. Data for the following variables were recorded for analysis: age, sex, weight, clinical diagnosis, resected lobe, duration of surgery, duration of chest-tube drainage, VA and reasons, VI and reasons, lobar arterial or venous branch implicated in case of VI, conversion to thoracotomy and reasons, duration of hospital stay, complications, and mortality. Twelve female patients and 9 male patients were operated on. Median age was 2 years (range, 2 days to 12 years). Median weight was 12 kg (range, 3–50). The clinical diagnosis registered was 15 congenital cystic adenomatoid malformations (CCAMs), 4 bronchiectasias, and 2 intralobar sequestrations. The resected lobes were left inferior (n:10), right inferior (n:6), middle (n:2), right superior (n:2), and left superior (n:1).
For the surgical procedure, all the patients were placed in a lateral decubitus position. A selective contralateral bronquial intubation was performed, and a pneumothorax was created by the insufflation of carbon dioxide (flow, 4–6 mL/min; pressure, 5 mm Hg). Three to 4 trocars of 3–12 mm were employed, according to patient requirement. For vascular resection and sealing, LigaSure™ (Valleylab, Boulder, CO) and/or plastic polymeric Hem-o-Lok® (Weck Closure Systems, Research Triangle Park, NC) clips were used. For bronchial closure, Hem-o-lok clips and/or an Endo-GIA II® (Ethicon Endo-Surgery, Cincinatti, OH) mechanical suture were used. Resected lung specimens were removed from the thorax through a 2–3-cm-long incision, using one of the existing trocar wounds. A chest tube was left in all cases.
A VA was defined as the accidental bleeding during dissection, depending on the surgeon and/or inflammatory conditions, adhesions, and so on. A VI was defined as the unexpected bleeding after successful vascular sealing, depending on the vascular-sealing device. The conversion criteria to thoracotomy were uncontrollable VA or VI, limited visibility of the diseased lobe, difficulty to dissect the corresponding anatomic structure, and other.
Results
Median surgical time was 168 minutes (range, 60–270). Median chest-tube drainage time was 4.7 days (range, 2–10). Median hospital stay was 12.65 days (range, 3–29). There were no VA. There was a 23.8% of VI (n:5). All VIs were arterial, not venous. All VIs were observed in children older than 7 years of age because of deficient sealing. The implicated arteries were 3 basal branches of the right inferior lobe and 2 basal branches of the left inferior lobe. All VIs were successfully controlled with LigaSure and/or one proximal Hem-o-Lok clip by TLL (Table 1). Four trocars were used in each case. The VIs were not a cause of conversion. The washing and aspiration of blood were essential for this maneuver, since they facilitated the visibility and control of the VI.
LigaSure™ was from Valleylab (Boulder, CO), and Hem-o-Lok® clips were from Weck Closure Systems (Research Triangle Park, NC).
BBRIL, basal branch of right inferior lobe; BBLIL, basal branch of left inferior lobe.
Eighty-one percent of the patients were solved by TLL (n:17). Four patients were converted. Two cases belonged to patients with CCAM; both were converted due to limited visibility of the diseased lung lobe. The next case corresponded to a patient with a past history of repetitive pneumonia and infected CCAM. The presence of abundant chronic perihilar tissue made dissection and visualization of the anatomic structures difficult. The last case corresponded to a patient with bronchiectasias in the right inferior lobe and multiple, large hilar adenopathies, which made dissection difficult. One of the patients required an intrasurgical blood transfusion, although he did not have hemodynamic compromise. The complications registered during hospital stay were subcutaneous emphysema (n:1), chylothorax (n:1), and pneumothorax (n:4), which resolved spontaneously. After hospital discharge, a patient presented with temporary paresia of the diaphragm, which resolved spontaneously in 6 months. Despite this high complication rate, there were no deaths. Moreover, none were related to a VI.
Discussion
Achieving hemostasis may sometimes be challenging, especially in TLL. Options for effective techniques for vessel sealing in pediatrics are limited because of the size and restricted intracorporeal space of most patients. LigaSure is a novel instrument, with widespread use, in many surgical disciplines,5–7 consisting of a bipolar radio-frequency generator and a 5-mm laparoscopic Maryland-style grasper dissector. It uses heat energy to denature collagen and elastin, thus achieving reliable sealing with minimal sticking, charring, and lateral thermal spread. It is associated with a decrease in blood loss and operating time. 8
The system, however, only achieves perfect sealing in pulmonary vessels less than 7 mm in diameter (Fig. 1). 9 We observed, in our series, that the dehiscense rate was increased in arteries with diameters larger than 7 mm. Also, we observed that the dehiscense rate was increased in patients older than 7 years of age. According to our experience and despite Ligasures sealing limitation, hemostasis could be safely achieved in vessels with diameters larger than 7 mm and in children older than 7 years of age. We specifically recommend the use of the sealing device and one proximal Hem-o-Lok clip to prevent and control VIs in all these cases (Fig. 2). Thereby, bleeding should, consequently, not be the main argument to decide in favor of a thoracotomy. Ligasures reliability would depend on vascular diameter and on patient age. We designed a rubber-artery model to compare diameters before and after the use of the 5-mm laparoscopic Maryland-style grasper dissector (Fig. 3) and to understand why this was so. Further studies are needed, nonetheless, to confirm in what degree the vascular diameter is directly vinculated to patient age.
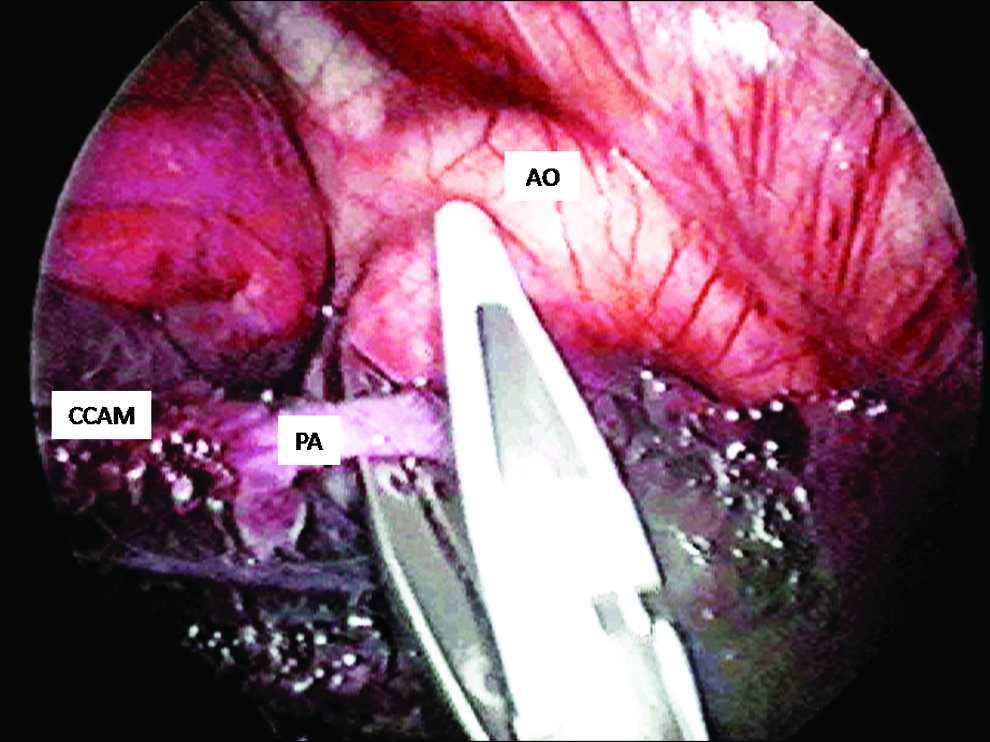
Lobectomy in a young patient. Note the diameter of the pulmonary artery, in comparison to the LigaSure™ (Valleylab, Boulder, CO) tip. In this case, no clips were needed and no VIs were observed. AO, aorta, PA, pulmonary artery; CCAM, cystic adenomatoid malformation.
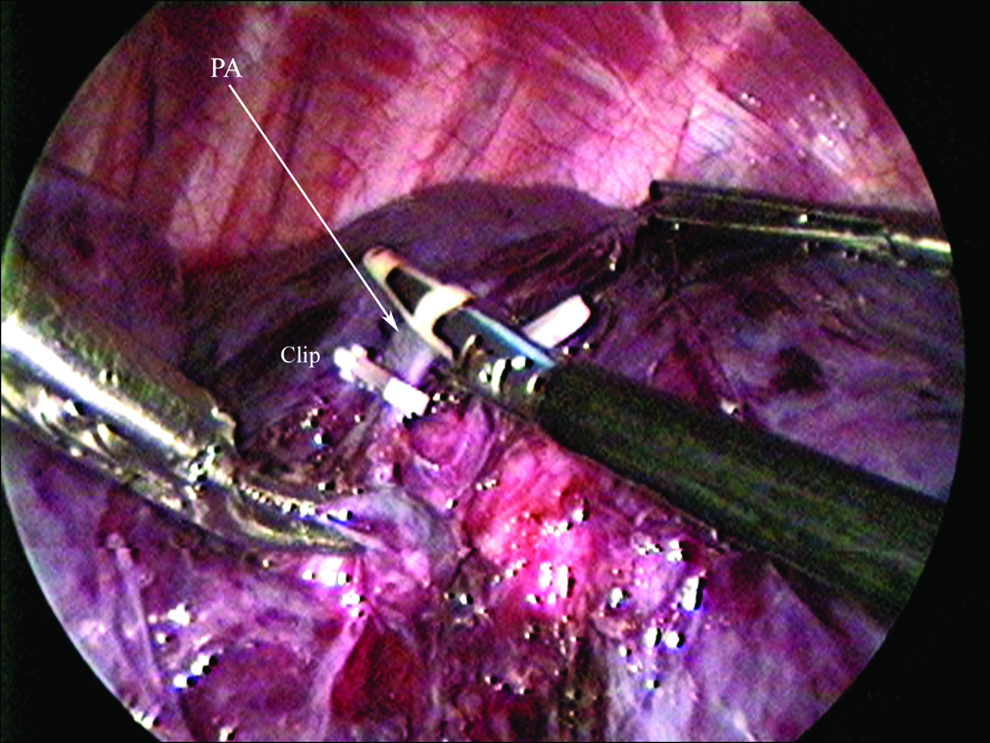
Vascular approach in a patient older than 7 years. Note the diameter of the pulmonary artery (arrow-PA) that covers almost the whole LigaSure™ (Valleylab, Boulder, CO) tip. In this case, a proximal Hem-o-Lok® clip (Weck Closure Systems, Research Triangle Park, NC) was applied. PA, pulmonary artery; Clip, proximal Hem-o-Lok clip.
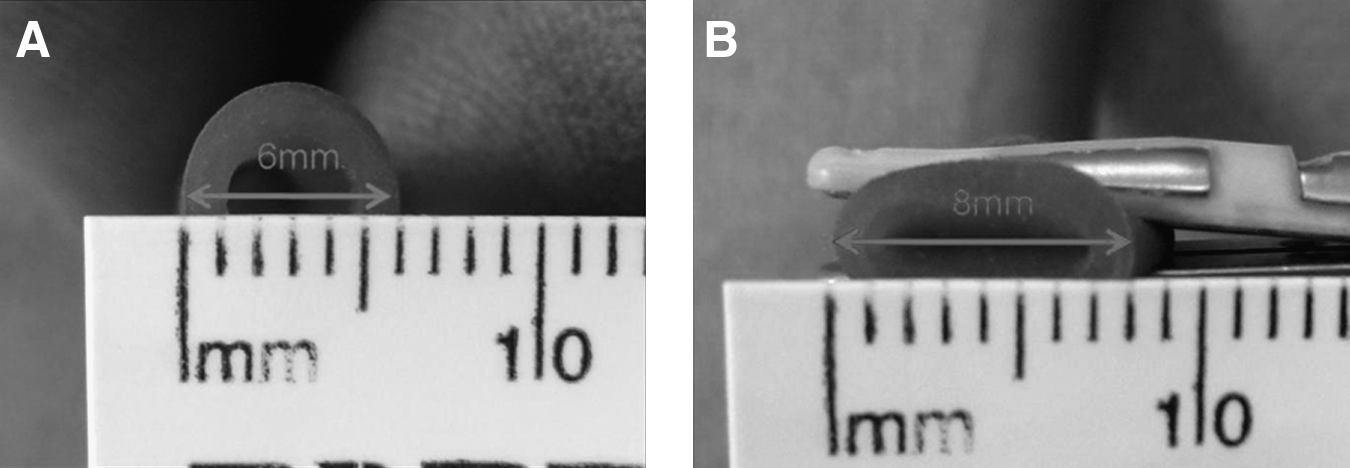
Rubber-artery model where diameters are compared before (
It is important to point out, also, that neither a VA nor a VI were a cause of conversion in our series. In fact, 2 patients were converted because of limited visibility and 2 other patients were converted because of difficult dissection. Just like Vu et al., we noted that TLL is challenging in patients with a history of pneumonia as well as a risk factor for conversion to thoracotomy. 10 Our results compare favorably with those reported by others.4,11,12 We relate our high complication rate to the learning curve (it has been our first series of patients operated on by TLL). The prolonged hospital stay was due, most probably, to the fact that 1) the majority of patients were neonates (some of them had associated congenital malformations) or infants smaller than 1 year of age and 2) the institution's clinical management policy.
Conclusions
In conclusion, TLL, when using LigaSure, appears technically feasible and reproducible, producing satisfactory preliminary results in patients with vascular diameters less than 7 mm and younger than 7 years of age. VI can be prevented in older children by using the sealing device and a proximal Hem-o-Lok clip. Further studies are required to confirm Ligasures sealing strength and reliability as well as the complications inherent to the technology and TLL.
Footnotes
Acknowledgments
The authors thank Carolina Millán (attending surgeon) and Giselle Corti (biologist) for their academic and editorial collaboration.
Disclosure Statement
No competing financial interests exist.