
Abstract
Abstract
A 65-year-old female suffered from recurrent urinary tract infection and intermittent right-flank soreness when active. Serial renal ultrasonography and supine/erect intravenous (i.v.) pyelography work-up revealed a floating right kidney with a descent of two vertebral bodies. A Laparoendoscopic single-site retroperitoneal nephropexy was performed. A homemade single port was created by using a commercially available wound retractor through a 3-cm incision at the tip of the 12th rib. With conventional 5-mm laparoscopy and instruments, a retroperitoneal nephropexy was perfomed. The procedure was completed successfully without any complication and with minimal blood loss. The total operative time was 110 minutes. The postoperative course was uneventful. The follow-up erect i.v. pyelographies revealed a normal right kidney position without descent. Laparoendoscopic single-site retroperitoneal nephropexy was a safe, effective procedure, according to our initial experience.
Introduction
Patients and Methods
A 65-year-old female presented with a recurrent urinary tract infection and intermittent right-flank soreness when active. She was a slim woman with a BMI (body mass index) of 21 without any palpable abdominal mass or knocking tenderness. The flank soreness was usually exacerbated by the upright position and relieved by recumbence. Serial renal ultrasonographies revealed intermittent right-side hydronephrosis. Thus, a floating right kidney with symptoms was highly suspected. Then, supine/erect intravenous (i.v.) pyelography was performed and revealed the downward displacement of two vertebral bodies of the right kidney on the erect position (Fig. 1). Due to refractory intermittent right-flank soreness while under oral-form analgesics for more than 3 months, a laparoendoscopic single-site retroperitoneal nephropexy for floating right kidney was suggested and consented.
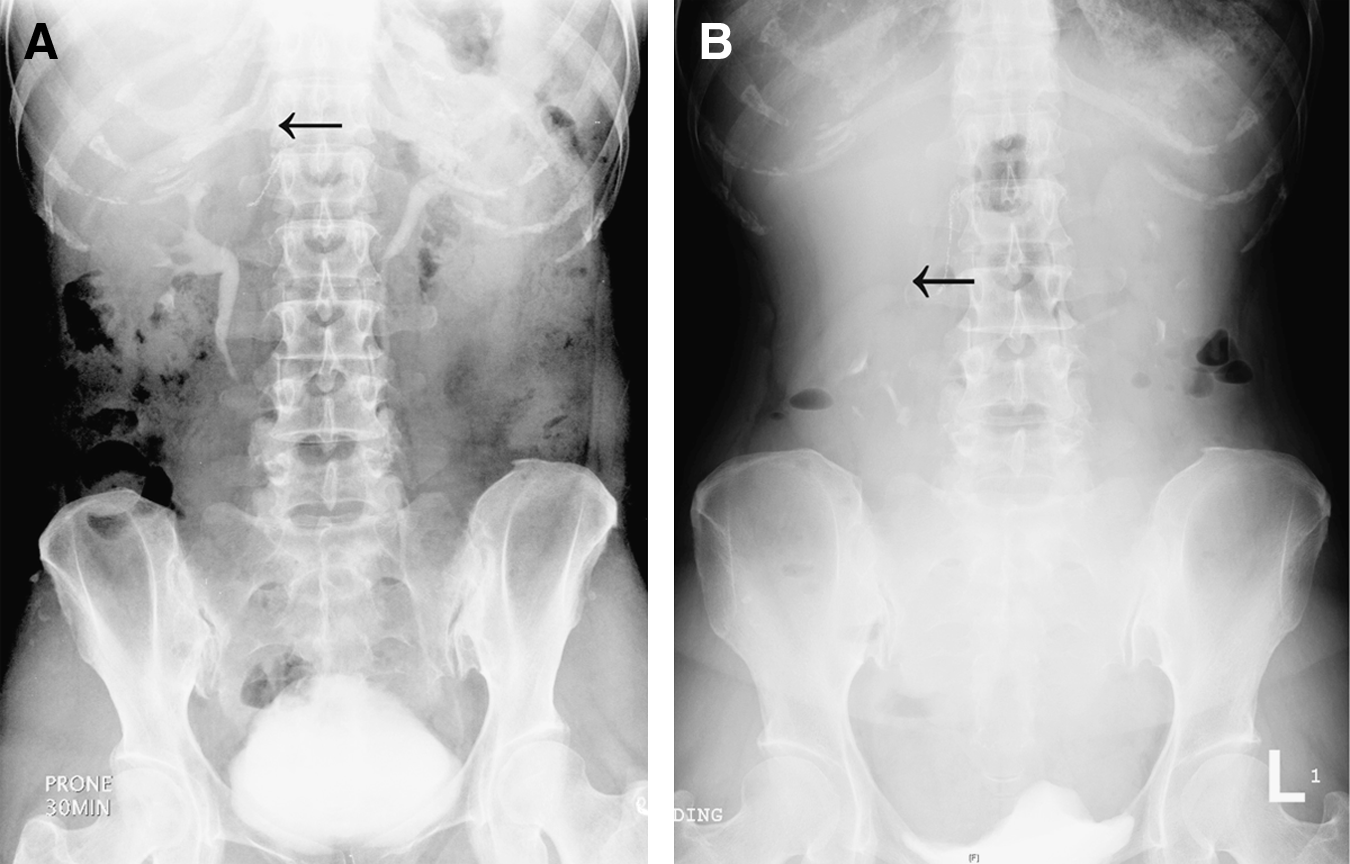
Erect intravenous (i.v.) pyelography in (
Operative technique
Under endotracheal general anesthesia, the patient was placed in a right-flank position. Then, a 2.5-cm incision was made beneath the tip of the 12th rib. The subcutaneous tissues and fascia were dissected sharply. With blunt-finger dissection, the retroperitoneal space was created for the single-port placement. An Alexis® wound retractor (Xsmall; Applied Medical, Rancho Santa Margarita, CA) was placed in position through the incision, with the bottom ring (green) inside the abdomen. A pair of sterile surgical gloves was snapped onto the external ring (white), and the upper half parts (including the five fingers) of the gloves were ligated and truncated. A 5-mm laparoscopic standard trocar was then inserted through the gloves and secured by a purse-string suture around the trocar. After the pnemoretroperitoneum was established, a rigid 5-mm 30-degree laparoscope was inserted to inspect the retroperitoneal cavity. Then, two additional 5-mm operating trocars were inserted with the same procedure (Fig. 2). Standard straight laparoscopic instruments were used for subsequent manipulation. The Gerota's fascia was entered, and the space surrounding the posterior renal capsule was created with blunt dissection. The posterior and lateral capsule of the kidney, and part of the anterior renal capsule, was separated from the retroperitoneal attachments by blunt, sharp dissection. Then, two 2-0 Monocryl sutures was delivered into the retroperitoneal space by directly puncturing the surgical gloves that snapped onto the wound retractor. Two twice-running stitches were made over the lower pole and midportion of the kidney. Each running stitch was attached with one 1 × 2 cm2 mesh to enhance postoperative adhesions between the floating kidney and the surrounding muscles (Fig. 3). Then, the needles were detached and removed through working ports. The two sets of stitches were delivered out of the body through the whole muscle layer of the back with an endoclosure via a tiny skin-stabbing wound at the level of the 2nd lumbar vertebra lateral to the sacrospinalis muscles. Finally, these stiches were fastened subcutaneously.

An Alexis® (Xsmall; Applied Medical, Rancho Santa Margarita, CA) wound-retractor–based multichannel homemade single port, including three 5-mm standard trocars secured on the gloves snapped onto the external ring of the wound retractor.
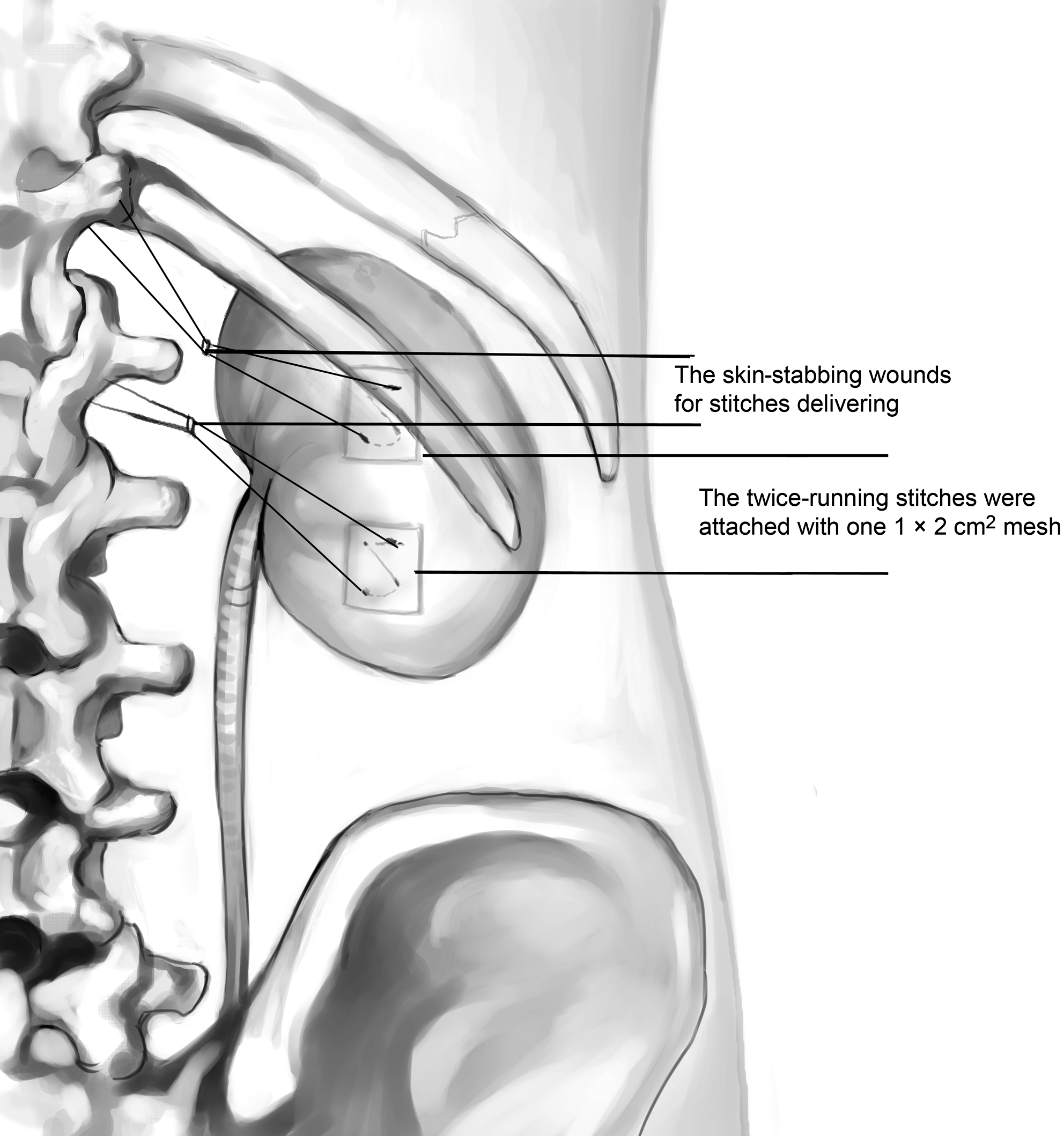
Each twice-running stitch made over the lower pole and midportion of the floating kidney was attached with one 1 × 2 cm2 mesh to enhance postoperative adhesion. The two sets of stitches were delivered out of the body separately via a tiny skin-stabbing wound at the level of the 2nd lumbar vertebra lateral to the sacrospinalis muscles.
Results
The operative time was 110 minutes (including time for single-port creation: 30 minutes). Postoperative recovery was uneventful. There was no intra- or postoperative complication. The patient started oral intake on postoperative day 1 and was discharged on postoperative day 4. The postoperative pain was rapidly relieved by on-demand oral analgesics.
The renal ptosis-related symptoms completely resolved during the outpatient follow-up. The follow-up i.v. pyelography study 3 months after procedure revealed that the treated kidney was in the desired position and axis, with a standing descent less than one vertebral body. The preoperative intermittent hydronephrosis noted by ultrasonographies resolved completely after the procedure. The cosmetic results were excellent (Fig. 4).
Postoperative photograph at 3 months following laparoendoscopic single-site retroperitoneal nephropexy.
Discussion
The floating kidney has been proven to be an actual renal pathology and the benefits of several types of laparoscopic nephropexy have been proven to be safe and effective for the symptomatic floating kidney.1,2 The recent revolution of a novel surgical technique, collectively known as LESS, has been successfully introduced in a wide variety of urologic procedures. 3 The LESS procedure has been successfully and safely performed in varicocelectomy, orchidopexy, prostatectomy, pyeloplasty, nephrectomy, and adrenalectomy. To our knowledge, this is the first reported laparoendoscopic single-site nephropexy for the floating kidney in the literature.
Several challenges should be conquered before the LESS procedure is started. The first challenge is to create a multiple-access platform through a single skin incision without compromising the pneumoperitoneum. Several types of ports are currently commercially available: the Triport and QuadPort (Advanced Surgical Concepts, Bray, Ireland); the Uni-X single-port access laparoscopic system (Pnavel Systems, Cleveland, OH), and the SILS port (Covidien, Mansfield, MA). However, these specialized ports were less durable and flexible than the standard laparoscopic trocar ports. 4 In addition, these commercially available single ports were not globally available, including in Taiwan. Hence, we created our homemade single port with multiple-access channels by securing several standard laparoscopic ports onto this homemade port. 5 Our homemade single-port merits the following characteristics: 1) It is more cost-effective than present single-port entry systems (US$150); 2) it is highly flexible for its freedom in choice of trocar sizes and trocar-position arrangement; 3) by using the larger trocar (10- or 12-mm), the mesh or needle is delivered into the abdomen without difficulty; and 4) it is a durable LESS platform, even in procedures requiring long operative times (i.e., up to 6 hours). 5
Another challenge is the loss of instrument triangulation when performing the LESS procedure. Newer articulating instruments offer a better resolution to the aforementioned problems. However, crossing manipulation of these articulating instruments is counterintuitive, and the learning curve does exist before the mastering of these newer instruments is achieved. In addition, these articulating instruments are structurally less durable than standard laparoscopic instruments, especially in tissue retraction. Hence, the LESS instruments should be designed more intuitively in handling and more reliably in tissue retraction. 4
Besides, the parallel arrangement of instruments usually leads to “sword fighting” of standard laparoscopic instruments not only inside, but also outside the abdomen. We had performed more than 80 urologic LESS procedures with the same LESS platform (i.e., homemade single-port 30-degree endoscopy and standard laparoscopic instruments). After gaining experience with different LESS procedures, the instrument triangulation and clashing problems now rarely impede our LESS procedure by using standard laparoscopic instruments without any ancillary ports. Because the position of the instrument for tissue traction and the instrument for tissue dissection could usually be placed in two different positions or directions, this would keep these instruments from clashing with each other. The only exceptions are the suturing and knot-tying techniques, which usually require an adequate instrument triangulation. Actually, these procedures could be overcome by a curved-tipped standard instrument and/or an extracorporeal knot-tying technique, such as that we had used in LESS nephropexy. Although the aforementioned LESS techniques require more time to learn and practice, it is possible to perform the LESS procedure with standard laparoscopic instruments.
Our LESS retroperitoneal nephropexy techniques have the following merits. With the current LESS technique, the cosmetic and surgical outcomes were maximized without compromising the efficacy of surgery (i.e., comparable operative time with laparoscopic nephropexy). Our LESS platform was cost-effective by using the homemade single-port and standard laparoscopic instruments. With the currently described LESS technique, further expenses on newer articulating instruments and flexible endoscopic systems were rarely necessary when a standard laparoscopic system and instruments are already available.
Conclusions
In conclusion, our initial experience revealed that LESS retroperitoneal nephropexy was a safe, effective and cost-effective procedure for symptomatic floating kidney with improved cosmetic results.
Footnotes
Disclosure Statement
No competing financial interests exist.