
Abstract
Abstract
Objectives:
To evaluate the feasibility, safety, and patients' satisfaction of laparoendoscopic single-site surgery (LESS) with a 2-mm miniport using a standard trocar and instruments.
Methods:
Between November 2008 and October 2009, we performed LESS for benign gynecologic conditions with a 2-mm miniport in 61 patients. Only 1 case was converted to conventional laparoscopic surgery using three ports to perform an appendectomy. The level of satisfaction of the patients was surveyed with five scales (“very satisfied,” “satisfied,” “not sure,” “unsatisfied,” and “very unsatisfied”).
Results:
The mean operative time was 46.6 ± 20.7 minutes, and the mean blood loss was 8.9 ± 7.4 mL. The length of the hospital stay postoperatively averaged 1.8 ± 0.9 days. No complications that required treatment occurred. Among 60 patients, 52 patients (87%) responded to the survey. Thirteen patients (25%) were “very satisfied,” 29 patients (56%) were “satisfied,” 8 patients (15%) were “not sure,” and 2 patients (4%) were “unsatisfied.” Forty-two patients (81%) had a positive perception of the surgery. Forty-nine patients (94%) responded that they were satisfied with the cosmetic outcome.
Conclusion:
LESS with a 2-mm miniport is a feasible and safe treatment modality for benign gynecologic diseases without incurring additional costs. Moreover, the cosmetic results were excellent.
Introduction
Materials and Methods
Between November 2008 and October 2009, we performed LESS with a 2-mm miniport for benign gynecologic conditions on 61 patients in the Department of Gynecology at Kyungpook National University Hospital in Daegu, Korea. The Institutional Review Board of our hospital approved this study. Each patient underwent a physical examination, routine laboratory evaluation, and pelvic ultrasound. Only 1 case was converted to conventional laparoscopic surgery using three ports to perform an appendectomy for a mucinous cystadenoma of the appendix. Except for this 1 case, all 60 cases were analyzed based on the following parameters: age, body mass index, operative time, blood loss, change in hemoglobin level, and length of hospital stay postoperatively. The level of satisfaction of the patients was surveyed over the phone on agreement by the same clinician (G.O.C.). To reduce bias, the survey was anonymously performed. All operations were performed by 1 surgeon (Y.S.L.).
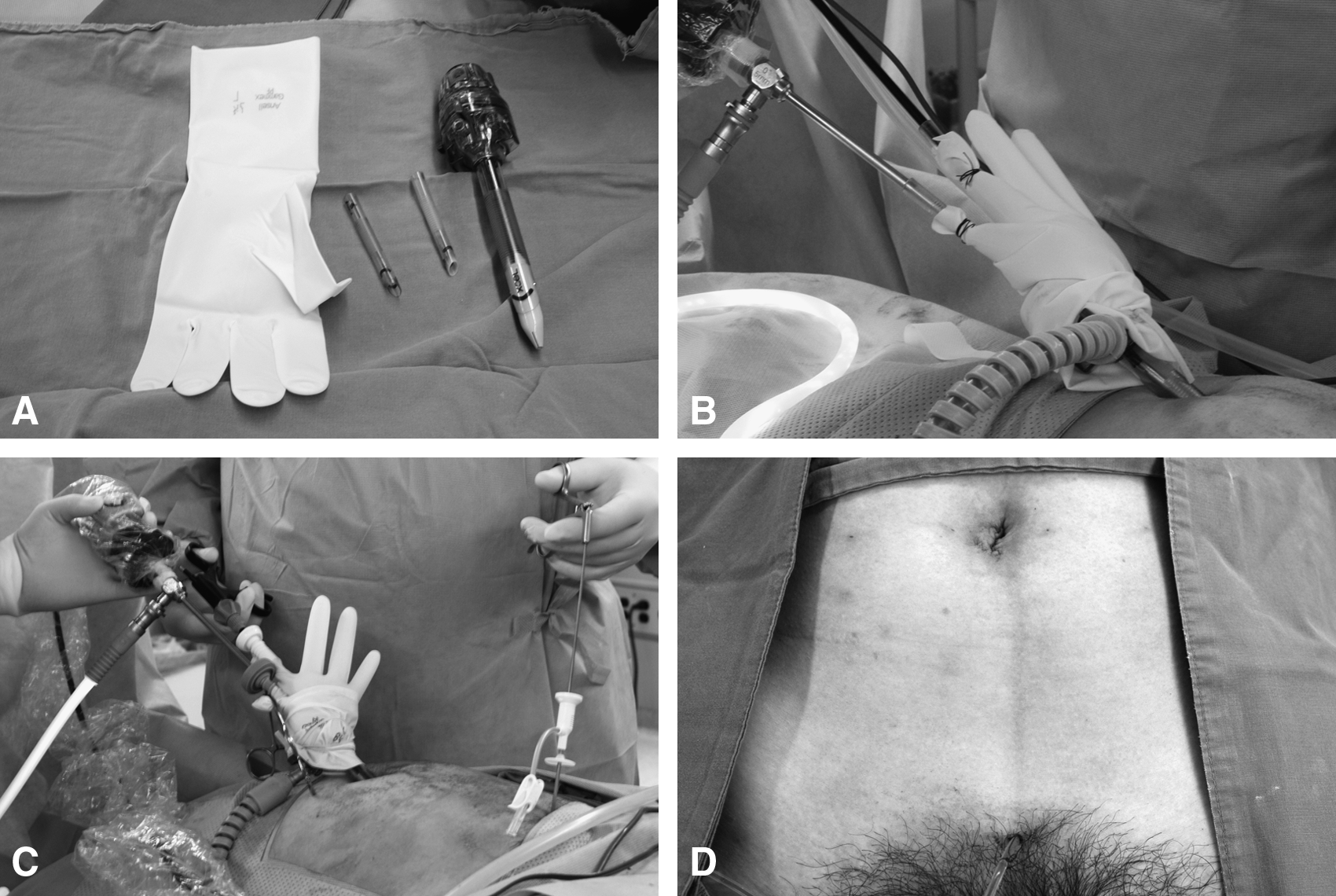
The surgical process was as follows. Under endotracheal general anesthesia, the patients were placed in the dorsolithotomy position after the placement of a uterine manipulator. Using a standard 12-mm trocar, the primary trocar was directly inserted through the umbilicus. A rigid, zero-degree, 5-mm laparoscope (Stryker®, San Jose, CA) was inserted through the trocar to inspect the peritoneal cavity. When an endobag (LapBag; Sejong Medical, Seoul, Korea) was required, the endobag was blindly placed around the lesion inside the pelvic cavity through the 12-mm trocar site with the end of the thread outside of the cannula sleeve. To prevent leakage of carbon dioxide, a surgical grove was fixed on the 12-mm trocar. To insert a 5-mm laparoscope and 5-mm standard laparoscopic instruments, two slim pipes were attached to the first and second finger positions of the surgical grove. Two slim pipes were made from a tip of 5-mm trocar (Fig. 1A–C). The purpose of attaching these two pipes was to prevent clashing between the laparoscope and instruments and to serve as two working channels. To facilitate entrance of a laparoscope and 5-mm instruments, we did not remove the top cap of the 12-mm trocar. First, a 5-mm laparoscope was inserted one-half of the length of the trocar. As we checked the direction of insertion of the 5-mm instrument, the laparoscope was fully inserted. In the suprapubic area, a 2-mm miniport (MiniPort™ Auto-Suture™; USSC, Norwalk, CT) was inserted without a skin incision, and a 2-mm grasping forceps (Auto-Suture) was introduced. Coagulation and dissection were performed using 5-mm instruments introduced through the umbilicus. To maintain triangulation, we used a 2-mm grasping forceps introduced through the suprapubic miniport. Cystectomies, salpingo-oophorectomies, and hysterectomies were similar to the procedures performed during three- or four-port laparoscopic surgery. We performed colpotomies to extract specimens in two hysterectomies and in 1 case involving the extirpation of an 11 × 8 cm mature cystic teratoma. For the other cases, the specimens were extracted through the umbilicus with or without an endobag. After surgery, drainage was placed in the cul-de-sac through the 2-mm miniport site, if necessary (Fig. 1D). The peritoneum and fascia of the umbilicus were closed using 2-0 Vicryl, and the skin was closed using Histoacryl® (B-Brown, Tuttllngen, Germany; Fig. 1D). The 2-mm miniport site was closed using Steri-Strips™ (3M Health Care, Neuss, Germany) without suture after removing the drain.
(
Results
The mean age of the patients was 39.0 ± 12.5 years, and the mean body mass index was 22.0 ± 2.5 kg/m2. There were 15 patients (25%) who had previously undergone abdominal surgery. The main operative procedure was an ovarian cystectomy (n = 34), followed by oophorectomy (n = 21), salpingectomy (n = 3), and hysterectomy (n = 2; Table 1). The mean operating time was 46.6 ± 20.7 minutes, and the mean blood loss was 8.9 ± 7.4 mL. The mean postoperative changes in the hemoglobin level were 1.6 ± 0.7 g/dL, and the length of hospital stay postoperatively averaged 1.8 ± 0.9 days. The postoperative recovery was uneventful in all of the patients. The histologic findings were as follows: mature cystic teratoma (n = 33), mucinous cystadenoma (n = 9), serous cystadenoma (n = 6), endometrioma (n = 6), paratubal cyst (n = 3), myoma (n = 2), and paraovarian cyst (n = 1; Table 2).
Data are presented as mean ± standard deviation or as a percentage of the total number.
Data are presented as mean ± standard deviation or as a percentage of the total number.
Twelve cases of appendectomies were performed using an Endoloop ligature (Endoloop Ligature PDS II; Ethicon, Summerville, NJ) due to suspected appendicitis. The mean operative time was 7.9 ± 3.7 minutes, and there was no blood loss.
The level of satisfaction of the patients was surveyed with five scales (“very satisfied,” “satisfied,” “not sure,” “unsatisfied,” and “very unsatisfied”). Among the 60 patients, 52 (87%) responded to the survey. Thirteen patients (25%) were “very satisfied,” 29 patients (56%) were “satisfied,” 8 patients (15%) were “not sure,” and 2 patients (4%) were “unsatisfied.” Forty-two patients (81%) had a positive perception of the surgery. Forty-nine patients (94%) were satisfied with the cosmetic outcome, 41 patients (79%) thought that this operation contributes to minimize postoperative pain, 41 patients (79%) considered the length of hospital stay to be short, and 43 patients (83%) would recommend this procedure to other family members.
Discussion
Wheeless 5 performed the first single incision laparoscopic tubal ligation through the umbilicus in 1969. Since then, many gynecologists have performed laparoscopic tubal ligation via a single umbilical incision. In this manner, gynecologists have been familiar with LESS since the 1970s. However, the further development of LESS has been insignificant until now. Kosumi et al. 6 reported an ovarian cystectomy through the umbilicus in a 2-month-old baby, and Ghezzi et al. 7 performed a salpingectomy after retracting a percutaneous sling suturing of the affected tube to treat an ectopic pregnancy. The primary reasons for LESS remaining underdeveloped are technical problems. However, new instruments, such as multilumen ports and bent or flexible instruments, have been recently developed. Many early clinical results have been reported in the fields of urology and surgery.8–10 However, multilumen ports and bent or flexible instruments require additional costs, which will create a financial burden to the patients and/or hospitals. Moreover, bent or flexible instruments require the acquisition of new skills by the surgeons and may lead to intraoperative complications, as they have different angles compared with the conventional rigid instruments. We performed LESS as described herein using a standard 12-mm trocar and rigid instruments without additional costs or a learning period of bent or flexible instruments.
No one would argue that one incision is better than multiple incisions. However, it should be recognized that the incision is not the 10 mm incision traditionally used in laparoscopic surgery; rather, it is a 2–3 cm incision for a multilumen port, such as an R-port or Uni-X. Kadar et al. 11 demonstrated that the frequency of incisional hernias was significantly higher for 12-mm than 10-mm trocars (P = 0.01). Although the frequency of incisional hernias with a 20-mm trocar site has not been reported, it is expected to have a higher incidence compared with standard 12-mm trocars. In addition, larger port site sizes may increase surgical morbidity, such as bleeding or internal organ damage, and may decrease the cosmetic outcome. It is our opinion that 12- and 2-mm port sites may be superior to 20-mm one-port surgery in cosmetic outcome, because the 2-mm trocar site does not leave a scar after surgery. Further, it is conceivable that our surgical procedure may have fewer complications, such as incisional hernias or bleeding, compared with a 2–3 cm incision.
Since the laparoscope and rigid instrument were introduced through one 12-mm trocar site, clashing of the laparoscope and instruments was common. To prevent this, 5-mm slim pipes were used, and the assistant adjusted the direction of the laparoscope according to the operator's instrument movements. When working through a single port, there may be loss of triangulation; however, traction is gained by the grasping forceps introduced from the suprapubic 2-mm miniport to maintain triangulation.
One of the significant limitations of the existing one-port surgery is difficulty of suturing. However, the vaginal stump was closed via laparoscopy in the two laparoscopic hysterectomies that were performed. This new surgical technique can be used to overcome the limitation of suturing in the existing one-port surgery.
The level of satisfaction of the patients for LESS should be considered. However, the level of satisfaction related to LESS has never been reported in the field of gynecology. Our study showed that 83% of the patients had a positive perception on the surgical outcome. The biggest advantage of LESS voiced by the patients was the cosmetic outcome (94%). According to recent research, however, only 39% of 100 patients responded that the cosmetic result was an advantage of natural orifice surgery. 12 Further, Swanstrom et al. 13 showed that procedure-related risks, pain, and recovery time were more important than cosmetic outcome, cost, length of hospital stay, and type of anesthesia in the choice of natural orifice translumenal endoscopic surgery.
In conclusion, the advantages of LESS with a 2-mm miniport compared with the existing one-port surgery are several. First, LESS with a 2-mm miniport costs less, as it does not use a multilumen port. Second, no learning period is necessary, because LESS with a 2-mm miniport does not require bent or flexible instruments. Third, LESS with a 2-mm miniport is superior to one-port surgery based on cosmetic outcome, as it requires a 12-mm incision in the umbilicus. Fourth, maintenance of triangulation during surgery is easier compared with the existing one-port surgery. Fifth, laparoscopic suturing is possible.
Thus, LESS with a 2-mm miniport is feasible and a safe operative method in treating benign gynecologic diseases. Moreover, 81% of the patients had a positive perception on this surgery, and the cosmetic outcome contributed the most to the level of satisfaction. However, prospective clinical trials are required to determine the true benefits and utility of this novel surgical approach compared not only with conventional laparoscopic surgery but also with the existing one-port surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.