
Abstract
Abstract
Background:
Single-incision laparoscopic appendectomy (SILA) has been successfully performed in children. The intracorporeal approach, using reticulating instruments and 5- to 10-mm ports, has been described in recent reports. In this article, we describe our technique of performing SILA in children, using conventional 3- and 5-mm ports and instruments only.
Methods:
We conducted a retrospective review of all consecutive children who underwent SILA over a 3-month period by a standardized technique of using one 3-mm and two 5-mm ports. The procedure was completed intracorporeally by conventional instruments, and the specimen was retrieved without wound contamination by a simple method.
Results:
Eleven consecutive children (8–14 years), with a mean body weight of 38.5 kg, underwent successful SILA by our technique during the review period. Mean operating time was 83 minutes. There was no conversion to conventional laparoscopic or open appendectomy. Mean postoperative analgesic requirement was 2.4 doses of oral acetaminophen, and no narcotic analgesic was required. All the patients recovered smoothly without complications.
Conclusions:
SILA can be safely performed in children when using standard laparoscopic instruments without additional costs in equipment. Using 3- and 5-mm ports seems more appealing to children, with their smaller umbilicus, than adults.
Introduction
Methods
We conducted a retrospective study of all the consecutive children who underwent SILA over a 3-month period by a standardized technique, which was performed by conventional 3- and 5-mm instruments only.
Surgical techniques
Incision and placement of ports in triangular configuration
A hemicircumferential incision was made along the lower half of the umbilical ring, from 3 to 9 o'clock, down to the aponeurotic fascia. Dissection was then performed at the plane between the subcutaneous fat and the fascia, in a caudal direction to develop a fascial surface, having a radial distance of 1–1.5 cm from the umbilical stalk (Fig. 1). This was prepared for the placement of one 3-mm and two 5-mm ports (Storz, Tuttlingen, Germany), in a triangular configuration over the fascia. By the open method, a 5-mm port was inserted at the midline, just inferior to the umbilical stalk, for the laparoscope. In order to laparoscopically visualize the placement of the other two trocars, the length of the camera port left inside the peritoneal cavity was limited to 1 cm. This was accomplished by placing a short latex tube over the port for anchorage. A purse-string suture was placed on the fascia around the camera port, and the suture was hitched to the latex tube to secure the position of the port and to prevent air leak. Either a zero- or 30-degree lens was used. After the development of the pneumoperitoneum, another 5-mm working port was then inserted on the right side of the camera port at around 5 mm apart. The 3-mm port was placed at the leftmost and the most inferior edge of the fascial surface, which was around 10 mm away from the camera port. The three ports formed a triangular configuration, with the two working ports farthest away. By adjusting the positions of the latex tubes over the 3- and 5-mm working ports, the three ports were stationed with different extracorporeal lengths, with the longest for the camera port, to minimize collision at the back-ends (Fig. 2).

Development of fascial surface inferior to the umbilical stalk, following the hemicircumferential incision.

The 5- and 3-mm ports were stationed with different extracorporeal lengths to minimize collisions at the back-ends.
Appendectomy
Most of the time, the laparoscope was kept at the most dependent position, with the two operating instruments above to maximize freedom of movement of the working instruments and allow adequate triangulation at the operative site. A long 3-mm grasper was used for retraction on the appendix, while the peritoneal attachments were divided by the 5-mm hook cautery. The mesoappendix was divided by 5-mm hook cautery or a vessel-sealing device (LigaSure,™ Valleylab, Boulder, CO). Endoloops were placed at the base of the appendix, with double ligatures on the caecal side, followed by division of the appendix. Cross-hand maneuver might be necessary in parts of the procedure, particularly during the mesoappendix division and tightening of the endoloop, in order to enhance the instrumental triangulation at the operative site. The 3-mm grasper retracted the appendix upward and toward the head, while the other instrument, through the 5-mm port, crossed under the grasper to operate toward the base of the appendix (Fig. 3). After the appendix was divided, the endoloop suture on the specimen side was left uncut for specimen retrieval.
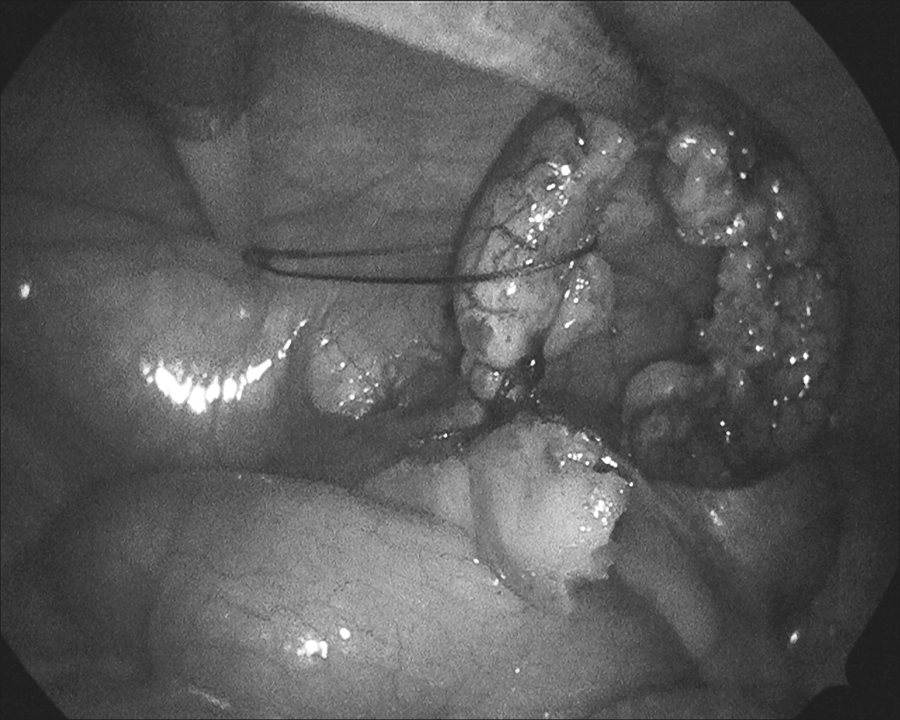
Cross-hand maneuver during the placement of the endoloop. The endoloop introducer, on the surgeon's right hand, crossed under the 3-mm grasper on the surgeon's left hand.
Specimen retrieval with wound protection
After the ports were removed, the two 5-mm port sites were incorporated into one by dividing the muscle in between, and the endoloop suture on the specimen was left intact through the incorporated wound. A small-size specimen retrieval bag with, the close-end cut away, was tunneled through the wound to protect it from being contaminated during appendix retrieval. The appendix was removed through the wound by pulling on the endoloop suture (Fig. 4).

Appendix extracted through the wound, which was protected by the specimen retrieval bag.
Results
Over a 3-month period from October 2009 to January 2010, 11 consecutive children underwent successful SILA by our technique. The patients ranged in age from 8 to 14 years, with a mean body weight of 38.5 kg (range, 31–53). Nine patients presented with acute appendicitis that required emergency surgery, and 2 children received an elective interval appendectomy, following successful conservative treatment for appendiceal abscess. Mean operative time was 83 minutes (range, 55–110). Among the 9 children with acute presentation, 2 had gangrenous appendicitis with perforation, while the rest had acute suppurative appendicitis, as confirmed by histology. There was no conversion to conventional laparoscopic or open appendectomy. All the patients recovered smoothly from surgery without any complications. Time to full diet varied from 24 to 84 hours, with the longest for the perforated appendicitis. Postoperative analgesic requirement ranged from 1 to 4 doses of oral acetaminophen (mean = 2.4 doses). No narcotic analgesic was required. During the study period, 5 other children underwent a conventional laparoscopic appendectomy in our institution. In 4 of them, the reason not to proceed to SILS was because of the unavailability of the senior surgeons, and that conventional laparoscopic appendectomy was performed by surgical residents. We made an active decision not to attempt SILS in a 3-year-old girl, who presented with generalized peritonitis, with a palpable mass extending to the umbilicus, when examined under general anesthesia. She underwent a conventional laparoscopic appendectomy for her complicated appendicitis, with full recovery. No patients received an open appendectomy during the review period.
Discussion
Successful application of SILA in children was recently reported, with both extracorporeal and intracorporeal approaches being described.6–9 An operating laparoscope was used in the transumbilical extracorporeal appendectomy.6,8 There have been, however, concerns about the potential increased risk of wound infection with the extracorporeal approach, and an ancillary 3-mm port was advocated as a modification to SILS to perform intracorporeal appendectomy. 10 Ates et al. have reported intracorporeal SILA by using a single port of two working channels or an operating laparoscope. 9 The procedure was performed by a single instrument, with the assistance of a transabdominal suture for retraction on the appendix. We believe this is a technically difficult method and difficult in gaining popularity. More recently, Dutta has reported the technique of multiple port placement, through a single vertical incision at the umbilicus, to perform the intracorporeal appendectomy with specially designed reticulating instruments. 7 In our technique, we used a hemicircumferential incision and developed a fascial surface inferior to the intact umbilical stalk for port placement, so as to retain the original configuration of the umbilicus after wound closure. The resultant scar can be easily concealed by the skin fold, which is usually prominent at the lower half of the umbilical ring. The incision is always adequate to accommodate one 3-mm and two 5-mm ports.
We used one 3-mm and two 5-mm ports, in contrast to three 5-mm or two 5-mm plus one 12-mm, as described by others.6,7 We believe the combination of ports, in our technique, seems more appealing to children, who have a smaller umbilicus than adults. This is particularly relevant to our Chinese children, whose body sizes are usually smaller than those of children in western countries. We do not agree that one should extend the skin incision beyond the umbilical ring to accommodate the ports, as that would defeat the whole purpose of performing SILS. The combination of two 5-mm and one 3-mm port minimizes the degree of surgical trauma, while allowing the procedure to be comfortably performed with appropriate instruments. The small size and placement of a 3-mm port at the leftmost and the most inferior edge of the fascial surface maximizes the distance between the two working ports in a triangular configuration with the camera port. This allows adequate triangulation of the two working instruments at the operative site and decreases collisions between the ports during instrumental movement. From our initial experience, keeping the laparoscope at the most dependent position, while having the working instruments above, allows the best freedom of instrumental movement, most of the time. When a cross-hand maneuver is required, the laparoscope may need to be pulled back to assess the relationship of the two working ports, with regard to which goes under the other. The surgeon may need to draw one of the instruments back into the lumen of the port in order to adjust the crossing relationship of the two working ports before further dissection. To the best of our knowledge, we are the first to report the use of a 3-mm port and instruments to perform SILA in children. Reticulating instruments, which are currently available at 5 mm only, have been used in other pediatric reports.6,7 Concern has been expressed regarding the mandatory demand for such costly disposable reticulating instruments, while the true benefit of SILS over the conventional laparoscopic approach has not been demonstrated. 10 By our technique, only standard laparoscopic instruments were used, and there was no additional cost in equipment. Although our case number was small, we have demonstrated that reticulating instruments are not essential to perform SILA in children. The procedure can be performed by conventional 3- and 5-mm instruments, which are most commonly used in standard laparoscopic procedures in children.
As we did not use any ports bigger than 5 mm in our method, the specimen could, in no way, be retrieved through any one of the ports, nor was it possible to push in a specimen retrieval bag through the lumen of the 5-mm port. We overcame this problem by incorporating the two 5-mm port wounds, and the resultant single wound was around 15 mm and big enough for specimen retrieval. We tunneled the wound with a specimen retrieval bag, with the close-end cut away to protect the wound from contamination by the appendix, which was extracted with the intact endoloop suture. We did not encounter any wound infection in this short series, and we believe this method is effective in protecting the wound without additional cost or the need for a special technique.
Concern has been expressed that SILS might be associated with more postoperative wound pain due to a bigger muscle defect and skin incision. The postoperative analgesic requirement, in this small case series, does not seem to compare unfavorably with that of conventional laparoscopic appendectomy. The wound incorporating the two 5-mm port sites measures around 15 mm and is comparable to the wound for the placement of a 10- or 12-mm port in the conventional approach. The fascial defect from the insertion of a 3-mm port is tiny. The degree of surgical trauma from the wound, in our method, should compare favorably with other methods when using ports of a bigger size. Randomized, controlled trials are needed to better evaluate the postoperative pain from SILA, in comparison to conventional approach.
The technique we have described is amenable to surgeons, as it does not require surgeon retraining, with respect to instrumental manipulation. The instruments used in our technique are already very familiar to those pediatric surgeons who have been well trained in standard laparoscopic procedures. Surgeons, however, still need to adapt to the new challenges in operating very much in line with the optic lens, the need for cross-hand maneuvering, and the way to decrease collisions between instruments. Although the operating time seemed to be longer than that expected from the conventional laparoscopic approach, we believe this would be shortened with the accumulation of experience of the individual surgeon. As there are no additional costs in specially designed disposable instruments, we believe our technique would promote the popularity of using the SILS approach to perform an appendectomy in children.
Conclusions
Our initial experience suggests that SILA can be safely performed in children when using conventional laparoscopic instruments, at no additional costs for equipment. Using 3-and 5-mm ports and instruments sounds more appealing for children and gives the potential for this method to be a viable alternative to the conventional laparoscopic approach. Being a common procedure, with relatively straightforward dissection, the appendectomy appears to be the most suitable procedure to begin the development of SILS in children.
Footnotes
Acknowledgments
The study was solely supported by the Department of Surgery, The Chinese University of Hong Kong (Hong Kong, China).
Disclosure Statement
No competing financial interests exist.