
Abstract
Abstract
Salpingoscopy is an endoscopic technique that allows the direct visualization of the tubal mucosa. The status of the tubal mucosa is the best prognostic factor when evaluating patients with tubal infertility. Salpingoscopy, performed during laparoscopy, has not reached wide acceptance due the costly, non-user-friendly, dedicated instrumentation needed. In this article, a simplified technique to perform salpingoscopy at the time of laparoscopy is reported, using a standard 2.9-mm diagnostic hysteroscope, with a 3.7-mm single-flow diagnostic sheath, introduced through an accessory port. Salpingoscopy, with this new technique, was performed in 13 patients with tubal infertility. The tubes were successfully cannulated in all patients, for a total of 24 tubes evaluated (2 patients had a single tube). Salpingoneostomy and salpingoovarolysis were completed after salpingoscopy only when the tubal mucosa was normal. In 1 patient with severe tubal damage, salpingectomy of the single remaining tube was performed. Salpingoscopy added a mean of 15 minutes to surgical time. Intrauterine pregnancies were obtained, after salpingoneostomy, fimbrioplasty, or adhesiolysis, in 5 of 12 patients (42%), with a mean follow-up of 9 months. The simplified technique of salpingoscopy, with a diagnostic hysteroscope introduced through an accessory trocar at the time of laparoscopy, adds important information on the reproductive potential of patients with tubal disease.
Introduction
Results of tubal reconstructive surgery vary in relation to the degree of tubal disease. In cases of distal tubal occlusion (DTO), live birth rates are reported to be between 39 and 59% in cases of mild disease, whereas they drop to less than 15% in cases of severe disease. 2 In cases of peritubal adhesions, term pregnancy rates are reported to be around 50%. 1 Selection of patients with good reproductive prognosis after surgery is, therefore, pivotal in the diagnostic workup of infertile patients. There is no consensus, however, on which method for the evaluation of the fallopian tubes, and of which classification of tubal damage, should be used. 5 Available methods include hysterosalpingography (HSG), laparoscopy with chromopertubation, and selective tubal cannulation, 2 all of which, however, have the limitation of not evaluating directly the tubal mucosa.
Salpingoscopy, performed during conventional laparoscopy or during transvaginal hydrolaparoscopy (THL), is an endoscopic technique that allows the direct visualization of the tubal mucosa. Laparoscopic salpingoscopy has the advantage of being performed after a complete evaluation of the abdominal and pelvic cavity. Further, it is possible to perform the surgical correction of any tuboperitoneal disease under the same procedure. Transvaginal salpingoscopy, at the time of THL, has the advantage of being performed under local or no anaesthesia, but its main limitations are that the field of vision is restricted to the pouch of Douglas, and that no operative procedures may be performed. For this reason, THL should be reserved to patients in whom no pelvic pathology requiring surgical treatment is suspected preoperatively. 6
The status of the tubal mucosa has been reported to be the best prognostic factor when evaluating patients with infertility due to DTO or peritubal adhesions.1,4,7 In a study by Marana et al., 1 in fact, no correlation between the extent of tubal damage, as evaluated with the American Fertility Society (AFS) classification 8 and postoperative reproductive outcomes, was found, for patients undergoing either salpingoneostomy or salpingoovarolysis. On the other hand, a strong correlation was present between the degree of endotubal damage, as evaluated by salpingoscopy, and postoperative reproductive outcomes. 1 The AFS classification, 8 published in 1988, recognizes the importance of the status of the ampullary endosalpinx as a prognostic parameter. However, in 1988, it was decided not to include it in the scoring system, since, at that time, salpingoscopy was “not being practiced universally.” We believe that the reluctance of including salpingoscopy in the diagnostic workup of patients with tubal infertility is due to the costly, non-user-friendly, instrumentation needed at the time of laparoscopy. A dedicated set of instruments, consisting of an operative laparoscope and an endoscope specifically designed for tubal cannulation, are, in fact, needed besides the conventional laparoscopic instrumentation. A much simplified technique for tubal endoscopy is presented in this article.
Materials and Methods
We propose here a simplified technique to perform salpingoscopy at the time of laparoscopy. Laparoscopy is performed with a 10-mm laparoscope introduced in the umbilicus and two or three accessory 5-mm trocars introduced suprapubically and lateral to the inferior epigastric vessels. A standard 2.9-mm diagnostic hysteroscope, with a 3.7-mm single-flow diagnostic sheath (26120BA and 26182D; Karl Storz GmbH, Tuttlingen, Germany), is then introduced through one of the accessory ports. In the case of DTO, a small 3- to 4-mm opening is created with a monopolar needle or scissors at the avascular point at the center of the radial scars, which is the site of fusion of the fimbrial folds, and corresponds to the original site of the ostium. The tube is then grasped with an atraumatic forceps and cannulated with the hysteroscope under laparoscopic vision (Fig. 1) and distended with lactated Ringer's solution introduced through the hysteroscope sheath. At this time, the operator switches vision from the laparoscope to the hysteroscope for the evaluation of the tubal mucosa (Fig. 2). As with conventional salpingoscopy, with this new technique, the tubal mucosa can be explored down to the isthmic-ampullary junction. The status of the tubal mucosa can, therefore, be evaluated according to Brosens' classification. 7
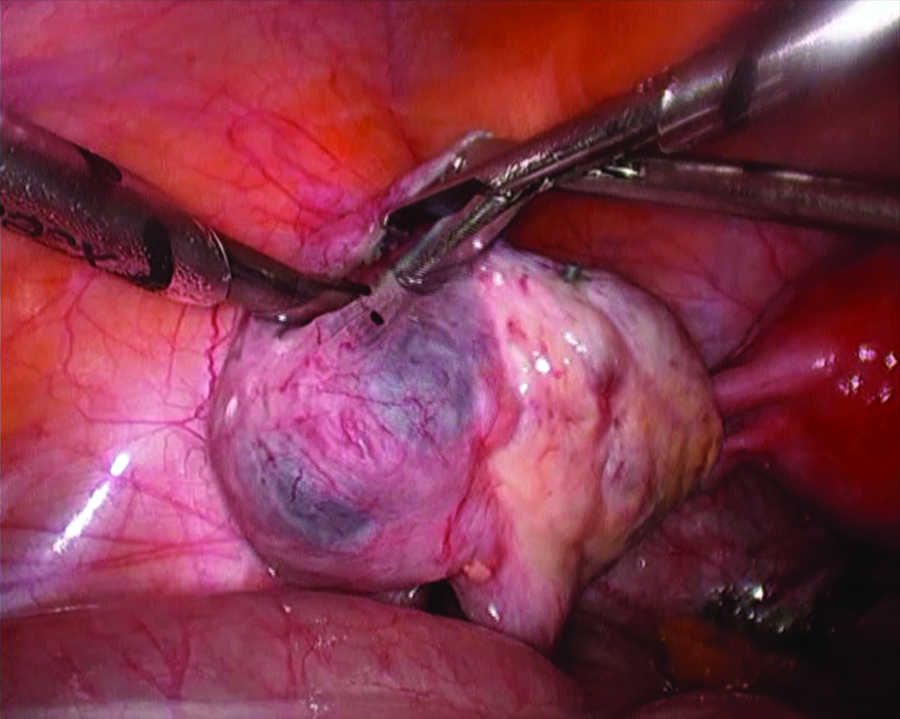
After the creation of an opening in the distally occluded tube, the small-caliber hysteroscope is introduced into the ampulla through an accessory trocar under laparoscopic vision.

The major and minor folds of the ampullary mucosa are visualized at salpingoscopy.
Since January 2008, we performed salpingoscopy with this new technique in 6 patients with bilateral DTO, in 2 patients with DTO of the single remaining tube, and in 5 patients with fimbrial phymosis or peritubal adhesions for a total of 13 patients evaluated. One of the 2 patients with DTO of the single remaining tube had been previously submitted elsewhere to salpingoneostomy by laparoscopy for a previous DTO, which appeared to have recurred at HSG performed after 1 year of unsuccessful attempts at obtaining pregnancy postoperatively.
All patients were of reproductive age (mean age, 34 years; range 28–39), had normal ovulatory cycles, and body mass index (BMI) within normal range (mean BMI, 21.2; range, 17.7–25.4). All patients were infertile, with a mean duration of infertility of 2.3 years (range, 1.0–5.0). No associated severe male factor was present. All patients had a preoperative diagnosis of tuboperitoneal factor of infertility, based on preoperative HSG, transvaginal sonography, or both. Laparoscopy, with an attempt at salpingoscopy, was, therefore, scheduled for all patients.
Results
Laparoscopy was performed in all patients, without intra- or postoperative complications. The tubes were successfully cannulated in all cases. In 2 patients, one tube was absent for previous salpingectomy. A total of 24 tubes were, therefore, cannulated.
In all patients, the presence of a tuboperitonal factor of infertility was confirmed, according to the preoperative suspect. In particular, 6 patients had a bilateral DTO (associated with moderate to severe adhesions, according to the AFS classification 8 ), 2 patients had a DTO of the single remaining tube associated with severe adhesions, 2 patients had fimbrial phymosis with associated peritubal adhesions, and 3 patients had moderate to severe peritubal adhesions with normal, patent tubes. In 4 patients, associated minimal endometriosis was present and treated.
Salpingoneostomy and salpingoovarolysis were completed after salpingoscopy in 12 of the 13 cases, when the tubal mucosa was normal. In 1 patient, with a recurrent DTO of the single remaining tube, laparoscopy revealed the presence of a large-caliber hydrosalpinx with associated severe adhesions (the tube appeared to be completely stuck to the anterior abdominal wall). After lysis of adhesions, salpingoscopy revealed the absence of normal mucosal folds. It was, therefore, decided to proceed to salpingectomy. Salpingoscopy added a mean of 15 minutes to the total surgical time (ranging from 8 to 20 minutes). Intrauterine pregnancies were obtained, after salpingoneostomy, fimbrioplasty, or adhesiolysis, in 5 of 12 patients (42%), in spite of a brief follow-up (mean follow-up, 9 months).
Discussion
With the simplified technique described in this article, patients with tubal disease can be classified during laparoscopy in a good prognostic group, when the tubal mucosa is normal, and in a poor prognostic group, when the tubal mucosa is damaged, with no additional costs for dedicated instrumentation. In a previous study, describing the use of salpingoscopy during laparoscopy, 1 we reported a 71% cumulative pregnancy rate after salpingoovarolysis, and a 64% cumulative pregnancy rate after salpingoneostomy for DTO, in patients with a normal tubal mucosa. These figures compare favourably with the 50 and 26% pregnancy rates in a nonselected group of patients with peritubal adhesions and DTO, respectively. 1
Conclusions
The simplified technique of salpingoscopy described in this article, performed with a standard small-caliber diagnostic hysteroscope introduced through an ancillary trocar at the time of laparoscopy, allows the evaluation of the endosalpinx in cases of tubal disease, at no significant additional costs. The evaluation of the tubal mucosa is of paramount importance in the selection of patients who may be able to most benefit from tubal surgery, therefore avoiding indiscriminate referral to IVF. The endoscopic procedure may allow the selection of patients who may best benefit from tubal surgery, with results in terms of live birth rate over 60% after 1 year. 1 Good clinical practice entails giving to the patient the gold-standard treatment for a specific disease, which should be the best or the most successful diagnostic or therapeutic modality for a condition. In cases of tubal damage, laparoscopy with salpingoscopy completes the diagnostic workup, which, in most cases, is not completed with early referral to IVF. Also, with better selection of ideal candidates, tubal surgery compares favorably in terms of reproductive outcome with IVF, which, according to the last published results for the United States, offers a 29.9% live birth rate per initiated ovarian stimulation cycle. 9
Footnotes
Disclosure Statement
No competing financial interests exist.