
Abstract
Abstract
Double-J ureteral stenting during laparoscopic surgery is technically demanding, time consuming, and stressful. We report here on a new, time-saving, and straightforward method to insert a Double-J stent, which is used during laparoscopic ureteral reimplantation.
Introduction
Technique
We performed transperitoneal extravesical laparoscopic ureteral reimplantation by using four ports for the patients who had lower ureteral stricture. To avoid placing tension on the anastomotic site, we dissected the ureter from the pelvic peritoneum up to the crossover point of the common iliac artery and the ureter. After exposing the bladder mucosa, an incision was made in the most caudal end of the mucosa.
The divided ureter was pulled out through the 10-mm port site that was nearest to the ureter (Fig. 1). The pneumoperitoneum was eliminated to decrease the distance between the ureter and the abdominal wall so as to facilitate drawing the longer ureter from the abdomen. After the trocar was removed, the end of the ureter was spatulated. The DJ stent was inserted into the ureter over the guidewire and the guidewire was removed by hand without stress, the same as in open surgery. The ureter with the DJ stent was reinserted into the abdomen (Fig. 2) and the removed trocar was reinserted as well. The ureter was reimplanted without tension, torsion, or angulation, with mucosal-to-mucosal apposition.
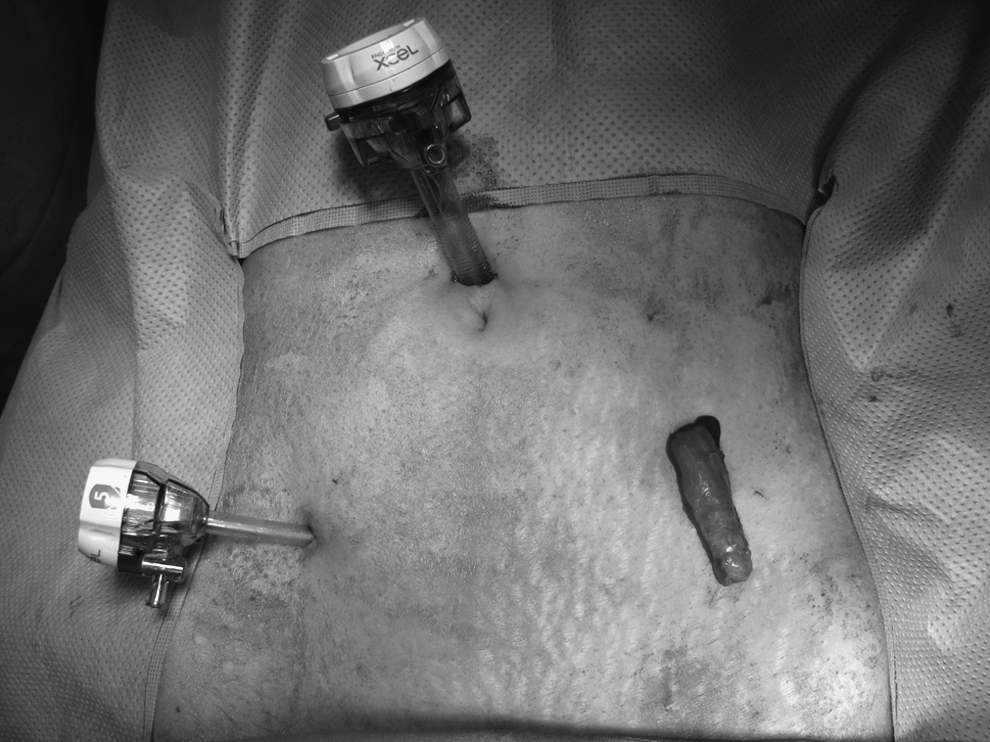
The divided ureter was pulled out through the port site that was nearest to it.

The ureter with Double-J stent was reinserted into the abdomen.
Discussion
Ureteral stenting is indispensable in many ureteral operations. Cystoscopic retrograde stenting of the ureter usually requires time-consuming position change. Retrograde stenting with flexible cystoscopy to avoid position change may be difficult in male patients with large median prostate lobe and in female patients. Laparoscopic antegrade placement of DJ stent remains technically demanding and time consuming. The advantage of the present technique is that it avoids the position change during retrograde DJ stenting, but also avoids the need for additional use of equipments such as flexible cystoscope or epidural catheter. 3 The biggest strength of this technique is that it requires little dexterity to handle the pliable DJ stent. The disadvantage of this technique is that it requires the care of preserving the periureteral tissue as to not disrupt the blood supply. It is the longitudinal vascularity that allows the ureter to be safely mobilized from the surrounding retroperitoneal tissues without compromising the vascular supply, provided that the periureteral adventitia is not stripped.
We used this technique in three consecutive transperitoneal laparoscopic ureteral reimplantations. The technique allowed perfect placement of the stent in all 3 cases within 3 minutes without any difficulty. Radiologic images were normal without ureteral stricture or reflux in all patients at postoperative 3 months. This was a simple and straightforward technique that required about the same dexterity as for open surgery.
Disclosure Statement
No competing financial interests exist.