
Abstract
Abstract
Purpose:
One-trocar–assisted pyeloplasty (OTAP) is a recent, not yet well-known surgical technique for the treatment of ureteropelvic junction obstruction, described for the first time by El Gohary in 2004. The first step of this procedure is to identify the pyeloureteral junction (PUJ) through a laparoscopic approach using one trocar, and the pelvic-ureteric anastomosis is carried out in “open” surgery. We present our experience with OTAP, an innovative technique in pediatric surgery.
Materials and Methods:
From October 2005 to December 2009, 39 patients (27 males and 12 females) with UPJ obstruction underwent OTAP. The age of these patients ranged from 1.5 month to 18 years (mean age: 5.3 years), especially 18 of them were under the age of 1 year. Despite the age difference, the technique was carried out using the same procedure. A retroperitoneal space was created and the PUJ was identified and dissected from the surrounding tissue with one trocar (10 mm) and an operative telescope, then the PUJ was brought up through the trocar site, and the anastomosis was performed using 6/0 absorbable sutures. Any redundant renal pelvis was reduced where needed.
Results:
All patients successfully underwent OTAP. An aberrant crossing vessel was found in 8 patients. The mean operative time was 78 minutes (range: 65–90 minutes) and the mean hospital stay was 2.5 (2–4) days. All children returned to full activity within 7 days. The follow-up mean was 24 months (range 1–49); all patients were asymptomatic.
Conclusion:
Our medium-term results confirm that OTAP is an innovative technique, which allows a safe approach for children and, moreover, it is applicable to the entire range of ages. However, a good practical experience is required.
Introduction
For many decades, open surgery has been the most common approach for pyeloplasty worldwide, but, recently, with the rapid progress of minimally invasive surgical techniques in children, the way to access the kidney and pelvis has changed.2,3
The transperitoneal, retroperitoneal, and robotic approaches have all been reported, with advocates for each procedure.4–6
Theoretically, the transperitoneal approach increases the risk of abdominal organ injury, and even if it is possible to carry out an easier dissection through the retroperitoneal approach, the small operative space and the technical difficulties have limited this application.
In 2004, El Gohary 7 performed laparoscopic-assisted Anderson-Hynes pyeloplasty in children with ureteropelvic junction obstruction.
The first step of this procedure is to identify the pyeloureteral junction (PUJ) through a laparoscopic approach using one trocar, and the ureteropelvic anastomosis is carried out in “open” surgery.
We present our initial experience with one-trocar–assisted pyeloplasty (OTAP), an innovative technique in pediatric surgery.
Patients and Methods
From October 2005 to December 2009, 39 pediatric patients (27 males and 12 females) with pyeloureteral junction obstruction (UPJO) underwent OTAP. The age of these patients ranged from 1.5 month to 18 years, especially 18 of them were younger than 1 year.
The surgical indication was UPJO diagnosed by renal ultrasonography, voiding cystouretrography, and renal scintigraphy mercaptoacetyltriglycine (MAG 3) or diethylene-triamine-polyamino-carboxylic acid (DIPA). Obstruction was established when the ultrasounds revealed severe hydronephrosis or an anterior–posterior diameter of >25 mm and, moreover, when the scintigraphy showed an obstruction with a half-time clearance of >30′ with reduced renal function.
In our group of patients, 17 were symptomatic: 14 presented abdominal pain, 3 recurrent urinary tract infection, and the rest had a antenatal diagnosis; for these the surgical indication was worsening of pyeloureteral dilatation at ultrasounds and/or reduction of renal function in asymptomatic patients.
The UPJO was on the left side in 23 patients, on the right side in 16 patients, and bilateral in 2 patients.
Despite the age difference, the technique was carried out using the same procedure.
Technique
Under general anesthesia, a catheter is inserted into the bladder and the patient is laterally positioned in standard flank. Through a 13-mm-long 11th or 12th subcostal incision, the Gerota's fascia is approached by separating the muscles instead of cutting them. Then this is opened and the operative telescope is introduced under direct vision (Fig. 1). A retroperitoneal working space is created by gas insufflations dissection. The insufflations pressure is <8 mmHg and the flow rate of CO2 is progressively increased from 1 to 3 L/min.
Trocar position for pneumoretroperitoneum.
The first step of the procedure is to identify the PUJ, which is anteriorly approached. Dissection is accomplished by a single instrument, inserted through the operative telescope; generally, this is a endo peanut (5 mm) that can be alternated to endo dissect or endo shear with unipolar cautery.
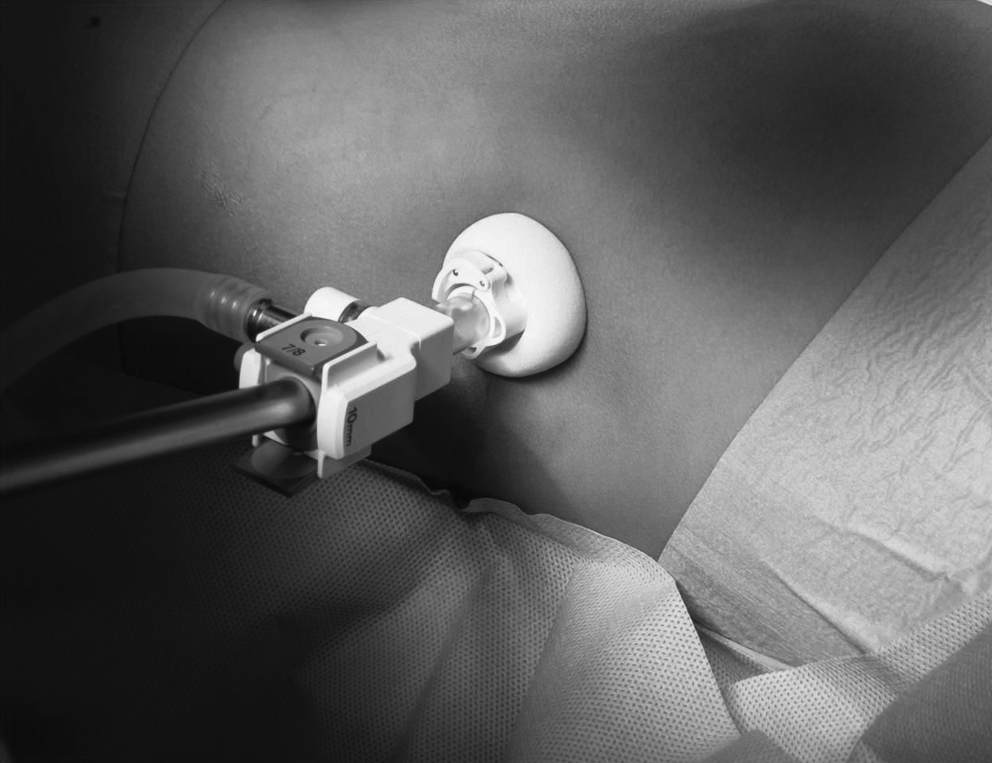
The PUJ exposition is obtained by identifying the proximal ureter in the retroperitoneum. A minimal dissection is used to free the PUJ from the connective tissue around it. Small vessels are divided by electrocoagulation. The anterior surface of the PUJ is cleared to identify any polar crossing vessels. The PUJ is exteriorized by a vessel loop through the trocar (Fig. 2) and a dismembered pyeloplasty is performed using 6-zero polydioxanon and a tapered 3/8 circular needle (Figs. 3 and 4). When the PUJ is obstructed by aberrant crossing vessel, ureteral transposition is necessary before realizing pyeloplasty. Any redundant renal pelvis is reduced where needed.

Exteriorization of pyeloureteral junction obstructed.

Pyeloureteral junction sectioned.

Pyeloplasty performed in open surgery.
A polyurethane Double-J stent is routinely inserted before completing the pyeloureteral anastomosis and it remains indwelling for 4–5 weeks. It is very important to choose the correct diameter of pigtail to permit an easy introduction of them by anterograde way without problems or complications. Once in site, the methylene blue and serum physiological solution is injected by bladder catheter to control the function of the stent and the correct position. Generally, it is possible to observe many drops coming up to the pelvic extremity of the pigtail.
A final retroperitoneoscopic look is useful to check the anastomosis (twisting and lick) and to value bleeding. A drain is placed in the retroperitoneal space at the end of the procedure.
The bladder catheter remains in all patients for 24 hours after surgery. Prophylactic antibiotics (third-generation cephalosporin) are routinely prescribed for 4 days and then half-doses are taken with continuity until the pigtail is removed.
Results
All patients successfully underwent OTAP. We realized 41 procedures (39 monolateral [95.1%] and 2 bilateral [4.8%]). The diagnosis of PUJ was intraoperatively confirmed in all cases.
We found 31 real stenosis (75.6%; 1 UJO of the lower moity), 8 aberrant crossing vessels (19.5%), 1 ureteral valve (2.4%), and 1 bifid pelvis (2.4%). The mean operative time was 78 minutes (range: 65–90 minutes). The presence of aberrant crossing vessels did not change the mean operative time. In 8 cases (19.5%), it was necessary to empty the voluminous pelvis before its exteriorization.
There were no intraoperative complications. There was one conversion (2.4%) in open surgery, because mobilization of PUJ was considered insufficient. The mean hospital stay was 2.5 (2–4) days. All children returned to full activity within 7 days after surgery.
The cosmetic results were excellent. A Double-J stent was removed by cystoscopy in all patients at 4–6 weeks after surgery. The mean follow-up was 24 months (range: 1–49); all patients were asymptomatic.
The success of OTAP has been defined by symptomatic improvement, decrease of hydronephrotic changes or dilatation of the renal pelvis on sonography, evaluated at 1, 3, 6, and 12 months, and a decrease on nuclear scan of the furosemide test washout parameters (<15′) with an improvement of renal function in those patients in whom that was compromised.
Discussion
Over the last few years, laparoscopy has played an increasing role in pediatric surgery, especially for the treatment of urologic pathologies. Laparoscopic pyeloplasty was introduced into adult surgery in 1993 and today it is a very popular procedure. However, this is not available for children. The main problem for the spread of this technique in pediatric surgery is the choice of the approach to the UPJ. In fact, the transperitoneal way has been the only option for several years. The reason is that this method is easier to use because of the larger working space in the peritoneal cavity. However, this is the only advantage; in fact, it requires colon mobilization, increasing the risk of visceral damage and other complications such as the adhesion and/or obstruction of the bowel.8,9
Nowadays, even a retroperitoneal approach is possible, to avoid all these possible complications. In this way, the peritoneal cavity remains unimpaired, and moreover, retroperitoneoscopy is feasible and safe. However, the minimal working space, especially in younger children, makes this surgery difficult to carry out; therefore, its use is still limited in pediatric surgery. Moreover, the use of this approach is much more frequent for ablative, but not for reconstructive procedures such as pyeloplasty, for which open surgery remains the gold standard. Recently, robotic surgery has been performed in a few selected centers, but very expensive equipment is required.
Several techniques have been described; they should be efficacious but less invasive to reduce the surgical trauma in children. For this reason, video-assisted pyeloplasty has been of great interest since it was first presented. This technique is a very interesting subject of study, because, unlike others, it can combine the advantages of laparoscopic methods with those of traditional surgery. In fact, at the beginning it is possible to exploit laparoscopic vision to easily identify the PUJ without performing extensive dissection, and moreover, the minimal invasiveness reduces the duration of recovery and favors esthetical effects. When the PUJ is released and externalized, a traditional pyeloplasty is performed with accuracy. This is useful to exceed retroperitoneoscopy limits because of the minimal space. Even if this technique is still at the experimental stage and the results reported in literature are limited, they are very encouraging, because they show the unquestionable value of OTAP, very good patient tolerance, few conversions to laparotomy, and surgical duration similar to other methods of traditional laparoscopy, even if the ureteropelvic junction obstruction is due to aberrant crossing vessels. Dissection is possible with a single tool without any risk, and PUJ exteriorization is gentle and nontraumatic. OTAP combines the advantages of a laparoscopic approach, such as reduced invasiveness, less postoperative pain, short hospital stay, and good cosmesis, and the advantages of a traditional surgery, such as high accuracy, to realize the pelvic anastomosis in a comfortable working space.
Moreover, the technique has not shown any complications yet and patients return to normal life activities within 7 days. The efficacy of the treatment is tested at the follow-up, when all the patients are asymptomatic and show a notable reduction of the pelvic dilatation at US control.10,11
It is important to say that this technique needs further evaluation, because the case reports are limited; thus, a long training is needed to obtain more knowledge about the technique and the necessary ability to carry it out.
OTAP is also achievable with accuracy in children and infants, because despite the different size, the technique is safe. This is a very important fact, because the progress of prenatal diagnosis makes more frequent surgical treatment in infants with hydronephrosis, wherein the other techniques such as retroperitoneoscopy and laparoscopy showed limits and difficulty. However, all the good results so far increase the validity of OTAP, so that it could become the treatment of choice for all variants of ureteropelvic junction obstruction, or anyway, this mininvasive approach could be considered the first step for major retroperitoneoscopy for the population of young surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.