
Abstract
Abstract
Purpose:
There are numerous published reports of laparoscopic resection of choledochal cysts (CDCs), but almost all involve extracorporeal reconstruction of a biliary drainage system. We describe and evaluate the technique of laparoscopic CDC resection with total intracorporeal reconstruction.
Methods:
We reviewed all patients who underwent a laparoscopic CDC resection from March 2005 to January 2010 at Rocky Mountain Children's Hospital and Children's Hospital of New York-Presbyterian. We obtained data on operative time, characteristics of reconstruction, time to initiation of diet, length of stay, complications, and outcome.
Results:
Thirteen patients (median age 5 years, range 1–16) underwent a laparoscopic CDC excision with total intracorporeal reconstruction. Four ports were used in all cases and no patients required conversion to an open procedure. Operative time ranged from 130 to 325 minutes (median 240 minutes). Median time to initiation of diet was 1 day (range 1–4 days). Median length of stay was 5 days (range 4–8 days). There were no cases of cholangitis; however, 1 patient developed a small bowel obstruction requiring re-operation.
Conclusion:
Laparoscopic resection of CDCs with total intracorporeal reconstruction is a safe and effective technique. The minimal handling of the bowel appears to minimize postoperative ileus, allows for early postoperative feeding and discharge.
Introduction
With the advent of laparoscopic surgery, more pediatric procedures are being performed with a minimally invasive approach. 1 The first laparoscopic CDC excision was reported by Farello et al. 2 in 1995. Currently, there are more than a dozen case reports and series describing experiences with laparoscopic excision of CDCs.1,3–17 However, the majority of these describe construction of the Roux-en-Y jejunojejunostomy extracorporeally. 13 Many authors prefer this method citing concerns of longer operative time and technical difficulty when performing the anastomosis laparoscopically. 14
Currently, only one series reported laparoscopic CDC excision with total intracorporeal reconstruction. 18 Creation of the jejunojejunostomy intracorporeally may decrease the incidence of postoperative ileus and contribute to earlier initiation of feeding. We report our experience with 13 cases of laparoscopic CDC excision using a total intracorporeal cyst excision and reconstruction.
Methods
We identified and reviewed the records of all pediatric patients found to have a CDC who underwent a laparoscopic excision followed by an intracorporeal hepaticojejunostomy and jejunojejunostomy between March 2005 and January 2010. The operations took place either at Rocky Mountain Hospital, Denver, Colorado, or at The Children's Hospital of New York-Presbyterian, New York, NY.
Informed consent for surgery was obtained from each patient's parent in all cases. The patient records were all reviewed for age at operation, operative time, time to initiation of diet, length of hospital stay, complications, and outcome. Study approval was granted by the Columbia University Institutional Review Board (IRB-AAAF0772).
Surgical technique
The procedure was performed in either the supine or dorsal lithotomy position depending upon the size of the patient. Infants and toddlers were placed near the foot of the table in a frog leg position. Older patients were placed in stir-ups with the lower legs angulated down at 90°. The surgeon stood between the patient's legs.
A combination of ports, 5–12 mm, was used depending on the size of the patient. A four-port technique has been used in all cases. A 5-mm umbilical port is initially used for the 5-mm laparoscope. The right-hand operating port is placed in the midclavicular line slightly above the umbilicus. The left-hand port is placed in the midclavicular line at or slightly below the umbilicus (Fig. 1). This creates the optimal operating angle of 90° between these ports at the porta of the liver, where the most difficult maneuvers take place.

(
A fourth port is placed in the anterior axillary line in the right upper quadrant. Through this port, a laparoscopic babcock clamp is used to grasp the gallbladder and retract it superiorly, exposing the cystic duct and the porta hepatis. This clamp is attached to the drape to provide a self-retaining retractor. The gallbladder is left in place during the entire procedure to provide exposure of the porta, thus eliminating the need for a more traumatic liver retractor.
The cystic duct is isolated and, if needed, a cholangiogram is performed. This is rarely necessary as the majority of these patients had a preoperative endoscopic retrograde cholangiopancreatography or magnetic resonance cholangiopancreatography. The cystic duct is clipped and divided allowing easier access to the common bile duct.
The extrahepatic biliary system is then mobilized and dissected. This is done with a combination of sharp and hook cautery dissection. The Ligasure® device (Covidien, Norwalk, CT) has been used in larger patients with significant inflammation to minimize bleeding. In all cases the duct was dissected away from the surrounding portal vein and hepatic arteries. Marsupialization of the back wall was not necessary in any case, despite significant inflammation present in 4 cases. Dissection was carried proximally to the confluence of the right and left hepatic duct, and the common hepatic duct was divided just distal to this bifurcation. The common bile duct was then retracted medially facilitating distal dissection and ligation of the duct behind the duodenum. To ligate the CDC distally, #0 PDS endoloops were used in all cases.
With CDC resection complete, the Roux limb was constructed intracorporeally. The jejunum was divided ∼10–15 cm distal to the ligament of trietz, and a 25–30 cm Roux limb was constructed. An end to side jejunojejunostomy was constructed with running 3-0 Vicryl in smaller patients and a side to side stapled anastomosis in patients over 10 kg. In larger patients the umbilical port was increased to a 12-mm port to introduce the stapler, divide the bowel, and create the stapled anastomosis (Fig. 2). In smaller patients the bowel was simply cut and sewn intracorporeally with a running stitch. The Roux limb was brought up in a retro-colic fashion and the hepaticojejunostomy was created using interrupted 5-0 PDS suture (Fig. 3).
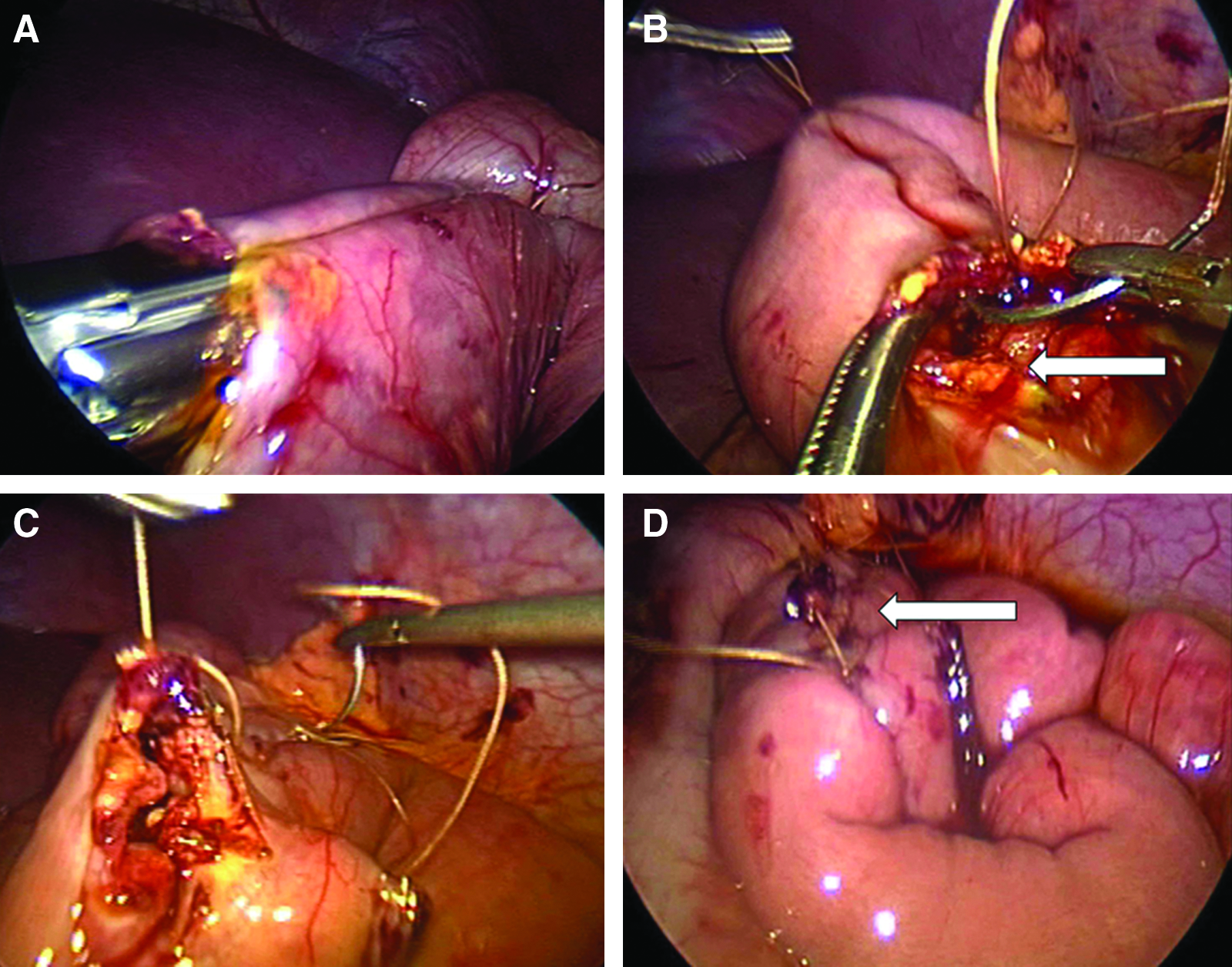
Performance of the intracorporeal jejunojejunostomy. (
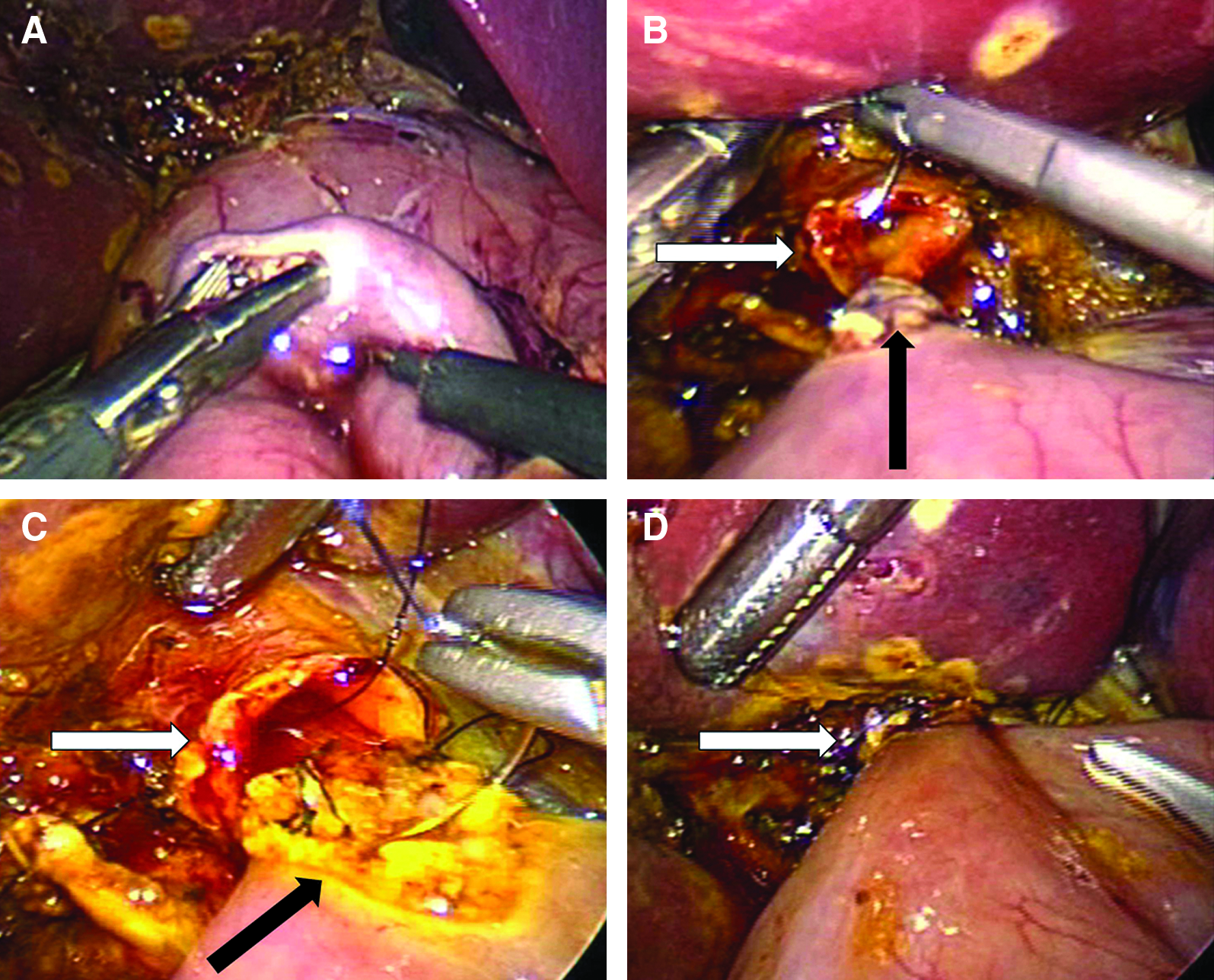
Performance of the hepaticojejunostomy. (
The gall bladder was then dissected from the liver bed and the gallbladder and CDC were removed via the umbilicus. A closed suction drain was left behind the biliary anastomosis in all cases.
Results
A total of 13 patients underwent a laparoscopic CDC excision with intracorporeal reconstruction (Table 1). Age at time of operation ranged from 1 to 16 years. Pain was the presenting symptom in 9 of 13 patients (70%). Signs on presentation were jaundice (5/13), palpable mass (2/13), and fever (1/13). Nine patients had hyperbilirubinemia and 2 patients had increased transaminases. The disease in one patient was diagnosed on prenatal ultrasound.
Four operative ports were used and there were no conversions to an open procedure. The hepaticojejunostomy and jejunojejunostomy were performed intracorporeally in all cases. Operative time ranged from 130 to 325 minutes (median 240 minutes). The cyst was able to be completely excised in all of our patients. Median time to initiation of diet was 1 day postoperatively. The median length of stay was 5 days.
There were no cases of postoperative cholangitis or pancreatitis. One patient had bilious output in the Jackson-Pratt drain; however, this ceased by the second postoperative day. One patient developed a small bowel obstruction that presented 2 weeks postoperatively. An exploratory laparotomy revealed that the jejunojejunostomy had herniated though the defect that had been made in the transverse mesocolon, thereby leading to a proximal obstruction. There were no deaths.
Discussion
Farello et al. 2 published the first case of a laparoscopic CDC excision in 1995. Since that time an increasing number of institutions have adopted this technique, with good success. Laparoscopic excision of CDCs has been purported to give better observation, a better cosmetic result, potentially less postoperative pain, and a shorter recovery. 5
The number of ports used varies depending on the series, but most commonly five ports have been used. 6 Typically, the laparoscope is inserted at the umbilicus, two operating ports on either side of the umbilicus, a left upper quadrant port to retract the liver and a right lower quadrant assistant port. 18 In the current series, the gallbladder was grasped and used to retract the liver, making the fifth port unnecessary. 6 Jang et al. described a four port technique in 2006. 16 Our technique is similar with the laparoscope at the umbilicus and two operating ports on either side, but we used a right upper quadrant port to retract the gallbladder. This gave us excellent observation of the cyst and facilitated excision. Use of the Ligasure device has also proven to be helpful when significant inflammation is encountered around the cyst.
In most series, the jejunojejunostomy is fashioned extracorporeally. 5 The main argument for performing an extracorporeal anastomosis is that it decreases the operative time. Le et al. 14 performed eight laparoscopic CDC resections, with six extracorporeal and two intracorporeal anastomoses. They reported an average time of 65 minutes for the intracorporeal and 13 minutes for the extracorporeal anastomoses. Recently, a series of 6 patients was reported using a totally intracorporeal excision and anastomosis. 18 The average jejunojejunostomy time was 38 minutes in the series. We performed a total intracorporeal jejunojejunal anastomosis in all 13 of our cases. Our average time for the jejunojejunostomy was not measured, but our operative times are comparable to previously reported series. In larger patients, performance of this anastomosis is greatly facilitated by using a stapler with suture closure of the open ends (Fig. 2).
Case series of laparoscopic CDC excision have shown that operative times have decreased as experience with this technique has grown. 15 This is true for our series as well. Our initial 8 cases revealed decreasing operative times with the senior surgeon performing all of the procedures. As we began to expand our experience to an additional institution, our operative times increased somewhat. This is likely due to a second learning curve at the new institution and with pediatric surgical residents now performing the majority of the procedure. Some authors argue against fashioning the jejunojejunostomy intracorporeally due to longer operative times. In other series, the operative time has ranged from 240 to 585 minutes. 17 Our mean operative time was 240 minutes. This suggests that performing the jejunojejunostomy intracorporeally does not unreasonably lengthen the operation.
Time to initiation of diet has been reported to be between 3 and 7.6 days postoperatively.6,16 Our patients were able to tolerate oral feeds earlier, median of 1 day, than in other series that performed an extracorporeal jejunojejunostomy. 5 There were no incidences of vomiting or need for reinsertion of nasogastric tube in our series. Ahn et al.'s series of totally intracorporeal reconstruction did not report time to initiation of diet. 18 The median length of stay in our patients was 5 days. This is shorter than the previous series, in which the length of stay has ranged from 5.5 to 12.5 days.4,11,14–19
Known complications of CDC excision are cholangitis, bile leak, intrahepatic duct stone formation, and pancreatitis. In the laparoscopic literature, the rate of bile leak has ranged from 0% to 20%.6,8,15 Many of the leaks improved with conservative treatment; however, on occasions re-exploration and repair was required. 5 We did not have any confirmed bile leaks in our series. One patient had increased bilious output in their drain; however, it quickly decreased postoperatively. It is likely that this represented residual bile in the abdomen after performance of the hepaticojejunostomy.
Small bowel obstruction after laparoscopic CDC has been reported. Lee et al. 5 reported one patient who developed a small bowel obstruction 3 years after the initial operation. An early small bowel obstruction developed in one case report. 19 The authors noted that the jejunojejunostomy was adherent to the mesentery of the colon due to an adhesive band. A potential advantage of performing the jejunojejunostomy intracorporeally is less bowel manipulation and a lower incidence of adhesion formation. One of our patients developed a small bowel obstruction due to migration of the Roux limb through the defect in the transverse mesocolon. Closure of the mesenteric defect is not universally performed after creation of the Roux limb. In this case, closure of the defect was performed, but may have broken down.
Conclusion
We have shown that laparoscopic excision of CDCs is safe. Shorter operative times are possible as experience with this technique develops. The minimal handling of the bowel by performing an intracorporeal jejunojejunostomy may minimize postoperative ileus allows for quicker postoperative feeding and earlier discharge.