
Abstract
Abstract
Introduction:
Vesicoureteral reflux (VUR) represents one of the most significant risk factors for acute pyelonephritis in children. Nephropathy with renal scarring is still the most concerning issue in VUR. Surgical correction to eliminate VUR is an important part of its management and this need is increasing for duplicated collecting systems (DCS). Laparoscopy may have a place in the treatment of VUR. We report our initial experience in the treatment of refluxing DCS by laparoscopic extravesical transperitoneal approach (LETA) following Lich–Gregoir technique. The aim of this study was to describe the evolution and evaluate the results and benefits of this technique.
Materials and Methods:
Between August 2007 and January 2010, 60 renal units in 43 children with VUR and deterioration of renal function on isotope renography were treated with LETA following the Lich–Gregoir procedure. Twelve patients had refluxing DCS in a lower polar system; three of them had bilateral VUR. Three cases of refluxing DCS were associated to obstruction. Two of them presented an ectopic ureterocele with adequate split renal function and another had an ectopic ureterocele with complete deterioration of upper polar renal function. Their mean age was 36 months (range: 15–80 months).
Results:
The mean surgical time was 90 minutes (38–140 minutes) in unilateral and 144 minutes (120–200 minutes) in bilateral VUR including cystoscopy. All procedures were successfully completed laparoscopically and the reflux was corrected in all patients. One-stage laparoscopic heminephroureterectomy with excision of ureterocele and ureteric reimplantation was done in 1 case, and ureterocele excision and ureteric reimplantation by LETA were done in 2 cases. The mean hospital stay was 27 hours. A cystogram was performed systematically in all patients at 45 days postoperatively; none of them presented recurrence of VUR. The follow-up period was 11 months (range: 2–24 months), without recurrence of VUR.
Conclusion:
LETA following the Lich–Gregoir procedure in refluxing DCS is a safe and effective approach even in unilateral, bilateral simultaneous, and split renal function in duplicated systems. When refluxing DCS is associated with obstruction and total deterioration of upper polar function, heminephroureterectomy with excision of ureterocele and ureteric reimplantation can be safely and effectively performed in a single-stage laparoscopic procedure, which minimizes the hazards of traditional open surgical reconstruction. A shorter hospital stay, decreased postoperative discomfort, reduced recovery period, and a low morbidity to resolve VUR in DCS are the benefits of this technique, with success rates similar to the open technique.
Introduction
Laparoscopic antireflux surgery has never achieved popular consensus because of the technical difficulty in dissection and suturing required; however, the efforts have been directed toward reducing the perioperative morbidity period and shorter hospitalization. The minimally invasive surgical approach to VUR disease was first described by Atala et al. in minipigs, 10 and the first report described in humans was in 1994 by Ehrlich et al. 11 Since then, different reports of laparoscopic repair have been described. Few pediatric centers have embraced either the laparoscopic extravesical or vesicoscopic cross-trigonal approaches and the success rates have been comparable to open surgery, with less morbidity in patients with VUR.12–31 We report our initial experience in the treatment of VUR by laparoscopic extravesical transperitoneal approach (LETA) following Lich–Gregoir technique in refluxing duplicated collecting systems (DCS). The aim of this study was to describe the evolution and evaluate the results and benefits of this technique.
Materials and Methods
Between August 2007 and January 2010, 60 renal units in 43 children with VUR and deterioration of renal function on isotope renography were treated with LETA following the Lich–Gregoir procedure. Twelve children (9 girls and 3 boys; mean age: 36 months [5–80 months]) had refluxing DCS in a lower polar system, with three of them having bilateral. VUR was classified by using the international classification as grades I to V: 7 had a preoperative VUR grade III, 4 grade IV, and 1 grade V. Preoperative nuclear renal scans DMSA (dimercaptosuccinic acid) was done in all patients, and a mean renal function of 39% (19%–40%) was found. Two cases presented an ectopic ureterocele with adequate split renal function and another had an ectopic ureterocele with complete deterioration of upper polar renal function. Two of these patients had Hutch diverticulum. The surgical indications according to the American Urology Academy are recurrent acute pyelonephritis under antibiotic prophylaxis and deterioration of renal function on nuclear renal scans DMSA.
Operative Technique
LETA was performed by the transperitoneal approach. Under general anesthesia, cystoscopy was used in these patients to assess the location of the ureteral orifices and to check bladder anatomy. The patient is placed in supine position with the legs apart; a urine catheter is inserted preoperatively. Three ports were used in all cases: a 5-mm 30° port for the telescope and two 3-mm trocars. The surgeon stood at the head of the patient, with the assistant to the left and the nurse to the right. The monitor is placed at the lower end of the table. The telescope is inserted through the transumbilical trocar, the other two 3-mm trocars are placed at the left and right lower abdomen under direct vision (Fig. 1). Stay sutures are used to expose the vesicoureteral junction (VUJ). Two stay sutures are inserted through the abdominal wall and are placed at each side of the bladder to pull up it to the anterior wall and expose the VUJ. The peritoneum is incised to identify the distal ureter that is isolated and dissected toward the VUJ. The ureter is mobilized to achieve sufficient freedom for a tension-free reimplantation. Using the scissors monopolar, the peritoneum is incised to expose the muscular wall of the bladder and create an optimal lateral tunnel about a length four times the size of the ureter (Paquin law). At this moment the bladder is filled partially with physiologic serum to expose and identify the mucosa, to avoid the perforation at the moment of detrusorraphy (Fig. 2). The detrusor muscle and all muscle fibbers are cautiously divided down with scissors until the mucosa is exposed. After completing the dissection, another stay suture is inserted through the abdominal wall and placed around the ureter toward the top of the bladder. The ureter is placed in the newly created tunnel, and the detrusor muscle is reapproximated with three or four separate intracorporeal stitches using absorbable or nonabsorbable suture 3-0 depending on the surgeon. At finish, the ureter is mobilized without tension to avoid ectasia or isquemia, and the urine catheter is removed (Fig. 3).

Trocars position.

Detrusorraphy and exposing the mucosa.
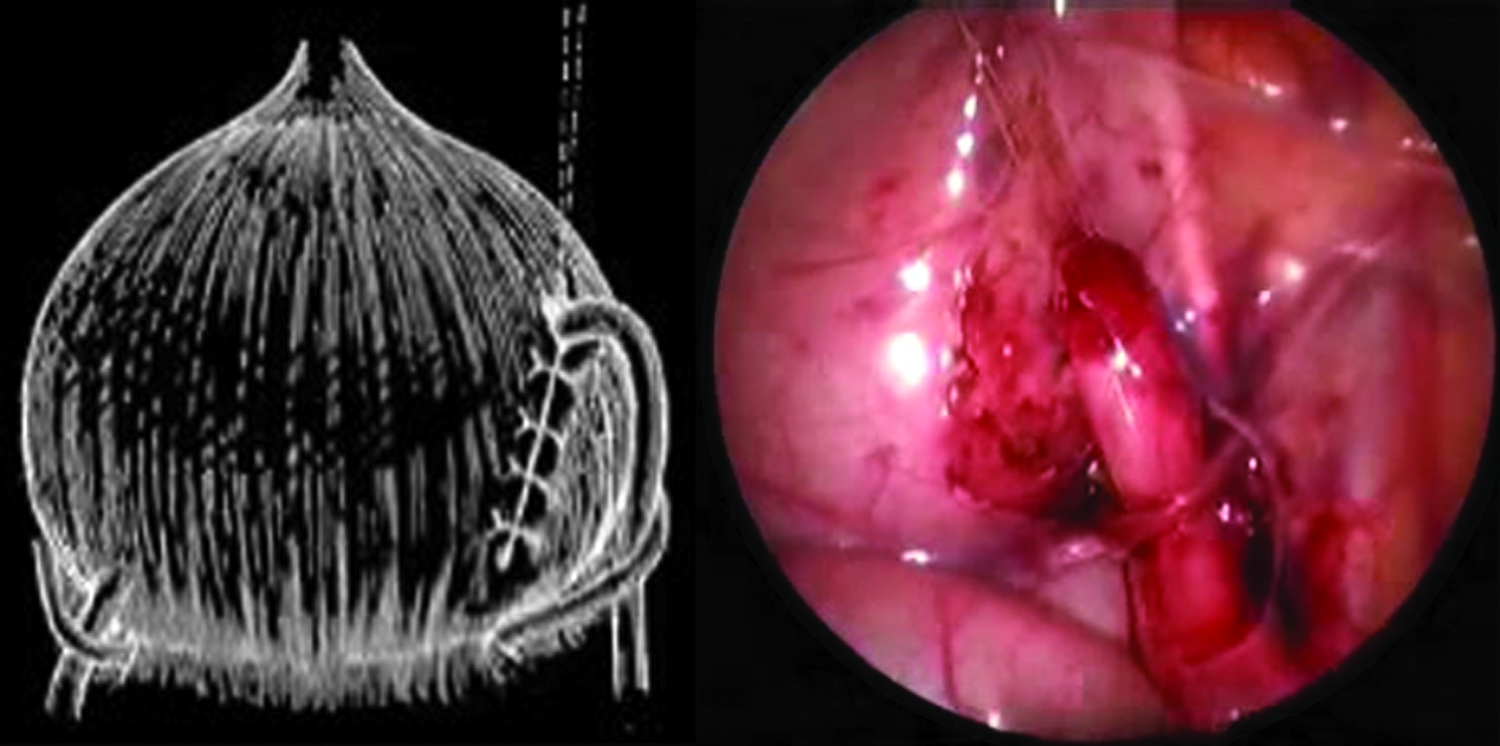
Vesicoureteral reimplantation.
Results
LETA following the Lich–Gregoir procedure was feasible in all 12 patients, and all 15 ureters were successfully reimplanted by LETA. Three of them had bilateral VUR and were repaired in a single procedure.
The mean surgical time was 90 minutes (58–140 minutes) in unilateral and 144 minutes (120–200 minutes) in bilateral VUR including cystoscopy. All procedures were successfully completed laparoscopically and the reflux was corrected in all patients. One-stage laparoscopic upper pole heminephroureterectomy with excision of ureterocele and ureteric reimplantation was done in 1 case, and in 2 cases, the ureterocele excision was done with a 3F Bug-bee using the cutting current at a level high enough to ensure a clean puncture, before starting the reimplantation. In 2 cases, refluxing DCS was associated with a paraureteral diverticulum; at the moment of reimplantation, the diverticulum was carefully reinforced to provide a secure back wall.
The mean hospital stay was 28 hours (22–48 hours). A fluoroscopic voiding cystogram and renal ultrasonography were performed systematically in all patients at 45 days postoperatively; none of them presented recurrence of VUR. The Hutch diverticulums were resolved after surgery. The follow-up period was 11 months (range: 2–24 months) after the postoperative cystogram, with clinical evaluation and ultrasonography systematic control at 3 months, 6 months, 1 year, and 2 years. A fluoroscopic voiding cystogram was performed again only in cases of recurrence of urinary tract infection. All patients were asymptomatic without urinary tract infection.
Discussion
VUR is the most common urologic anomaly in children and represents one of the most significant risk factors for acute pyelonephritis in children. Nephropathy with renal scarring is still the most concerning issue in VUR. Surgical correction to eliminate VUR is an important part of its management. 1 The DCS, present in 0.8% of the general population, is more common in female individuals. The ureter draining the upper segment may migrate too far caudally and become ectopic and obstructed, whereas the ureter draining the lower segment may end laterally and have a short intravesical tunnel that leads to VUR. 17 VUR is the most frequent clinical problem in DCS and involves the lower pole in 95% of cases. 18 Conservative treatment, the most accurate study currently available, found significantly lower-resolution rates in DCS than in simple system and resolution of high-grade VUR is reported as uniformly rare in DCS.
The management of VUR continues to evolve. Endoscopic correction of VUR is a reasonable alternative to open surgical reimplantation, particularly in cases of low grade, although long-term results into adulthood remain unknown; however, the success rate is lower in patients with refluxing DCS. 19
In 2008, Callaghan presented the factor involved in parenteral decision making for surgical correction of VUR and considered that the parents selecting open surgery consider the success of the procedure most important, and the majorities are satisfied with their choice of treatment. Parents choosing endoscopic correction consider the minimally invasive nature of the procedure and the success rate most important, but the outcome may alter their satisfaction. 20
The spectrum of urology pediatric laparoscopy has undergone a dramatic evolution. Initially used as a diagnostic tool, laparoscopically complex and reconstructive procedures are now performed. Different techniques of VUR demonstrating feasibility with pneumovesicoscopic, laparoscopic, and robot-assisted techniques are encouraging and have been reported to be beneficial in terms of decreased postoperative pain, shorter hospital stay, and quicker return to normal activity. 21 Extravesical reimplantation and laparoscopic Cohen technique were the most commonly performed with a high success rate.
The Lich–Gregoir technique was simultaneously developed and described by Lich in 1961 and Gregoir in 1964.22,23 This technique is an extravesical procedure and has the following advantages: minimal bladder spasm, less morbidity because the bladder remains intact, no hematuria, and no anastomosis. Additionally, decreased hospital stay with faster recovery makes it a potential 1-day surgery.15–25 The Lich–Gregoir technique is associated with a high success rate as the Cohen technique.
In open surgery, the Lich–Gregoir technique has been associated with incidence of urinary retention for bilateral reimplantation and impaired voiding efficiency. These are the common complications of this technique, ranging from 3% to 20%.26,27 The cause might be a result of neurovascular injury during wound handling and ureteral or bladder dissection. 28 However, in open surgery, Mc Achran in 2005 demonstrated that bilateral extravesical ureteroneocystostomy can be performed in selected patients without postoperative urinary retention, with uniform hospital discharge in 1 day. 15 In 2008 and 2009, Palmer demonstrated that unilateral and bilateral extravesical ureteral reimplantation can consistently result in same day discharge from the hospital without postoperative urinary retention.16–25 The minimal invasive technique is associated with less morbidity owing to less tissue and nerve injury and can be handled in an outpatient setting.
One of the advantages of LETA with open surgery is in cases when the refluxing DCS is associated with either obstruction or VUR or both, as these conditions may cause upper tract damage. Surgical procedures may involve upper or lower tract manipulation or a combination of both and can be performed in one stage. In our series, in 3 of 12 patients, refluxing DCS was associated with obstruction; 2 had ectopic intravesical ureterocele with adequate split renal function and 1 had ectopic intravesical ureterocele with complete deterioration of upper polar rein function. In 1 case, upper heminephroureterectomy with excision of ureterocele and ureteric reimplantation was done in one-stage laparoscopy, and in 2 cases, only excision of ureterocele and ureteric reimplantation were done laparoscopically. Yeung in the 2007 ESPU meeting reported that laparoscopic heminephroureterectomy with excision of ureterocele and ureteric reimplantation can be safely and effectively performed in a single-stage laparoscopic procedure. The procedure minimizes the hazards of traditional open surgical reconstruction in patients with refluxing DCS associated with ureterocele and complete deterioration of upper polar function and VUR. 29 Careful selection of operative candidates is necessary. It has been speculated that ureters requiring tapering are unsuitable for Lich–Gregoir technique by laparoscopic approach; however, Ansari in 2006 described an extracorporeal tailoring for megaureter to perform LETA following Lich–Gregoir technique with good results. 30
Based on the results in this preliminary series, the authors believe that LETA following the Lich–Gregoir technique for refluxing DCS is a safe, effective, and feasible procedure with good results. In some cases, when refluxing DCS is associated with obstruction and upper tract damage, radical definitive surgery can be safely and effectively performed in a single laparoscopic procedure, with good short-term results.
With our technique, excellent results comparable to those of established open procedures were achieved: a low morbidity to resolve the VUR, decreased postoperative discomfort, shorter hospital stay, good cosmetic results, and reduced recovery period. LETA following Lich–Gregoir technique is easy to perform even for refluxing DCS, unilateral, and bilateral simultaneous. In most cases, LETA is not associated with bladder dysfunction as in an open surgery, even in bilateral procedures. In fact, we believe that this procedure is technically reproducible for young surgeons in laparoscopic and urological training. Our experience with LETA, and many laparoscopic and urological procedures to date, allowed our learning curve to plateau after 6–7 cases, and our operative time decreased significantly after 6 cases. We still make a videorecording of all of our procedures not only for use as a learning tool by our residents and fellow, but also to allow the surgeons to be critical of their technique and permit further improvement. Minimal invasive surgery is an alternative to open procedure and not to medical treatment, especially in patients with nephropathy with renal scarring. We believe that this procedure will become an established treatment option.
Footnotes
Disclosure Statement
No competing financial interests exist.