
Abstract
Abstract
Objective:
Laparoscopy is an alternative procedure for pediatric inguinal hernia, with a trend toward increasing use of extracorporeal knotting and decreasing use of working ports. The aim of this study was to evaluate the preliminary results of one-trocar laparoscopic herniorrhaphy in infants and children.
Methods:
Between April 2007 and March 2010, 216 infants and children treated were retrospectively reviewed. Under laparoscopic guidance, the hernia defect was closed extracorporeally by a nonabsorbable suture, which was introduced into the abdomen by an 18-gauge vascular access on one side of the hernia defect and withdrawn on the opposite side by a homemade hook-pin through a stab incision. Preperitoneal hydrodissection was performed during the procedure. Being a developing technique, multiple linear regressions were used to model markers for the operating time, including descriptive data, diameter of scope, operation findings, and the procedural volume.
Results:
A total of 308 procedures were successfully performed among 214 patients (99.1%) and the mean operating time was 42.9 ± 24.7 minutes (range: 9–255 minutes). Additional working instruments were necessary in 7 patients (3.3%). Only 2 (0.9%) recurrences were observed during this period. Male gender (β = 7.507, P = .001), prematurity (β = 10.051, P = .004), presence of incarcerated hernia (β = 12.188, P = .016), and both sides simultaneous operation (β = 7.057, P = .001) would increase the operating time, while being independent of age, weight, presence of sliding hernia, and diameter of scope. However, the operating time may decrease with procedural volume (β = −0.119, P < .001).
Conclusions:
Without assistant working instrument, laparoscopy-assisted extracorporeal ligation of the hernia defect may be safely performed in most infants and children. The use of preperitoneal hydrodissection and extraperitoneal knot-tying could tautly enclose the hernia defect without peritoneal gaps and approach an accepted recurrence rate.
Introduction
However, there are some technical limitations, although modifications on laparoscopic surgery continue to be refined. The known limitations of the laparoscopic surgery are as follows: (1) Most of these methods employ a laparoscope inserted via an umbilical incision and two lateral ports for instruments to ligate the hernia defect. 4 The necessity for intra-abdominal skills, such as intracorporeal suturing, knot-tying, and manipulation of the suture on a needle, may be time-consuming and cumbersome. 5 (2) In fact, compared with open herniotomy with an almost disappeared wound in the skin crease, laparoscopic approach did not take any superiority in cosmesis. Conversely, the procedure was thought not to be a minimally invasive surgery because of the necessity of multiple skin incisions and pneumoperitoneum during operation. In a single-blinded, randomized study, recovery and outcome were similar after open and three-port laparoscopic hernia repair in children. 6 Moreover, three-port laparoscopic approach was associated with increased operative time and postoperative pain. 6
Therefore, further development in minimal access surgery for pediatric inguinal hernia is to decrease the number and size of skin incisions. With a trend toward increasing use of extracorporeal knotting and decreasing use of working ports and endoscopic instruments, 3 single-port endoscopy-assisted percutaneous extraperitoneal closure with variable devices is the attainment.5,7,8 Recently, we have developed a modified technique for one-trocar laparoscopic percutaneous transperitoneal closure of pediatric inguinal hernias, using a simple homemade hook-pin and vascular access. 9 Herein, the author describes the preliminary results of the novel methods in a 3-year experience.
Patients and Methods
Between April 2007 and March 2010, a total of 221 consecutive infants and children who were enrolled for the purpose of solving the inguinal hernia problem were reviewed retrospectively. Of the 221 children, 5 patients were excluded. One 10-year-old boy presented with direct-type inguinal hernia, and two additional working ports were necessary to facilitate closure of the defect. 10 In one 6-month-old boy presenting with incarcerated inguinal hernia, laparoscopic reduction was unsuccessful and open laparotomy was necessary to facilitate reduction. The remaining 3 patients (5-year-old boy, 6-year-old girl, and 7-year-old girl) were initially diagnosed as having inguinal hernia, but negative hernias were noted during laparoscopy. Magnetic resonance imaging was investigated for the 3 children. Spermatic cord lipoma was identified in the boy, whereas asymmetric labium majus enlargement was diagnosed in the 2 girls.11,12 No further groin exploration was performed.
Surgical technique
The initial surgical technique was presented in 2008, and it remains the same. 9 All the operative procedures were done by the first author. Under laparoscopic guidance (5-mm laparoscope or 3-mm needlescope), the hernia defect was enclosed by a nonabsorbable suture, which was introduced percutaneously at the corresponding skin of the orifice of the hernia defect by an 18F vascular catheter (Surflash I.V. catheter, I.D. 0.95 × 64 mm; Terumo Corporation, Tokyo, Japan) on one side of the hernia defect and withdrawn on the opposite side by a hooked pin, which was made by an orthopedic pin (I.D. 1.8 mm, MES-CF01-063-21; Mizuho, Tokyo, Japan), through one needle puncture wound. The suture was then tied extracorporeally to obliterate the hernia sac. During the procedure, 5–8 mL of isotonic saline was infused percutaneously via the vascular catheter into the preperitoneal space to obtain the preperitoneal dissection of the hernia defect (Fig. 1).
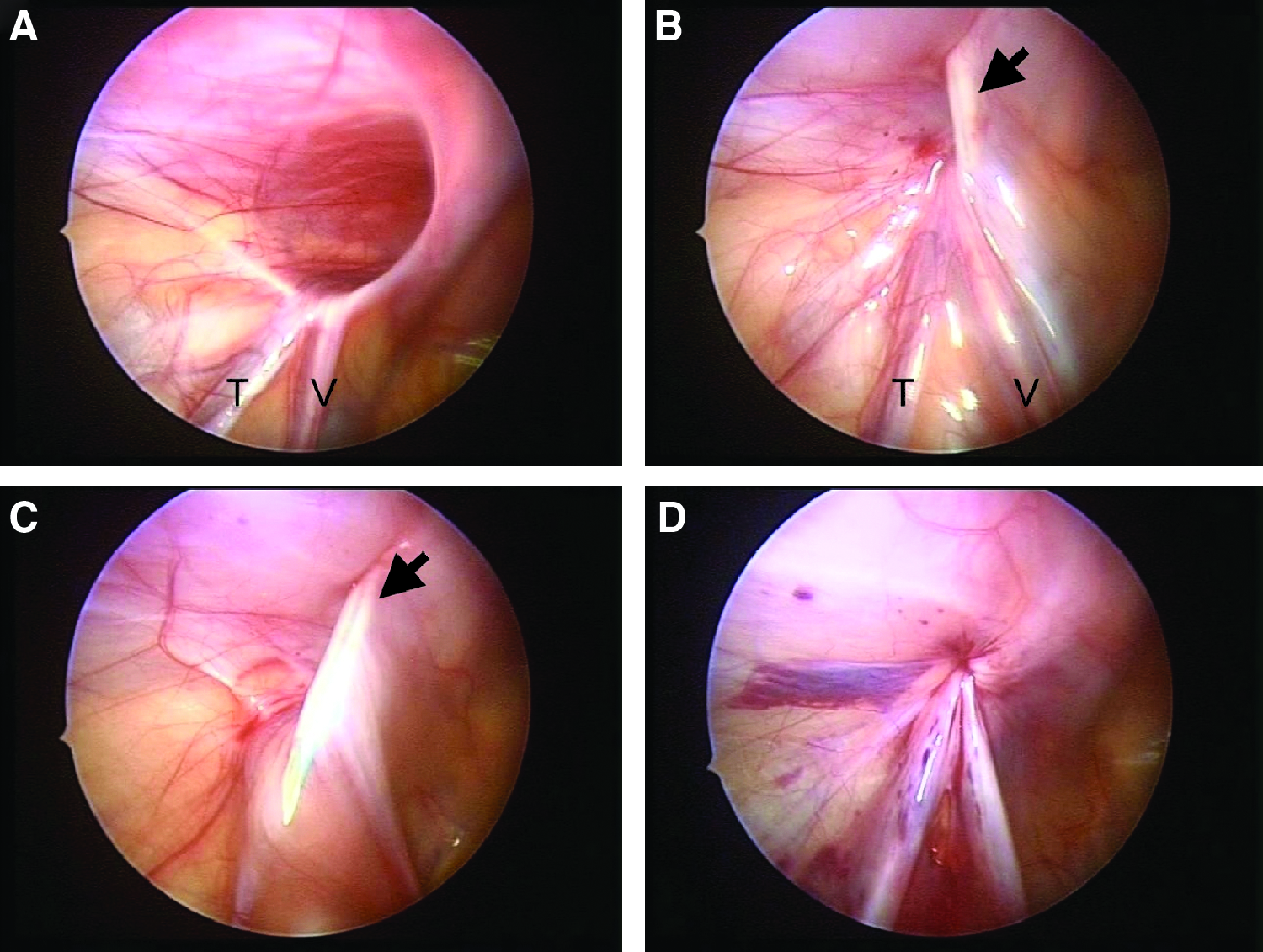
Intraoperative photograph showing a 4-year-old boy receiving the procedure. (
Data collection and statistical analysis
Case patients were analyzed for their descriptive variables (age at operation, body weight, prematurity, and gender) and perioperative data by reviewing their medical charts. Before beginning our analysis, the available literature was reviewed to identify factors thought to be important for the operating time of the developing procedure. Student's t-tests and χ2 tests were used to compare continuous and categorical descriptive variables, respectively. Univariate and multivariate linear regression analyses were used to examine the factors influencing the operating time. Potential confounders such as patient age, gender, prematurity, body weight, diameter of scope, and perioperative findings were adjusted in all multivariable analyses. Results were expressed as mean with standard deviation or effect and 95% confidence interval where appropriate. A P value of <0.05 denoted statistical significance. SPSS for Windows 12.0 was used for all statistics.
Results
Of the 216 children, there were 139 boys and 77 girls with a mean age of 3.45 ± 3.8 years (range: 9 days to 21 years). Right-sided inguinal hernia was present in 98 patients, left-sided in 98, and bilateral in 20. The mean body weight was 14.3 ± 11.6 kg (range: 2–77 kg).
The procedure was successfully performed 308 times in 214 patients (99.1%). Two patients (0.9%) failed in the procedure. In one 80-day-old male infant (2 kg), approach to the hernia defect intraperitoneally was a failure because of limited working space, and he was converted to the open approach. In another 13-day-old male infant (2.77 kg), the friable peritoneum of the orifice was cut through by the enclosing suture during extracorporeal knot-tying after immediate reduction of the incarcerated hernia, and the hernia defect was closed by N-shaped sutures with an assistant working port.
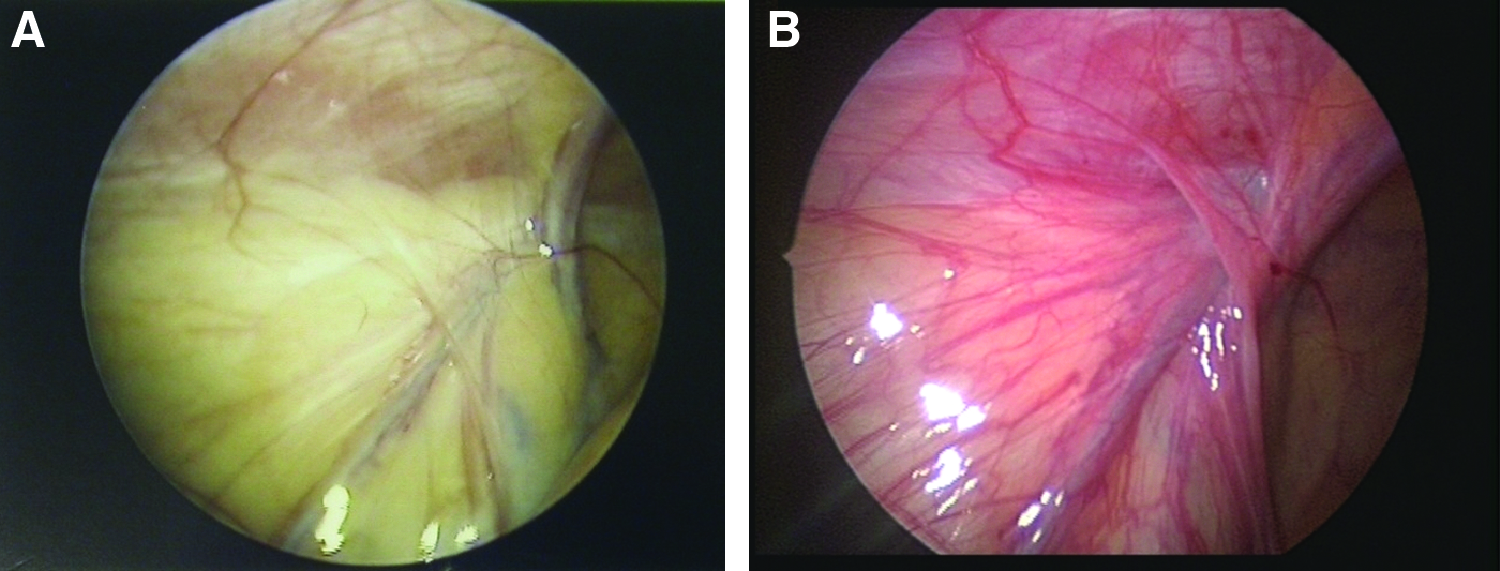
Nine patients (4.2%) suffered from metachronous hernias from a previous approach on the other side, including conventional open herniotomy in 8 and laparoscopy in 1 patient. One 9 years old suffered recurrent hernia from open herniotomy 47 days previously (Fig. 2). Nine patients (4.2%) presented with an incarcerated hernia, and 3 of them required emergency operation because of failure of manual reduction under sedation.

Laparoscopic views showing right-side recurrent hernia after open herniotomy in a 9-year-old boy (
During operation, sliding hernia was found in 15 patients (6.9%), including omentum in 2, fallopian tubes in 12, and Amyand's hernia in 1 patient. Contralateral patent processus vaginalis was present in 74 patients (34.3%). Unrelated procedures performed at the same time included umbilical hernia in 22 patients, circumcision in 11, left posterior auricular dermoid cyst in 1, removal of bilateral myringotomy ventilation tubes for acute otitis media in 1, left arm keloid in 1, simple frenectomy in 1, incidental appendectomy in 1, and an unexpected left ovarian teratoma in 1 patient. Additional working instruments were necessary in 7 patients (3.3%), including incarcerated hernia in 2, sliding hernia in 3, appendectomy in 1, and the teratoma in 1 patient. There was no serious intraoperative complication. Unintentional preperitoneal pneumodissection during insufflation, which may disturb the procedure and obstruct contralateral patent processus vaginalis, occurred in 6 patients (2.8%). Retroperitoneal hematoma during operation was noted in 7 patients (3.3%) during operation and was resolved with observation. Disruption of the enclosing suture during extracorporeal knot-tying occurred in 7 patients (3.3%) and repeat ligation of the defects was required.
Recurrence occurred in 2 patients (0.9%) and the time to hernia recurrence was 43 and 161 days, respectively. Stitches abscess or granuloma at the suture site occurred in 4 patients (1.9%), and all were treated with removal of the stitch and oral antibiotics.
Being a developing procedure, factors influencing the operating time were analyzed and the results are shown in Table 1. One hundred seventy-four patients without unrelated operations were enrolled. In the univariate analysis, the operating time was directly related to male gender, prematurity, presence of incarcerated hernia, and both sides simultaneous operation, while being independent of age, weight, presence of sliding hernia, and diameter of scope. In the multivariate analysis, the operating time was significantly directly related to male gender, prematurity, presence of incarcerated hernia, and simultaneous operation on both sides of inguinal hernias (P = .001, .004, .016, and .001). However, the operating time was significantly inversely related to the procedural volume in the univariate and multivariate analyses (β = −0.132, P < .001; β = −0.119, P < .001).
CI, confidence interval.
Discussion
In a large series of 6361 pediatric inguinal hernias over a 35-year period treated with open herniotomy, only 1 boy did not have a hernia and 4 girls had labial lipomas (presenting as an indirect inguinal hernia). 1 However, up to 1.2% of infants and children with preoperative diagnosis of inguinal hernia presented as negative hernias during laparoscopy in the 3-year study. This may be explained by few case numbers and the short period of this retrospective review. Notwithstanding, laparoscopic approach exempted unnecessary dissection of the spermatic cord if negative hernias occurred at the time of surgery. Moreover, an unexpected intra-abdominal lesion, such as ovarian teratoma in the present series, may be found during laparoscopy.
Pneumoperitoneum may help to widen the internal ring 13 and further facilitate reduction of incarcerated hernia during laparoscopy. In the series, 5 patients with incarcerated inguinal hernia failed in manual reduction under sedation. Emergency operations were performed, and a laparoscopic approach was elected. Laparoscopic reduction was successful in 4 patients and one additional working instrument was necessary in 2 of them. Pneumoperitoneum may also help to explore contralateral defects. However, in the present series, a 3-year-old boy presented with metachronous left hernia at 119 days after a previous laparoscopic approach (Fig. 3). The authors would propose that an obliterated processus vaginalis might open again when there is adequate intra-abdominal pressure.
A 3-year-old boy receiving the method. (
In the standard three-port technique with intracorporeal knot-tying or the two-port technique with an assistant port for intra-abdominal suturing, the hernia defect is always closed by N-shaped or purse-string sutures, both of which cannot enclose the defect completely and may leave multiple peritoneal gaps. The resultant peritoneal gaps cannot provide adequate peritoneal injury and may disturb or defer further peritoneal adhesion if the knot-tying is loosening gradually, leading to potential recurrence. 3 The author suggests complete extraperitoneal enclosing of the hernia defect could decrease peritoneal gaps, and single-port endoscopy-assisted percutaneous extraperitoneal closure may be the preferred technique. Moreover, in the single-port technique, the ligation of the hernia defect could be achieved percutaneously without the need for intracorporeal manipulation of the needle and knot-tying.
To completely enclose suturing of the hernia defect without any gap in the single-port technique, preperitoneal hydrodissection must be the main step. The concept of hydrodissection during laparoscopic hernia repair has been already described in the literature. 14 In 2007, Chan and colleagues employed preperitoneal hydrodissection in the three-port intraperitoneal-suturing technique and concluded that the recurrence rate could decrease from 4.88% to 0.4% after the usage of preperitoneal hydrodissection. 14 Recently, the method of preperitoneal hydrodissection has been applied in the single-port technique.5,9 With the aid of hydrodissection, the vas and vessels could be separated from the peritoneum; therefore, a completely enclosing suture of the hernia defect could be provided without any gaps.5,9 From the above conception, only 2 (0.9%) recurrences were observed in the present series. In 1 case of recurrence reoperated by the same technique, the suture was not found, which may indicate that the reason for the recurrence was a technique mistake and not the technique itself (Fig. 2).
Also, the method of preperitoneal hydrodissection was useful in (i) providing additional space for negotiating the working instruments; (ii) keeping the device just under the peritoneum, and observing the needle sign 7 ; (iii) avoiding injury to the vas and vessels; (iv) making a further airtight extracorporeal knot-tying 14 ; and (v) decreasing postoperative hydrocele, which may be caused by interruption of testicular lymphatic drainage because of being thicker than the peritoneum bites of the encircling suture. 5 Moreover, normal saline, the solution for preperitoneal hydrodissection, could predispose the formation of peritoneal adhesions and fibrosis. 15 Therefore, during passing of the suture, preperitoneal normal saline injection may cause more tissue trauma, further promoting the formation of peritoneal adhesions and minimizing later recurrence.
Schier suggests that laparoscopic hernia repair in small babies is a less technically demanding procedure than primary inguinal herniotomy. 16 In the present series, 55 of the children (25.5%) weighed below 5 kg and the median weight at surgery was 3.12 kg (range: 2–5 kg). Two of the 55 patients (3.6%) failed in the procedure. Although the present method may be time-consuming in small infants (P = .003), small babies usually receive more unrelated operations (mostly umbilical hernia) and simultaneous operations on both sides of inguinal hernias than those weighing >5 kg (P < .001) (Table 2). Besides, body weight is unrelated to the operating time in multivariate analysis (β = −0.119, P < .001). The present series confirms Schier's assumption that laparoscopic hernia repair could be successfully and safely performed in most infants and children, regardless of age and body weight.
The operating time usually represents complexity of technical skill and familiarity of the procedure in an individual surgeon. 17 In the present series, male gender, prematurity, and presence of incarceration were time-demanding in the multivariate analysis. However, the operating time may decrease with increased individual procedural volume (β = −0.119, P < .001).
Some surgeons perform a very similar hernia repair with the addition of introducing an extra grasping instrument through the umbilicus alongside the telescope, providing an addition instrument to assist with the hernia sac purse-string suture. In the series, additional working instruments were necessary in some complicated inguinal hernias, including incarcerated hernias in 3, sliding hernias in 3, and unrelated operations (appendix and teratoma) in 2. In the early periods of the developing technique, additional working ports were always placed on the lateral abdominal wall. In the last 3 cases, all instruments and camera could be inserted through the same umbilical incision, which could provide better cosmetics and reach the state of minimally invasive surgery. 18
A number of drawbacks in the present series have been identified. First, compared with traditional inguinal herniotomy, the present study of a small number of patients examined the practice at only a single facility and the follow-up period was too short to make any conclusion about only a few complications of the technique. More long-term follow-up of the treatment modality is necessary. Second, as only 25 of the infants (11.6%) weighed below 3 kg and none weighed below 2 kg, the evidence for the effectiveness and safety of the technique for any age and weight needs to be further evaluated.
Conclusion
One-trocar laparoscopy-assisted extracorporeal ligation of inguinal hernia could be successfully and safely performed in most infants and children. Although additional working instruments were necessary in rare situations, single umbilical incision laparoscopic surgery appeared to be a feasible and safe technique for the treatment of complicated inguinal hernia in the pediatric setting. The smaller and fewer skin incisions of the single-port technique could reach the state of minimally invasive surgery. Preperitoneal hydrodissection could avoid trauma to the cord structures, completely enclose the hernia defect without peritoneal gaps, provide a further tensionless extracorporeal knot-tying, and approach an accepted recurrence rate similar to that of the established open technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
An abstract (ID: 26568) of this article was presented as a loop video poster in the 19th Annual Congress of the International Pediatric Endosurgery Group, June 8–12, 2010, Hawaii.