
Abstract
Abstract
Introduction:
Single-incision pediatric endosurgery is gaining popularity in children. We have recently applied the single-incision approach for thoracoscopic procedures. We report our initial experience with single-incision thoracoscopic surgery in the pediatric population.
Methods:
A retrospective chart review of the first 10 single-incision thoracoscopic operations done at our institution was conducted. The patients' mean age and weight and the median operative time, postoperative length of stay, and time until discontinuation of chest tubes were determined.
Results:
The 10 procedures were performed in eight patients (two patients each had bilateral procedures). The procedures performed included wedge resection and mechanical pleurodesis for spontaneous pneumothorax (n = 7), wedge biopsies for lymphoma (n = 1) and chronic granulomatous disease (n = 1), and resection of an apical extrapulmonary neuroblastoma (n = 1). All of the procedures were completed without intraoperative complication or significant blood loss. In each case, multiple trocars and/or unsheathed instruments were passed through a single small incision, which was subsequently used for the chest tube(s). The mean patient age was 13.5 years (range 3–18 years). The mean weight was 47 kilograms (range 16–63 kg). The median operative time was 64 minutes (range 50–201 minutes). The median postoperative length of stay was 7 days (range 3–19 days). The median time until chest tube removal was 3 days (range 2–15 days). The mean follow-up was 7 months (range 3–12 months). One patient developed a recurrent pneumothorax and persistent air leak after having undergone a wedge resection and pleurodesis for a spontaneous pneumothorax and required a reoperation.
Conclusion:
Single-incision thoracoscopic surgery is a feasible alternative to the traditional multiple-incision approach in the pediatric population. The in-line positioning of the camera and instruments often proves to be an advantage rather than a hindrance.
Introduction
The technique for single-incision thoracoscopic procedures has been reported in the adult literature.9,10 However, experience in children remains extremely limited. We have recently applied the single-incision approach to a variety of pediatric thoracic conditions. We report our initial experience with single-incision thoracoscopic surgery (SITS) in the pediatric population.
Materials and Methods
With approval from the institutional review board, a retrospective chart review of the first 10 single-incision thoracoscopic operations done at a single institution (St. Christopher's Hospital for Children, Philadelphia, PA) was conducted. These initial procedures were performed over a 10-month period of time (November, 2008–August, 2009).
Informed consent was obtained for each patient. The discussion included details of the potential risks and benefits of open surgery versus traditional multiple-incision thoracoscopy versus a single-incision thoracoscopic approach. Once consent was obtained, each patient was prepared for the operating room. After the induction of general double-lumen endotracheal tube anesthesia, each patient was placed in the lateral decubitus position and properly padded. A single, small incision (∼2.5–3 cm) was made obliquely at the anticipated chest tube site within a rib interspace (Fig. 1). Two trocars (either two 5 mm or one 5 mm and one 12 mm) were placed, and one unsheathed 3 or 5 mm instrument was passed adjacent to the trocars directly through the intercostal muscles. This array allowed for visualization with a 5 mm thoracoscope and tissue manipulation with two instruments. Wedge resections of the lung were performed with an endoscopic stapling device passed through the 12 mm trocar (Fig. 2). In patients undergoing the procedure for spontaneous pneumothorax, a mechanical pleurodesis was performed with a cautery tip scratch pad. One or two chest tubes were left through the trocar site(s).

A 12 mm trocar, a 5 mm trocar, and an unsheathed grasper passed through a single 2.5 cm thoracic incision that is obliquely oriented in the rib interspace.
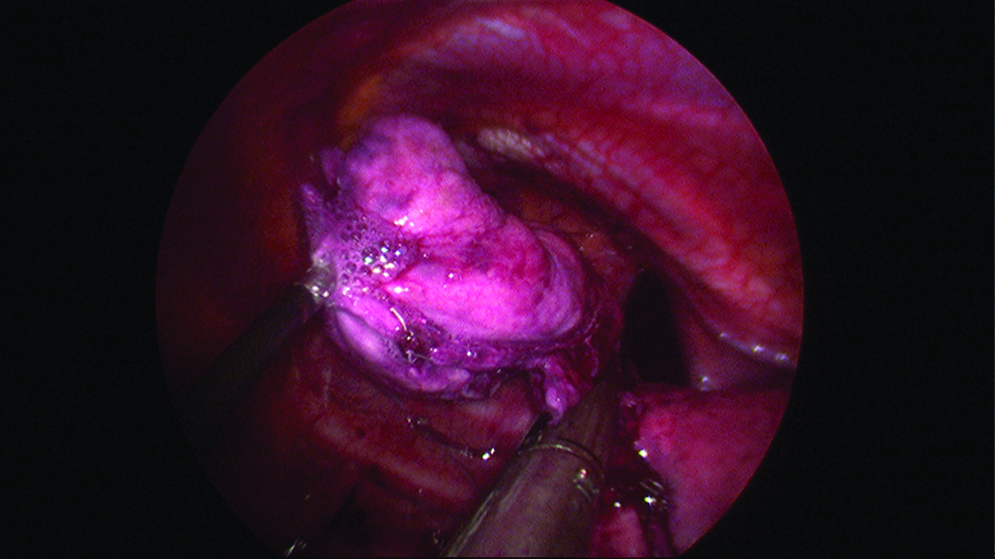
An apical pulmonary wedge resection being completed with an endoscopic stapler.
Data collected included the diagnosis and corresponding procedure performed. The patients' mean age and weight as well as the median operative time, postoperative length of stay, and time until discontinuation of chest tubes were determined. Any complication was noted.
Results
The 10 procedures were performed in eight patients (two patients each had bilateral procedures done under different anesthetics). The operations performed included wedge resection and mechanical pleurodesis for spontaneous pneumothorax (n = 7), wedge biopsies for lymphoma (n = 1) and chronic granulomatous disease (n = 1), and resection of an apical extrapulmonary neuroblastoma (n = 1). All of the procedures were completed without intraoperative complication or significant blood loss. The mean patient age was 13.5 years (range 3–18 years). The mean weight was 47 kg (range 16–63 kg). The median operative time was 64 minutes (range 50–201 minutes). The median postoperative length of stay was 7 days (range 3–19 days). The median time until chest tube removal was 3 days (range 2–15 days). The mean follow up was 7 months (range 3–12 months). One postoperative complication occurred. After initially doing well and after chest tube removal, this patient developed a recurrent pneumothorax and persistent air leak after having undergone a wedge resection and mechanical pleurodesis for a spontaneous pneumothorax. The patient required a reoperation and ultimately did well. His final pathologic and microbiologic diagnoses revealed an occult aspergillus infection within the apex of the lung that included the bullae, suggesting an underlying immunologic disorder and raising the possibility of this condition having contributed to his complication.
Discussion
Single-incision surgery is rapidly gaining popularity, particularly for abdominal operations. Both laparoscopic and thoracoscopic techniques have been reported in adults.1–4,9,10 More recently, single-incision pediatric endosurgery has been applied to a variety of conditions in children.5–8 However, experience with SITS in children who have thoracic pathology remains limited as evidenced by the paucity of pediatric cases in the literature. Some of the series in the adult literature include adolescents.11,12 However, there are no reports of this technique being performed in young children. The youngest patient in our series, in whom we resected an apical neuroblastoma, was 3 years old. This operation was the lengthiest in our series (201 minutes), but it was completed without complication and without the need to make additional incisions or convert to an open thoracotomy. Overall in our series, the patient age and weight range was broad indicating that this technique is feasible in both young children and adolescents.
Seventy percent (7 of 10) of the cases performed in our initial series was for the management of primary spontaneous pneumothorax and associated bullous disease. This condition usually occurs in thin adolescents, and boys are more often affected than girls (estimated to be 7.4–18/100,000 versus 1.2–6/100,000, respectively).13,14 The occurrence of these pneumothoraces may be related to the rapid increase in the vertical thoracic dimension in comparison to the horizontal dimension that occurs during growth spurts. An increase in negative pressure at the lung apex may lead to the formation of subpleural bullae that may subsequently rupture, causing a spontaneous pneumothorax 15 (Fig. 3). The treatment of an initial pneumothorax has traditionally been non-operative with observation, supplemental oxygenation, and possible needle aspiration or tube thoracostomy. 16 Operative intervention is generally reserved for patients who have a recurrence, a persistent pneumothorax or air leak, and/or large bullae. Since initially reported in 1986, thoracoscopy with multiple-incision sites has become the surgical standard of care for the treatment of primary spontaneous pneumothorax in both the adult and pediatric populations.17,18 Postoperative pain, postoperative respiratory function, cosmesis, and patient satisfaction are all superior with the thoracoscopic approach as compared with an open thoracotomy.19–21 Long term follow-up, however, has revealed that the minimally invasive approach is not without complications, as up to one half of patients have complaints of chest wall paresthesias and one third of patients experience chronic thoracic wall pain.22,23
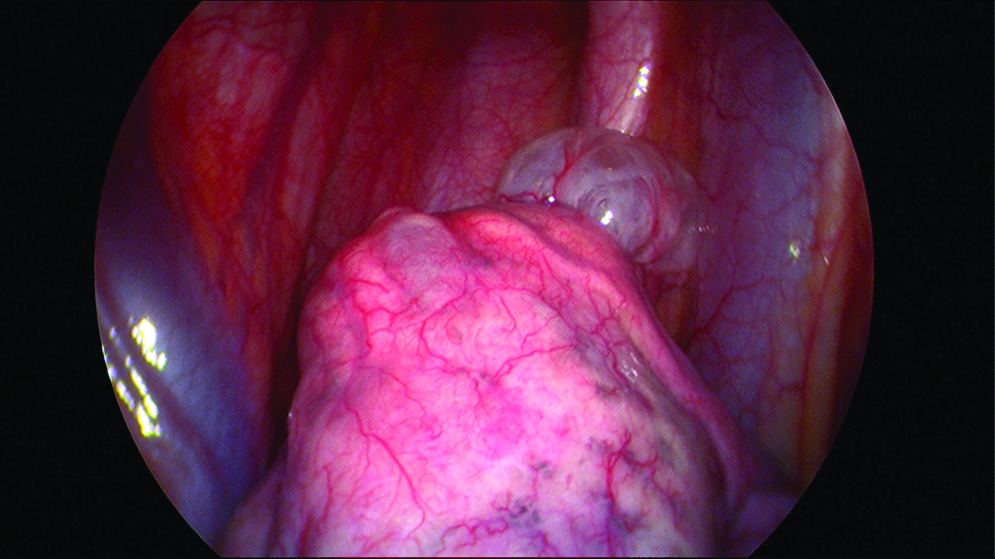
An apical pulmonary bulla in a patient who had a spontaneous pneumothorax.
Recent reports in the adult literature have demonstrated the safety and efficacy of a single-incision thoracoscopic approach for the management of primary spontaneous pneumothorax.11,12 Initial results have revealed decreased postoperative paresthesias, initial postoperative pain scales, and chronic pain in single-incision versus standard multiple-incision thoracoscopy. 11 Salati et al. reported equivalent surgical costs and a decrease in total hospital costs because of a shorter postoperative length of stay. 12 In our series, the single postoperative complication that occurred was a recurrent pneumothorax and persistent air leak after a wedge resection and pleurodesis in a patient initially operated on for a primary spontaneous pneumothorax. The patient had initially done well after the operation and was discharged home after chest tube removal. The final cultures from the resected specimen, however, revealed an aspergillus infection, suggesting that the patient had an occult immunodeficiency and that the staple line may have dehisced due to the infection rather than a technical reason.
Our initial experience demonstrates that SITS is a feasible technique for the surgical management of a variety of thoracic conditions in the pediatric population. In contrast to the conventional multiple-site approach in which the instruments and telescope approach the tissues in differing planes, the in-line positioning of the thoracoscope, grasper(s), and endoscopic stapler in SITS can be an advantage. Further, the procedures in our series were performed with the same instruments and trocars used in traditional multiple-incision thoracoscopy, and so no additional costs were incurred.
Conclusion
We view SITS as the natural next step in the evolution of pediatric thoracic surgery. Further experience, long-term follow-up, and more critical evaluation with prospective randomized trials are necessary to evaluate SITS in the pediatric population.
Footnotes
Disclosure Statement
No competing financial interests exist.