
Abstract
Abstract
Purpose:
The purpose of this prospective study was to evaluate the efficiency, feasibility, and surgical outcomes of microlaparoscopy-assisted pull-through (MAPT) for Hirschsprung's disease.
Methods:
Starting in 2005, pull-through procedures for Hirschsprung's disease were performed exclusively using 2-mm instruments and miniscopes (microlaparoscopy). Three miniports were inserted laterally in the right abdominal wall in one line, with the miniscope at the level of the umbilicus and the working trocars cranially/caudally of the scope. The left colon was dissected, and transanal pull-through was performed.
Results:
MAPT was performed in 16 children (10 boys and 6 girls; average age: 5.7 months). Six patients had previous abdominal surgeries. A 1.9-mm cystoscope or a 2.4-mm arthroscope was used in the first 5 cases. In the remainder, a recently developed 2.4-mm miniscope was used for visualization. The length of the resected colon segment was up to the left colonic flexur in 5 children, up to the middle of the descending colon in 4 cases and up to the sigmoid-descending segment in 7 children. The average operation time was 185 minutes (range: 120–330 minutes). The only intraoperative complication that occurred was an injury of the right iliac vein by inadvertent slippage of an electrocautery hook requiring laparotomy. At follow-up, 80% of the parents were unable to identify the scars after microlaparoscopy.
Conclusion:
MAPT is a safe and practical procedure regardless of age or previous surgery.
Introduction
The aim of this prospective study was to report our early experiences with and surgical outcomes of microlaparoscopy-assisted transanal pull-through for HD in children.
Methods
Starting in 2005, we conducted a prospective, nonrandomized feasibility study to introduce the microlaparoscopic approach (the exclusive use of 2-mm instrument sets and miniscopes less then 2.5 mm in diameter) for the pull-through procedure in children with HD.
Children with HD, considered for colonic resection, were randomly assigned to the microlaparoscopic approach according to the availability of the miniscope and a consulting surgeon experienced in microlaparoscopy.
Preoperative diagnoses were based on typical clinical manifestations (constipation requiring regular enemas, events of toxic colitis in newborns and infants) with X-ray findings of a narrow distal segment, a transitional zone, and an upper proximal dilated segment detected on contrast enema studies of the rectum and colon. Prior to the pull-through procedure, the diagnosis was confirmed initially by endorectal full-cut biopsy, and the length of the aganglionic colon segment was identified by seromuscular biopsy obtained laparoscopically, if required.
The consulting surgeon described the difference between standard laparoscopy and microlaparoscopy to all parents and obtained fully informed consent from them. All procedures except for one were carried out by the first author or by fellows under his supervision.
All procedures were performed under general anesthesia and endotracheal intubation, and the abdominal part was documented by video recording. All data were prospectively collected and retrospectively rereviewed for this report. All patients were followed up weekly for up to 8 weeks after surgery and every second week for up to 4 months at regular outpatient visits.
Surgical technique
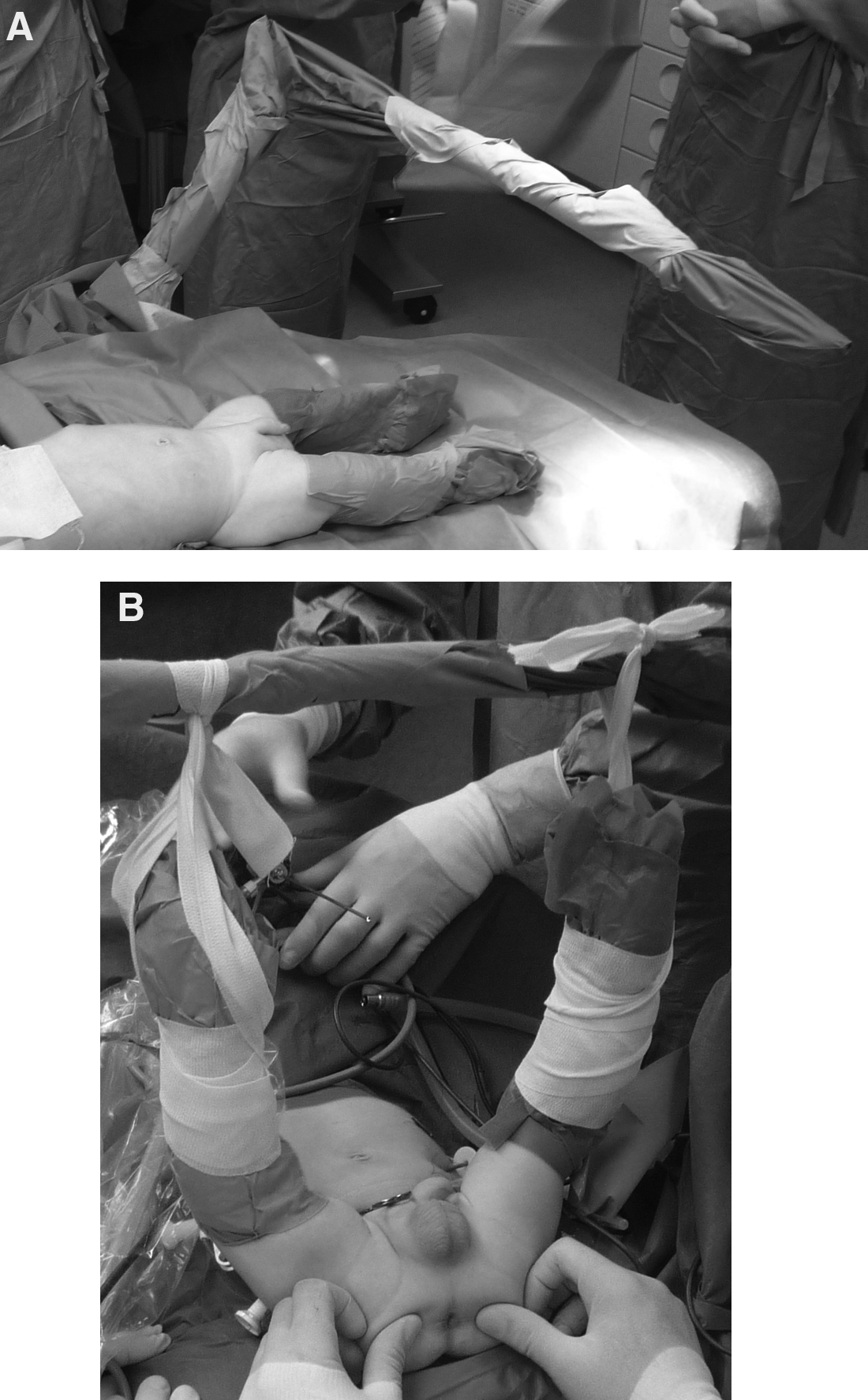
The patients were prepared and draped in a position intraoperatively changeable between the supine and the lithotomy position. To initiate the microlaparoscopic part of the procedure, the children were positioned supinely and moved to the lithotomy position with the pelvis elevated and both legs hanging up on an L-shaped bar above the pelvic area for the subsequent transanal dissection (Fig. 1A, B). Urinary catheterization was routinely performed.
A Veress needle was introduced into the abdominal cavity at the right lower abdominal wall. A CO2 pneumoperitoneum was established with an initial flow of 0.3 L/minute (to ensure proper placement of the Veress needle), which was subsequently increased to 1 L/minute. A maximum intraperitoneal pressure of 12 mm mercury was established. The Veress needle was replaced by a miniport (Autosuture MiniPort, 2 mm, short trocar length; United States Surgical Corp., Norwalk, CT), and a 1.9- or 2.4-mm 0° scope (Storz, Tuttlingen, Germany) was introduced. The 2.4-mm scope (Storz; product no.: SN 26005 AA) was developed in cooperation with the first author of this manuscript specifically for use by the microlaparoscopy study group at our department. After performing diagnostic laparoscopy, under direct visualization, two working miniports were placed lateral cranially and caudally to the scope at the right iliacal fossa and at the upper abdominal wall (at the umbilical level for the older children and 2 cm cranially to the umbilicus for the infants) (Fig. 2). To retract the descending colon, either a 2-mm grasper was introduced through the left upper lateral abdominal wall or two monofilament stay sutures were placed directly through the abdominal wall and grasped extracorporeally.

Photograph of the abdomen demonstrating the miniport positions at the end of the procedure.
In a few initial cases, seromuscular colon biopsies were taken for immediate histopathological examination to identify the aganglionic colon segment.
A window on the sigmoid mesentery was created using a monopolar cautery hook (Fig. 3), and the mesocolon was dissected up to 5 cm orally to the transitional zone. Next, dissection around the rectal wall was performed circumferentially down to the pelvis under the peritoneal reflection approximately 2 cm anteriorly and to the level of the coccyx posteriorly.

View through the 2.4-mm scope of the sigmoid area; a window on the sigmoid mesentery is created using a monopolar cautery hook.
After performing microlaparoscopic colon dissection and mobilization, the abdominal cavity was desufflated, but the trocars were left in position. The lithotomy position was carried out by moving the L-bar cranially for the transanal dissection, anal retraction was performed using perianal stay-sutures. To make mucosal dissection easier, submucosal injection of a saline water/adrenalin mixture was performed, and the mucosum was incised circumferentially 0.5–1 cm above the dentate line using a monopolar cautery needle. Submucosal dissection was carried out proximally until the peritoneal cavity was reached, and the rectal muscle was then incised circumferentially. The dissected colon segment was pulled through and transected on the point marked during the prior microlaparoscopy (Fig. 4), and anastomosis was performed using absorbable monofilament sutures. At the end of the procedure, the patient was positioned supinely again, and a control microlaparoscopy was carried out to confirm the nonrotated position of the colon, to identify possible twisting of the bowel and to explore the site for possible persistent bleeding.

Photograph of the resected specimen showing the transitional zone in the upper part of the picture.
Results
A microlaparoscopy-assisted pull-through procedure for HD was performed in 16 children (10 boys, 6 girls). Their ages ranged from 1 month to 2 years (average: 5.7 months). Six patients had previous abdominal surgery, including laparotomy and colostoma placement, because of events of toxic colitis (3) and leveling laparoscopic biopsy (3). Five children suffered from significant colitis preoperatively. In 8 children, an intraoperative leveling biopsy was performed (totally 11 children with leveling biopsies). The length of the resected colon segment was up to the left colonic flexur in 5 children and up to the middle of the descending colon in 4 cases. A resection of the sigmoid-descending segment was performed in 7 children. The average operation time was 185 minutes (range: 120–330 minutes). There was never a need to replace the miniscope with a 5-mm laparoscope. Conversion to open surgery was required in only 1 child and was the only serious intraoperative complication that occurred in this series: a minor injury of the right iliac vein by inadvertent slippage of an electrocautery hook required subsequent laparotomy. The occurrence of this serious intraoperative complication was surgeon related and not because of the torque required on the small instrument. In this series, no intestinal perforation, no anastomotic fistula formation, and no fecal incontinence occurred. There was minimal blood loss during the surgery. In the initial 5 cases, a 1.9-mm cystoscope or a 2.4-mm arthroscope was used for visualization. In the remainder, a newly developed 2.4-mm miniscope was used for visualization.
Intra-abdominal illumination and visualization of the site was sufficient in all cases.
Oral intake of clear fluids was started 24 hours after surgery, and the patients advanced to formula on the third day. The mean hospital stay was 7.8 days (range: 5–11 days). Anal dilatation was begun during the first regular outpatient visit at 14 days after the surgery and continued for 2–3 months in all patients.
For this report, a follow-up, including clinical examination and ultrasound examination of the colon, was performed for all children. The parents were interviewed to assess cosmesis and postoperative events occurring after the regular outpatient visit period. Follow-up ranged from 1 to 35 months. Two children suffered from severe colitis that required inpatient treatment at pediatric wards in the first year after surgery. Three children suffered from repeated constipation in the first 8 months postoperatively, but this did not continue beyond 1 postoperative year. In one of these children, a remicrolaparoscopy was performed 11 months after the surgery, and colonic biopsies were obtained to exclude neuronal intestinal dysplasia. In 2 other children, bilateral symptomatic inguinal hernias were treated microlaparoscopically in the follow-up time. In all 3 children with re-microlaparoscopy, there were no intestinal adhesions noted during the second procedure.
At follow-up, 80% of the parents were unable to identify any of the former 2-mm trocar insertion sites in the abdominal wall. The abdomens of the children appeared scarless (Fig. 5). All parents were strongly satisfied with the assessed cosmesis. One of the children with a bilateral inguinal hernia was admitted to our department explicitly because of the parents' wish to perform the herniorrhaphy microlaparoscopically. The parents of this child refused a prior attempt of open surgery for hernia repair scheduled in another hospital, even knowing that we could not guarantee a completely successful microlaparoscopic herniorrhaphy because of possible intra-abdominal adhesion after the previous colon resection and an episode of severe enterocolitis postoperatively.

The same child, as documented in Figure 2, at 6 months after surgery with a visually scarless abdomen.
Discussion
In 1994, laparoscopic access for mesocolon dissection in children and infants during a Duhamel procedure was first described by Smith et al. 1 Since then, laparoscopy-assisted transanal pull-through techniques for HD have become widely accepted procedures. The benefits of laparoscopic access have been described as reduced traumatization, better visualization of the intra-abdominal anatomy during the pull-through procedure, and superior cosmesis postoperatively.2,11,15 Various techniques and different modifications have been described with the goal of improving surgical outcomes.2–11 Additionally, a debate has been raised about the necessity of an additional laparoscopic approach during the pull-through procedure. The so-called natural orifice transluminal endoscopic surgery (NOTES) access in newborns during the pull-through procedure, introducing 5.5-mm trocars for the 5-mm laparoscope and instruments transanally into the peritoneal cavity, 16 and transumbilical minilaparotomy 17 for colon dissection have been reported. Obermayr et al. 18 reported the use of minilaparotomy through a Pfannenstiel incision to complete colon resection during transanal endorectal pull-through in children with long-segment HD. Technically, the pull-through procedure, which keeps the surgery exclusively transanal, is reported to be associated with possible overstretching of the anus, excessive and demanding handling within the anal canal, and tension traction of the colonic and mesocolonic structures.18,19 In a retrospective study reported by Pratap et al. 19 of 65 patients who underwent transanal pull-through, inadvertent full-thickness mobilization of the rectum occurred in 3 patients (4.6%), retraction and bleeding of colonic mesenteric vessels occurred in 2 (3.7%), difficulty in mobilizing intraperitoneal colon occurred in 1 (1.5%), perianal excoriation occurred in 22 (34%), increased stool frequency occurred in 20 (31%), and anal stenosis occurred in 3 (4.6%).
Previously, we used a 5-mm scope inserted through the right lateral abdominal wall for visualization during the laparoscopic part of sigmoid colon resection for HD. Since 2005, the microlaparoscopic approach was introduced at our department for various procedures, and it was successfully used instead of conventional laparoscopy in children.12–14
After having gained experience in microlaparoscopy, in a prospective feasibility study, we began to perform the colon mobilization and dissection for HD using 2-mm instruments and miniscopes exclusively.
In the reported series, no intestinal perforations were detected, no anastomotic fistulae formed, and no fecal incontinence occurred. There was minimal blood loss during the surgery, and the visualization of the peritoneal cavity was sufficient in all cases. Thus, our results show that primary microlaparoscopy-assisted pull-through is not associated with any early postoperative complication, which is in accordance with other reports that showed low rates of early postoperative complications using the conventional laparoscopic approach2,11 and using open or transanal approaches.3–10 In this series, the only serious intraoperative complication that occurred was an injury of the right iliac vein by inadvertent slippage of an electrocautery hook that required laparotomy. This severe intraoperative complication was defined as surgeon-related and not as surgical approach-related by an independent reviewer of the intraoperative video recording.
Regarding late postoperative complications in our series, 2 children suffered from severe colitis requiring inpatient treatment in the first year after surgery. Three children suffered from repeated constipation in the first 8 months postoperatively, but none did after 1 postoperative year. In one of these children, a remicrolaparoscopy was performed 11 months after surgery, and colonic biopsies were obtained to exclude neuronal intestinal dysplasia. In a study reported by Liem et al. 11 about the early and late outcomes of primary laparoscopic endorectal colon pull-through leaving a short rectal seromuscular sleeve for HD in 200 children, defecation function was satisfactory in long-term follow-up, 79% of their patients had one to four bowel movements per day, and two anastomotic fistulae occurred postsurgically at 3 and 12 months. They also had 6 patients with anastomotic stenosis who responded to anal dilatation. Additionally, 9.7% of their cases had enterocolitis. In the series of transanal endorectal pull-through reported by Obermayr et al., 18 in 40% of the children examined by follow-up, an anal stenosis at the site of the colo-anal anastomosis was found. In their series, no routine dilatation program was performed postoperatively, but an anal calibration was performed under general anesthesia at 6 weeks after surgery. Anal dilatation in our series was begun during the first regular outpatient visit at 14 days after the surgery and continued for 2–3 months in all patients, which was almost the same as in the study reported by Liem and Hau, 2 in which it was begun at home 15 days after the operation and continued for 3 months. The parents in our study were introduced carefully to perform the daily dilatation at home using Hegar instruments, and it was controlled by the surgeon only during the outpatient visits.
The average operative time in this series was 185 minutes (range: 120–330 minutes). In Liem and Hau's 2 early results from 61 cases of primary laparoscopic endorectal colon pull-through for HD, the operative time in their series ranged from 95 to 210 minutes (mean: 140 minutes), and they did not have any conversions in their patients.
At follow-up, 80% of the parents were unable to identify any of the former 2-mm trocar insertion sites in the abdominal wall. The abdomens of the children appeared scarless.
Our preliminary surgical outcomes are comparable to those reported by other authors performing pull-through procedures, either laparoscopy assisted or transanally only.3–11,15–19 In our hands, conventional laparoscopic or even microlaparoscopic visualization, mobilization, and dissection of the aganglionic colon segment was a favorable tool for the treatment of HD. It allows surgeons to identify the transition zone, to visualize the complete colon, to obtain leveling biopsies intracorporeally at any time during the surgery, and to control the pull-through procedure intra-abdominally by avoiding possible twisting and bleeding that may occur in transanal pull-through. Additionally, a benefit of microlaparoscopic access that we noted in our last 8 cases was that it allowed us to perform the dissection around the rectal wall circumferentially deep into the pelvis under the peritoneal reflection approximately 2 cm anteriorly and to the level of the coccyx posteriorly. Under the magnification of the scope, the dissection could be performed keeping strictly to the rectum wall, thereby preserving the pelvic nerves and vessels. By doing so, the effect was to leave a very short aganglionic rectum cuff during the following transanal mucosal dissection. It is our impression that leaving this very short rectal cuff affected the significantly lower rates of postoperative constipation and enterocolitis in the last 8 patients. However, the sample size is too small for any conclusion yet.
The laparoscopic approach was favored in 41% of the responses in a survey performed by Keckler et al. 20 (2009) among the pediatric surgeons listed in the American Pediatric Surgical Association Directory. The microlaparoscopic approach is technically identical to conventional laparoscopy except that it uses 2-mm instrument sets and miniscopes exclusively for visualization. The advantages of microlaparoscopy are obvious: it maximally reduces access trauma and provides superior cosmesis while retaining the full efficacy of the laparoscopic technique. The incisions left by 2.5-mm ports and 3-mm instruments are almost similar if ports not used. However, in the same way as mentioned for the 3-mm instruments used directly trough the abdominal wall, our technique is possible to be performed without to use the trocars also, resulting in an incision of 1.9 mm. But, at the moment, we found that the use of miniports is comfortable in instrument handling during the surgery. Also, instead of the miniport, a 14G cannula could be used as trocar for the 1.9-mm instruments. Aiming to avoid one incision on the lateral abdominal wall, the umbilicus was used for one working trocar, occasionally. Accordingly with the continuing further refinements of our technique, the results will be reported in the next future.
The use of microlaparoscopy in children for various surgical approaches has been previously reported and discussed in detail by the first author.12–14 Additionally, in the present feasibility study of microlaparoscopic colon dissection for HD, it was demonstrated that the microlaparoscopic approach could be successfully performed in cases of previous laparotomy, colostoma placement, and laparoscopy and in subjects after severe postpartal enterocolitis episodes. Microlaparoscopy is an attempt to further minimize the access trauma of laparoscopic procedures, and we suggest that downsizing the instruments and scopes used in pediatric surgery is beneficial for infants and children.
Recognizing the pilot character of the present study and the small sample size of the continuing study, it seems that the microlaparoscopy-assisted pull-through procedure for HD is safe and practical. Larger randomized comparative studies are required to verify the possible benefits of the microlaparoscopic approach over the transanal-only approach indicated by our initial experiences.
Footnotes
Disclosure Statement
No competing financial interests exist.