
Abstract
Abstract
Benign acquired esophagorespiratory fistulas (BERFs) represent a broad spectrum of anatomic pathology presenting in a wide variety of clinical settings. These fistulas can lead to severe respiratory compromise and rarely close spontaneously. Surgical fistula closure has been the traditional therapeutic approach, but is associated with significant morbidity and mortality. The recent advent of endoscopic technologies suggests that minimally invasive procedures may offer a safe alternative to surgery for the treatment of esophagorespiratory fistulas. In this article, we present our experience in treating complex benign esophagorespiratory fistulas of diverse etiologies utilizing a primarily minimal invasive, endoscopic, or combined surgical and endoscopic approaches. Our experience demonstrates that an endoscopic-based approach is safe and technically feasible and can, potentially, spare a subset of patients from open surgery. A multidisciplinary decision-making process, based on individualized parameters, is a prerequisite for a successful outcome.
Introduction
CT, computed tomography; ICU, intensive care unit.
Case 1
A 58-year-old presented to an outside hospital for the repair of an epiphrenic esophageal diverticulum, which had recently become symptomatic. The patient underwent an open diverticulectomy via a right thoracotomy without a myotomy, which resulted in an esophageal leak originating from the staple-line repair. The patient developed a severe, persistent pulmonary infection with multiple bouts of sepsis. A barium contrast study revealed a large distal left esophago-pleural-cutaneous fistula. After 7 months of in-patient care, the patient was transferred to our center.
A laparotomy and midline sternotomy was performed and a large esophagorespiratory fistula was identified, with significant surrounding esophageal damage. The patient underwent a distal esophageal exclusion, gastric pull-through, and, finally, cervical anastamosis via an additional left cervical incision. The excluded distal native esophagus was left in situ (Fig. 1A, B). After 1 month on mechanical ventilation in the intensive care unit (ICU) and an additional month on the ward, the patient was discharged, tolerating a regular diet with an esophageal drain and feeding jejunostomy in place. Although the patient has since begun to regain weight and resume activities of daily living, at 18 months following the surgery, the patient is receiving continued medical management and is scheduled for an endoscopic ablation for persistent drainage of the excluded native esophagus.
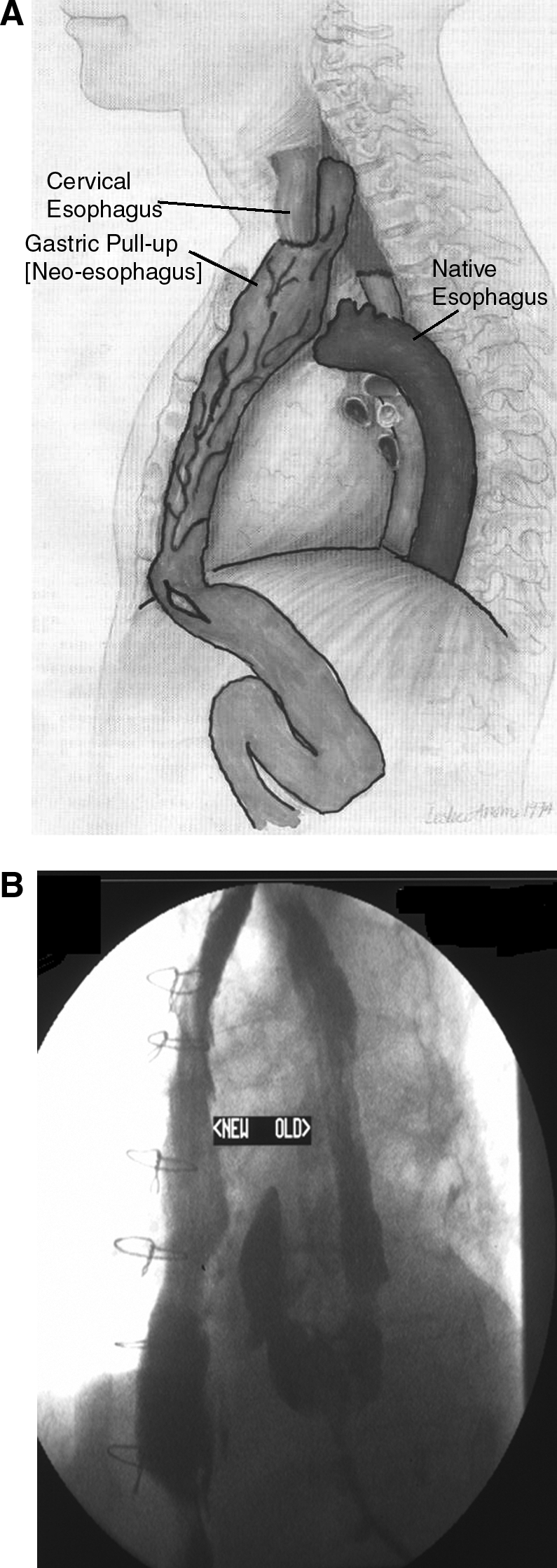
(
Case 2
A 51-year-old male with a history of a distal esophageal diverticulum and right esophagobronchial fistula status postdiverticular excision, closure of the fistula, and right lower lobectomy 7 years earlier, presented to an outside hospital complaining of a persistent, but progrssive, cough and a choking sensation exacerbated by oral intake. A computed tomography (CT) scan of the chest demonstrated the leakage of contrast material from the esophagus into a fluid collection, which continued into the bronchial tree. Endoscopy confirmed an 8-mm defect on the anterior wall of the esophagus, and the patient was taken for endoscopic repair. Following initial endoscopic cauterization of the region, using an argon laser, metallic endoclips were placed, via an endoscopic retrograde cholangiopancreatography scope, on the proximal and distal edges of the defect, thereby reducing its size to approximately 5 mm. The defect was reduced incrementally over future sessions, using additional clips and fibrin flue application, until, after a total of 5 sessions, the defect was completely closed. Three years postprocedure, the patient has had no complications and remains symptom free.
Case 3
A 40-year-old male presented to the emergency department complaining of progressive chest pain, cough, shortness of breath, and a fever 6 weeks after an uneventful laparoscopic appendectomy. A CT scan of the chest and abdomen demonstrated the esophagus draining into a mass-like structure below the carina, consistent with an abscess, with accompanying esophageal wall inflammation and mediastinal lymphadenopathy. Upper endoscopy revealed significant external compression of the left mainstem bronchus and distal esophagus. Although the abscess responded to intravenous (i.v.) antibiotic treatment, approximately 12 weeks later, while receiving i.v. antibiotic treatment for a new occipital brain abscess, the patient developed dyspnea and recurrent cough. Barium swallow revealed the presence of a left esophagobroncho fistula 30 cm from the incisors (Fig. 2), and endoscopy confirmed a 5-mm defect in the left wall of the distal esophagus. The fistula was closed endoscopically over a total of 6 sessions, using a combination of argon electrocautization and fibrin glue application, with the subsequent resolution of respiratory symptoms. Follow-up endoscopy, 6 months following repair, revealed a 1–2-mm defect in the region of the original fistula months. The patient notes the presence of a mild cough when drinking, which does not interfere with his general lifestyle. The patient is currently being evaluated for possible endoscopic reclosure of the defect with fibrin glue to reseal the defect.
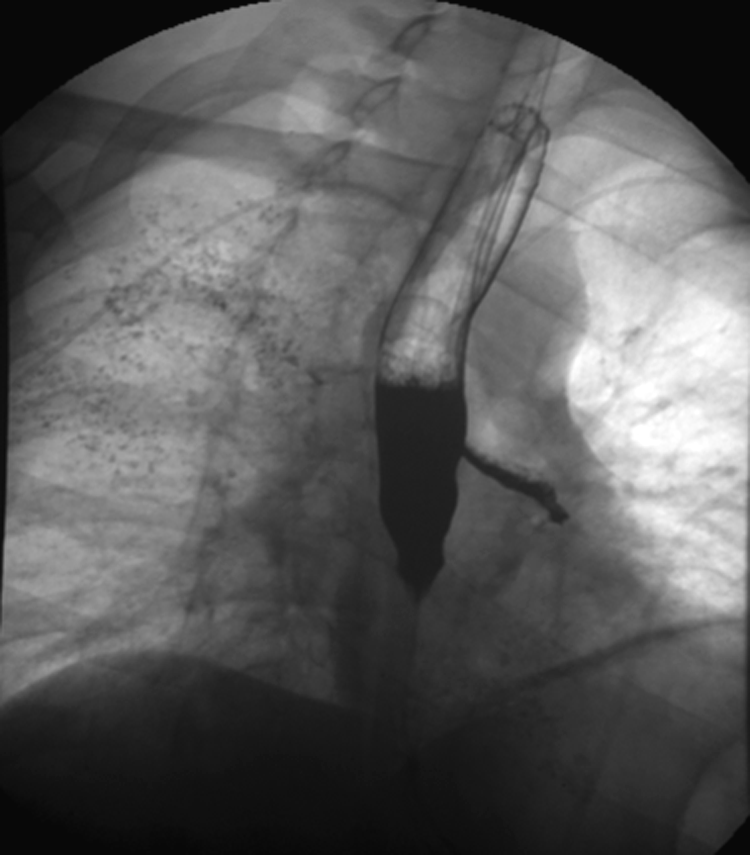
Barium swallow demonstrating leakage of contrast from the esophagus into the bronchial tree.
Discussion
AERFs are generally categorized as malignant or benign, with malignant, late-stage esophageal cancer, accounting for over 50% of all cases. Benign esophagorespiratory fistulas (BERFs) are generally either inflammatory or postsurgical in nature. 1 Both malignant and nonmalignant BERFs tend to lead to life-threatening recurrent pulmonary contamination, infection, and malnutrition. Acquired BERFs can result from a variety of etiologies, including prolonged mechanical ventilation, iatrogenic injury, trauma, prior tracheal or esophageal surgery, indwelling stents, granulomatous mediastinal infections, and AIDS. The relative incidences of the various anatomic locations vary, based on the incendiary cause.1,2 Currently, the most common cause of an acquired BERF is as a complication of cuffed endotracheal or tracheostomy tubes, presumably due to pressure necrosis of the tracheal and esophageal walls from the inflated endotracheal tube cuff. 3
Benign fistulas place the patient at significant risk for developing recurrent pulmonary infection and poor nutrition. Additionally, because the incidence of spontaneous closure of these fistulas is extremely low, reviews of the subject have emphasized the necessity of definitive repair in these cases. 4 BERFs present a particularly challenging clinical dilemma, specifically because of their potential for curability. Unlike cases of malignant fistula, where patient life expectancy is short, the repair of benign fistulas provides the opportunity for cure, making the functional, long-term recovery a critical factor in electing the therapeutic approach.
Historically, open surgery has been the treatment option of choice, when technically feasible. Nevertheless, open operative closure of BERFs is not a simple endeavor. The circumferential nature and size of the injury often necessitates tracheal resection and not just repair. The operations are long and often complex. Postoperative positive pressure ventilation carries a significant risk of anastamotic complications, such as dehiscence and stenosis, resulting in significant postoperative morbidity and a postoperative mortality rate of 8.3%. 1 Finally, because BERFs frequently occur in patients with multiple medical problems who are not ideally suited for major surgery, the risks of abstention and potential future respiratory complications must always be measured against the very present risks of operative intervention.
Case 1 described a complex patient with multiple medical problems in which we encountered this very dilemma. Because he had a very large defect with significant esophageal damage with recurrent thoracic infection requiring a washout, he was not deemed appropriate for endoscopic repair. Nevertheless, because of severe esophageal damage, direct anastamosis was also not possible. Although the patient was repaired successfully with an ingenuitive one-stage esophageal exclusion with a gastric pull-through and cervical anastamosis, he experienced a prolonged ICU and hospital course with a subsequent chronic postoperative morbidity.
In recognition of the severe and morbid nature of this repair, minimally invasive approaches have been sought to serve as an alternative to open surgery in selected cases. Tracheal stenting has been used for the palliative treatment of malignant tracheoesophageal fistulas and as a temporizing measure for patients with benign fistulas until they are medically stable to undergo surgical repair. Tracheal stenting is actually contraindicated in patients eligible for surgical repair, as the pressure exerted by the stent can lead to further esophago-tracheal injury. 5
Although there is much literature reporting successful endoscopic closure of esophageal perforations up to 2 cm using various combinations of argon electrocautery, endoscopic clips, and fibrin sealant, there only a few reported cases successful application of this technique to esophageal fistulas.6,7 Theoretically, these fistulas can be repaired endoscopically or bronchoscopically. For cases of small fistulas, which are difficult to identify, bronchoscopic visualization and interrogation can aid in localizing the esophageal defect, as was performed in patient 2. In our experience, endoscopic therapy should begin with argon electrocauterization of the tissue surrounding the defect. We have found that it not only contracts the surrounding tissue, thereby reducing the size of the defect, but it also creates a more effective surface for the fibrin sealant to adhere. Larger defects will often require multiple sessions, which may span over a few weeks, during which endoscopic clips are placed at the edges of the defect to gradually reduce the size to 2–3 mm, at which time it can be definitively sealed with fibrin sealant.
Conclusions
In conclusion, BERFs represent an uncommon, but highly heterogenous, spectrum of pathology, often with disparate presentations and divergent clinical courses. Although all benign cases should still be definitively repaired, there is no longer a single solution to these complex cases nor is there a single person who can provide it. Minimally invasive endoscopic closure can potentially spare selected patients the morbidity and mortality of open surgery. As technologic devices continue to emerge and clinicians gain experience with minimally invasive and NOTES techniques, it may not be long before endoscopic repair becomes the new standard treatment of BERFs, with alternative methods, such as open surgery, reserved for individual cases.
Footnotes
Disclosure Statement
No competing financial interests exist.