
Abstract
Abstract
Objective:
The goal of this study is to prospectively evaluate the safety of concomitant cholecystectomy during laparoscopic anti-reflux surgery (LARS).
Methods:
A total of 1000 patients underwent LARS between May 2004 and August 2009. Patients who had a LARS procedure alone were defined as group A and those who had cholecystectomy during the LARS were defined as group B. All data, including demographics, operative details, perioperative complications, and outcomes, were recorded to the prospective database. Chi-square and t-test were used for statistical analysis.
Results:
There were 934 (93.4%) patients in group A and 66 (6.6%) in group B. Cholelithiasis (n = 48) and gallbladder polyp larger than 10 mm (n = 18) were the indications for cholecystectomy. Demographic characteristics were similar among the groups. There were no mortality and conversion. The mean operating time was 50 minutes for group A and 80 minutes for group B (P = 0.0001). The mean hospital stay was 1 day for each group. The mean follow-up was 35 and 38 months for groups A and B, respectively (P = 0.195). Esophageal perforation, jejunal perforation, and pulmonary emboli were the major complications and were seen only in group A (P = 0.790). All other peroperative minor complications and postoperative dysphagia, bloating, and reflux recurrence were similar between the two groups (P > 0.05).
Conclusion:
LARS and cholecystectomy can be performed safely during the same session without increasing the rates of morbidity and recurrence of reflux.
Introduction
The recommended therapy for symptomatic cholelithiasis and polyps larger than 10 mm is cholecystectomy. However, the approach for asymptomatic patients remains uncertain. About 15%–30% of asymptomatic patients will demonstrate biliary symptoms in the future and require cholecystectomy. 3 Lund reported that 30% of men and 50% of women with untreated asymptomatic gall stones became symptomatic during a 5-to-20 year follow-up. 4 Moreover, there are studies indicating that complications associated with gall bladder stones might occur after interventions involving nonbiliary surgeries. 5
On the other hand, cholecystectomy has been reported to alter the upper gastrointestinal system motility, increase the duodenogastric/gastroesophageal reflux, and have the potential to impose reflux-related problems.6,7
The aim of this study is to prospectively evaluate the clinical results of concomitant cholecystectomy performed in the same session with laparoscopic anti-reflux surgery (LARS). This paper represents a single surgeon's experience from a single center, excluding his learning curve.
Materials and Methods
The study was conducted at our anti-reflux therapy center, which is a specialized tertiary referral center for the diagnosis and treatment of GERD. All patients referred to us with probable GERD were comprehensively evaluated. Gastroscopy at our center with biopsies is a routine procedure after a detailed history is obtained. PH meter was also a routine procedure in patients without esophagitis. A definite diagnosis is established according to the patient's history (typical symptoms responding to proton pump inhibitors) in addition to presence of esophagitis at gastroscopy. Biopsy proven Barrett's disease or a DeMeester score of >14.7 and/or symptom index >50% at PH meter analysis were also conclusive evidence for GERD in symptomatic patients seeking surgical care. Therefore, patients were classified as either erosive or nonerosive GERD. Extra esophageal symptoms were carefully recorded. Indications for surgery were quite straightforward. Any patient having a definite diagnosis of GERD with symptoms of >1-year duration was a candidate for LARS. Patient preference was the rule in choosing a surgical approach instead of continuing medication and diet. All patients underwent upper gastrointestinal ultrasound (US) preoperatively.
Groups
Group A was comprised of 934 patients who received LARS alone and represents the control group.
Sixty-six patients who exhibited gallstone (n = 48) or gallbladder polyp larger than 10 mm (n = 18) in the preoperative US were informed about their gallbladder pathologies before surgery, and the likely outcomes of cholecystectomy that can be performed in the same session were discussed. Twenty-five out of 48 of these patients had a previous history of gall stone related problems (i.e.: biliary colic or previously elevated enzyme levels). None of these patients were jaundiced or had acute cholecystitis. Twenty-three patients did not have any biliary symptoms. The age range of these 23 patients varied between 19 and 39 years. In this sub-group of patients, natural course of asymptomatic gallbladder stones were comprehensively discussed. As they were already undergoing a planned laparoscopic procedure, addition of cholecystectomy was patient preference in this subgroup of young patients. All the patients provided written consent for removal of their gallbladders in the same session, and those 66 patients (Group B) constituted the study group.
Gastroscopy
The Olympus CV 260 was employed for upper gastrointestinal endoscopy. All endoscopic procedures were carried out in the presence of an anesthesiologist. Before achievement of deep sedation during spontaneous breathing with propofol 1–2 mg/kg, the patients were premedicated with midazolam 0.15 mg/kg and fentanyl 1 μg/kg, while monitoring the vital signs. The endoscopic assessment of esophagitis was done according to the Los Angeles classification. 8 Hiatus defects larger than 5 cm were recognized as large hiatal hernia. In all endoscopies, a punch biopsy was routinely obtained from the antral mucosa of the stomach. Biopsies were endoscopically acquired from the lower end of the esophagus from patients demonstrating Barrett's esophagus.
Manometry
Manometric examination of the esophagus was also a routine procedure before performing LARS. The UPS 2020 stationary GI (MMS Enschede) device with four lumen water-perfused system was used. By “stationary pull-through technique,” the length and localization of the lower esophageal sphincter (LES) were determined. The results were analyzed with a computer program; and the LES pressure, average esophageal contraction pressure, percentage of LES relaxation, and esophageal peristaltism were recorded.
24-hour pH meter
Orion II and Ohmega (MMS Enschede) devices were employed. A double-sensor catheter was used after calibration with pH 1.07 and 7.01 solutions. These results were analyzed and evaluated with a computer program.
Ultrasonography
The hepatobiliary system was evaluated with a Siemens Antares™ (Siemens Medical Solutions USA Inc.) device by using 2–4 Mhz probes.
Surgical technique
All operations were done by the senior author (M.A.Y.) and the series does not contain his learning curve including both operations. All patients were admitted on the day of surgery and underwent an anti-reflux procedure after an overnight fast. High-resolution video recordings of all operations were also collected for possible future analysis of technical details. The surgical procedure of choice was based on the preoperative manometric examination and severeness of the disease. Partial 270 degrees fundoplication, namely Toupet's operation, was the procedure of choice in patients having mean esophageal contraction amplitudes <20 mmHg. Partial fundoplication was also performed whenever there was a technical difficulty to secure a floppy full wrap, that is, inability to cut short gastric vessels or difficulties in dissection. Crural repair with silk sutures, deployment of a V-shaped monofilament polypropylene graft (Prolene; Ethicon, Ltd.), cutting short gastrics with LigaSure™ (Valleylab), and a floppy 1.5–2 cm wrap done over a 60 F bougie were the preferred techniques for Nissen's procedure. Usage of grafts for hiatal repair became a routine early in our experience. Drains were rarely used at the surgeon's discretion. An additional 5 mm trocar from the right upper quadrant was applied in patients scheduled for cholecystectomy (Fig. 1). This was the sole difference between the trocar placements in both groups. Our cholecystectomy technique has been previously outlined.9,10 Videos of patients in group B were watched and attention was paid to find out whether any gallbladder perforation during cholecystectomy had occurred or not. Any graft placement in those patients who had gallblader perforation was noted.
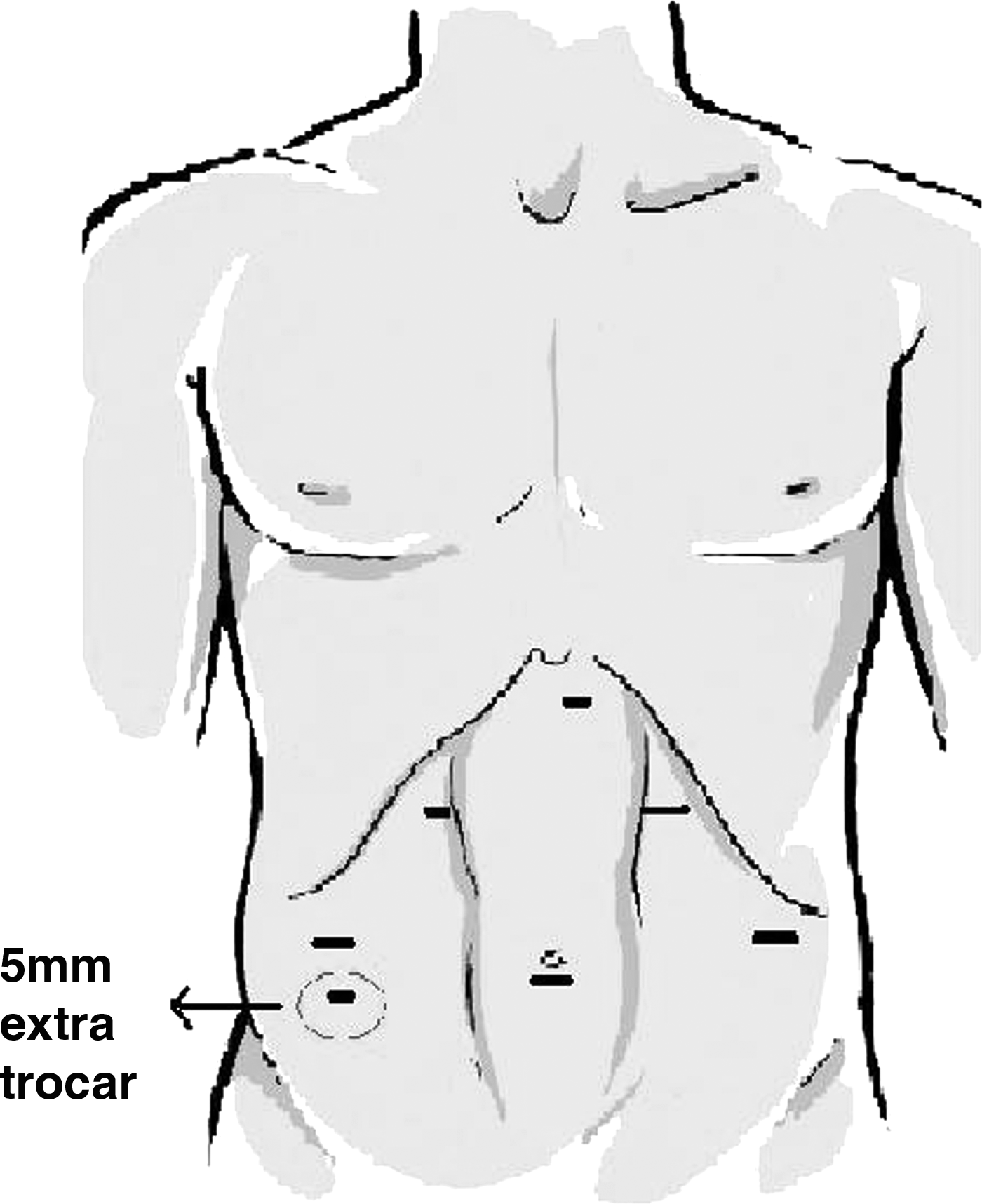
Trocar placement in cholecystectomy group.
Postoperative care
All patients were hospitalized for 1 day unless specific problems occurred. All patients were seen 1 week and 2 months after surgery and yearly thereafter. Patients who were not able to come for yearly visits were contacted by phone and asked their symptom status. No attempt was made to perform gastroscopy or pH meter testing during these controls unless the patient was symptomatic or had Barrett's disease.
Study design and statistics
All data, including demographics, operative details, operative/postoperative complications, and early/late outcome, were recorded to the prospective database using SPSS software (SPSS for Windows 11.5; SPSS). Chi-square and t-test were used for statistical analysis; P < 0.05 was recognized as statistically significant.
Results
A total of 1000 patients underwent a laparoscopic anti-reflux operation from May 2004 to August 2009. Sixty-six (6.6%) of those patients were also subjected to cholecystectomy in the same session. None of the cases were converted to open procedure and there was no mortality. Demographic characteristics of the patients are outlined in Table 1.
BMI, body mass index.
Preoperative findings of the patients are shown in Table 2. Apart from the presenting symptoms of the patients, preoperative findings did not differ between the two groups. Group B demonstrated more typical symptoms such as isolated retrosternal burning and/or regurgitation. Fifty-eight patients were initially subjected to cholecystectomy, whereas fundoplication procedure was performed first on eight patients in group B.
Significantly different between the groups.
LES, lower esophageal sphincter.
Perioperative findings are shown in Table 3. The mean operation room time was significantly longer in group B (80.51 ± 31.68) compared with group A (49.93 ± 21.53). Discharge times and frequencies of graft and drain usage were similar in both groups. Bougie usage was more frequent in group A. Group B showed no complications associated with cholecystectomy. In 13 cases, the gallbladder was perforated during cholecystectomy and bile was spread over the abdominal space, but stayed limited within the cholecystectomy area. Vigorous irrigation with saline and aspiration was performed in these cases. Hiatoplasty with grafts was performed on five of those 13 patients. None of those 5 patients demonstrated any complications. Further, there were no graft-related complication in any of the “grafted” patients during the entire follow-up.
Significantly different between the groups.
Esophageal perforation, jejunal perforation, and pulmonary emboli were the major complications and were seen only in group A. In one patient, a diagnosis of pulmonary emboli with lower extremity doppler US and pulmonary angiography followed by immediate subcutaneous heparin for a week and oral anticoagulation for 1 year thereafter was needed, and she recovered without sequelae. Esophageal perforation resulted from the bougie insertion and was immediately diagnosed and laparoscopically repaired with success without any further sequelae. In one patient, jejunal perforation resulted from umblical trocar insertion and became evident 10 hours postoperatively. This patient was operated the day after LARS with laparotomy and recovered uneventfully. These three major complications and the rest of the minor complications did not show a statistically significant difference between the groups (Table 4).
The mean follow-up of the present series was 36 months. Long-term follow-up and recurrence data are presented in Table 5. Dysphagia, resolving spontaneously or requiring reintervention, was evenly distributed between the groups. Acute dysphagia, typically occurring during the immediate postoperative period, was easily diagnosed by no passage of opaque liquids in upper gastrointestinal series and occurred in nine patients of group A. All 9 patients had undergone a Nissen procedure and all were treated by early reoperation laparoscopically. All nine Nissen operations were converted to Toupet within 1 to 7 days postoperatively with enlargement of the hiatus in two. Five cases were operated on the next day after the Nissen's procedure and 4 were operated on after rehospitalization of the patients. All early reoperated patients had an uneventful recovery without any dysphagia thereafter.
A total of 32 patients were rehospitalized. Eight of them were due to reoperations (4 late, 4 early). The other 24 patients were rehospitalized due to multiple other reasons such as acute gas bloating, chest/abdominal pain, mediastinal/subcutaneous emphysema, or anxiety and were treated with medical therapy.
In addition to perioperative complications, a total of 8 patients (all in group A) had esophageal dilation postoperatively. As for the postoperative dysphagia, bloating, and reinterventions, there were no significant differences between the groups (Table 5).
Discussion
Gallbladder diseases and GERD are the most common diseases affecting the digestive system. The prevalance of GERD in Western countries has been reported to be around 20%. 2 In the United States, the number of patients having a gallbladder stone is estimated to be 15–20 million, and 0.5%–11% of all cholecystectomy cases reveal a gallbladder polyp. 11
Gallbladder polyps are usually asymptomatic and are frequently diagnosed as a result of abdominal US performed due to other reasons. 12 Although gallbladder polyps do not have a definite treatment algorithm, cholecystectomy is the preferred option in cases with sessile polyps larger than 10 mm that pose a risk for malignancy, and malignancy prevalence among those cases is known to be around 37%. 13 The fact that gall bladder cancers constitute one of the most aggressive malignancies increases the importance of precancerous lesions.
As the utilization of US in the evaluation of abdominal disorders increased, the number of patients with asymptomatic gallbladder stone increased as well. Approximately 50%–70% of patients with cholelithiasis are known to be asymptomatic during the diagnosis. 14 This is also in accordance with the number of asymptomatic patients in the present series. Although age dependent, the risk of developing a biliary symptom is 15%–30% among asymptomatic patients. 3 Lund reported that 30% of men and almost half of women will become symptomatic 5 to 20 years after the diagnosis. 4 Therefore, the cumulative risk of developing obvious symptoms and serious complications is certainly much higher in younger aged patients as those reported herein. The recommended treatment of symptomatic gallbladder stone is surgery; however, the approach to the asymptomatic patients is controversial. Although many patients remain asymptomatic, the likelihood of serious and life-threatening complications such as acute cholecystitis, acute pancreatitis, and jaundice, as well as the elevation of surgical risk with the advancing age, have led some surgeons to prefer elective cholecystectomy. Along with the advent of laparoscopic surgical technology, this preference has peaked and the number of patients receiving cholecystectomy has shown a significant increase worldwide owing to the minimally invasive nature of the procedure. Between 1989 and 1993, the percentage of cholecystectomy treatment among the 45–64 age group elevated from 18.7% to 25%.15,16 The reasons behind that rise are the studies proving the safety of laparoscopic cholecystectomy with minimal morbidity and 0.1%–0.5% mortality 17 along with the evidence pointing out its clear superiority over open surgery. It should, however, be noted that the mortality of elective cholecystectomy increases with age. In patients older than 70 years, emergency cholecystectomy is associated with a 20-fold increase in mortality rates. 18
Another important point is the likelihood of nonbiliary surgeries increasing the complications associated with the presence of asymptomatic gall bladder stones in the early postoperative period. Juhasz et al. published the results of 305 patients with asymptomatic gallbladder stone who received colorectal surgery. 5 One hundred ninety-five patients (64%) were subjected to incidental cholecystectomy, whereas 110 (36%) patients were spared. Between the two groups, no difference was reported with regard to operative mortality or morbidity. In the group that was spared from cholecystectomy, 16 (14%) patients developed postoperative biliary symptoms, and two patients received cholecystectomy along the course of their hospital stay due to development of acute cholecystitis. In another study, 9 of 11 patients who underwent aortic aneurism resection were reported to develop cholecystitis within a mean period of 2.9 years. 19 Thompson et al. reported the development of biliary symptoms within 6 months in 16 of 23 patients who had asymptomatic gallbladder stone and experienced laparotomy for various reasons. 20 There is no information as to why a large number of asymptomatic gallbladder stones become symptomatic after nonbiliary surgeries.
On the other hand, there are studies which claim that cholecystectomy reduces upper gastrointestinal motility and might cause gastroesophageal reflux or aggravate the already existing reflux.7,21,22 Jazrawi et al. showed increased prevelance of gastroesophageal reflux and esophagitis. 7 In a histopathologic and DNA flow cytometric study, stomach mucosa has been shown to be affected from duodenogastric reflux after cholecystectomy. 21 Another study demonstrated an elevated duodenogastric reflux after Tc-99 infusion and gastric aspiration along with 24-hour antroduodenal manometry. 22 However, Manifold et al. reported no elevation in duodenogastric or gastroesophageal reflux after 24-hour gastric pH-meter and bilirubin monitorization. 22 There is still an ongoing discussion on this issue.
The aim of our study was to evaluate the probable risks of additional cholecystectomy in patients undergoing LARS. As discussed above, it is not very infrequent for a surgeon to confront with a patient requiring both cholecystectomy and LARS. Therefore, it would be very interesting to know whether the “additional” procedure increases the surgical risk or not.
It should be noted that all patients in the cholecystectomy group were about to undergo a laparoscopic procedure, namely LARS, which is in the close vicinity of the gallbladder. Additional surgical stress was only a 5 mm extra trocar insertion and slightly increased operating time. Since no major complication occurred in the cholecystectomy group and all minor problems were evenly distributed among the groups, as well as no delay in discharge times was noted, the present series clearly shows the feasibility of addition of elective cholecystectomy to LARS.
Nevertheless, among 66 patients undergoing cholecystectomy, only 23 were asymptomatic and the rest had clear indications for cholecystectomy. Whether cholecystectomy is indicated in this subgroup of patients is still a controversial issue and beyond the scope of our study. However, it should be remembered that a number of these considerably young patients are saved from a subsequent and, probably, more formidable operation, as the natural course of asymptomatic gallbladder stones is very well known as discussed above.
There are a few studies in the literature that focus on this subject. Pozo et al. reported safety of elective cholecystectomy during anti-reflux surgery for uncomplicated gallbladder stone disease among a low-risk patient population. 23 Differing from our study, that was a retrospective evaluation between cholecystectomy alone versus cholecystectomy + LARS. As in our study, no differences in any compared parameters were found excluding the operating time. In another study, Klaus et al. performed LARS on 1065 patients while also doing incidental cholecystectomy in 67 of them and reported no increase in the postoperative morbidity in a retrospective analysis. 24 No complications associated with cholecystectomy were found in the study, and conversion to open surgery was required only in one patient due to cystic artery hemorrhage. Differing from our series, postoperative bloating was found to be significantly elevated in the cholecystectomy group.
There is no algorithm that indicates which procedure should be the initial procedure in the treatment of GERD and concurrent cholelithiasis. Hiatoplasty without graft may be preferred to prevent the probability of an infection in the presence of diffuse abdominal sludge and/or stone contamination associated with a perforated gallbladder. In the present study, 58 patients initially received cholecystectomy, whereas 13 patients developed gallbladder perforation. In all patients, contamination was limited within the cholecystectomy area and grafting was used in hiatoplasty of 5 of these 13 patients. None of the patients exhibited a complication associated with the grafts. We still think that cholecystectomy should be the first operation and depending on the contamination status, a choice against the deployment of a graft may be preferred.
In conclusion, the probability of encountering a patient presenting with both GERD and gallbladder pathology is not low for a surgeon. Both diseases can be safely treated in the same session without increasing the morbidity and mortality. Therefore, considerable number of subsequent operations that may even be more risky in the future can be eliminated.
Footnotes
Disclosure Statement
No competing financial interests exist.